
Abstract

To the editor,
Benign lesions or malignancies in the head and neck can invade or compress the trachea and cause severe airway obstruction with subsequent respiratory failure. Patients with such urgent situations are sometimes encountered in the emergency department. In the past, prompt consultations for emergent tracheostomy was the primary choice for these patients. However, both surgeons and patients may experience great suffering during the procedure. Herein, we would like to share our experience regarding airway management in a patient having thyroid metastasis complicated with tracheal compression.
A 55-year-old female (height 154 cm; weight 50 kg) presented to the emergency department because of dyspnea for 2 days. She had a history of left-sided breast cancer experiencing modified radical mastectomy and concurrent chemoradiotherapy. The physical evaluations revealed palpable and solid masses at the front of the neck and stridor on expiration. Computed tomography scans demonstrated that hypodense lesions occupied bilateral thyroid glands, leading to tracheal compression with a minimal diameter of 7 mm (Figure 1). Initially, our chest surgeon was consulted for evaluation of awake tracheostomy, but the extension of thyroid masses significantly increased the difficulties in performing the procedure. Moreover, the patient strongly rejected the surgery in awake status. Then, we were consulted for advanced airway management due to the impending complete airway obstruction and respiratory failure.
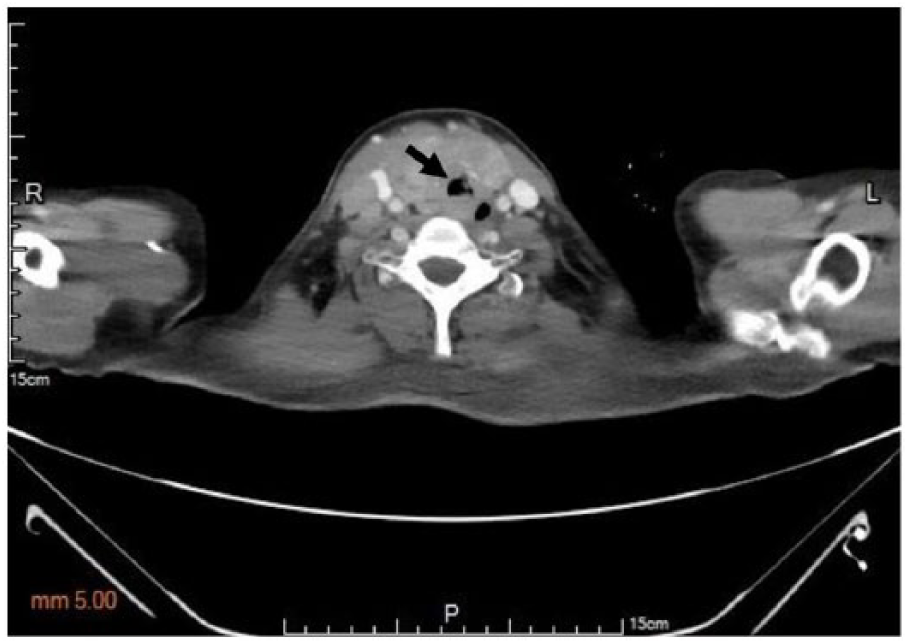
Multiple hypodense lesions in bilateral thyroid glands with tracheal compression in computed tomography scans (arrow; measured minimal diameter: 7 mm).
With careful evaluation and discussion, awake fiberoptic nasal intubation was recommended in this case. Following light sedation with intravenous 2 mg midazolam and topical anesthesia in the upper airway using 2% lidocaine spray, a small size of nasotracheal tube (Mallinckrodt™ Nasal RAE Cuffless Tracheal Tube; I.D./O.D., 5.0/6.9 mm) was selected to perform the initial attempts via the nasal route under the guidance of the fiberscope (Olympus PortaView® LF-DP; O.D., 3.1 mm). However, the optimal insertion depth could not be achieved due to insufficient length below the curvature of the inserted tube. Therefore, an oral endotracheal tube (Shiley™ Cuffed Basic Endotracheal Tube; I.D./O.D., 5.0/6.8 mm) replaced the traditional nasotracheal tube, and was successfully placed and fixed at the mark of 23 cm. Considering the connector of the oral endotracheal tube close to the patient’s nasal ala and the possibility of prolonged nasotracheal intubation, we connected a proximal part of the initial nasotracheal tube, which was cut at the curvature (the mark of 18 cm), to the end of the oral endotracheal tube outside the nostril (Figure 2), based on the method introduced previously by Cherng and Chen. 1 After establishing a relatively safe and reliable airway, the patient received total thyroidectomy and tracheostomy. The result of tissue pathology revealed metastatic adenocarcinoma originated from breast cancer. Therefore, our case started a new course of chemotherapy afterwards.

The modified nasotracheal tube has two components consisting of an oral endotracheal tube (the distal part) and a preformed nasotracheal tube (the proximal part).
According to the current practice guidelines 2 for difficult airway management by the American Society of Anesthesiologists, invasive airway access is a reasonable strategy in expected difficulties of intubation and ventilation. In a retrospective study, Sagiv et al. 3 demonstrated that awake tracheostomy was considered as an appropriate airway management strategy for patients with airway obstruction and possible difficult intubation resulted from various etiologies of head and neck. However, awake tracheostomy should be avoided in some cases with inflammation of the neck skin or lesions located at the incision site just as in the present case. In these scenarios, awake fiberoptic intubation can be an efficacious alternative strategy.
Awake fiberoptic nasal intubation is a technique allowing a flexible fiberscope through the nasal route to provide a clear visualization of vocal cords and subsequent passage of an endotracheal tube into the trachea under direct vision. When awake nasal intubation is indicated, we often encounter great difficulties in size selection of nasotracheal tube because the smaller size usually stands for the shorter length below the curvature of the tube. However, choosing an endotracheal tube with the smaller size to avoid trauma or bleeding in patients with partial airway obstruction may be necessary. Because inadequate tube length may lead to failure to rescue the airway impending obstruction, this disadvantage of smaller nasotracheal tubes must be overcome.
Compared with traditional nasotracheal tubes, an oral tracheal tube with the same size of inner diameter has more adjustable length in the nasal route (Figure 3). Therefore, we can easily control the insertion depth to achieve the appropriate distance above the carina. In addition, the proximal part of the nasotracheal tube, connected to the oral tracheal tube, can be adjustable to the desirable direction of tube angulation and then prevent against nasal necrosis due to excessive pressure between the surface of the nasal ala and the nasotracheal tube. 1 In conclusion, the modified nasotracheal tube can not only be applied in long-term head and neck surgeries, but can also be an effective and safe alternative airway management for patients having airway obstruction.
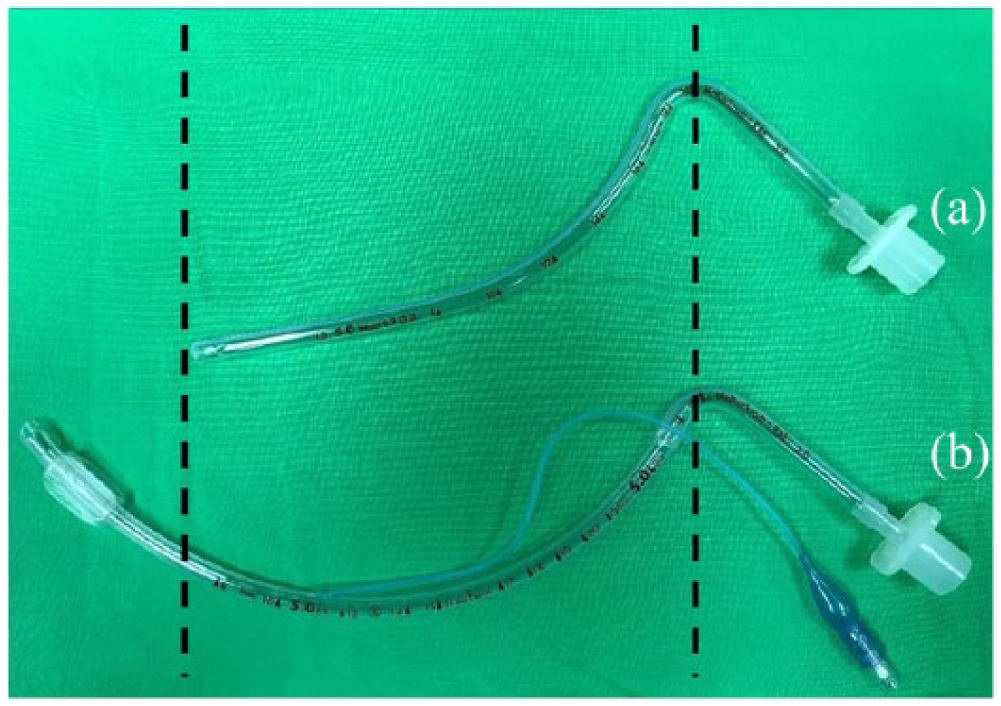
(a) Standard nasotracheal tube. (b) Modified nasotracheal tube, which is significantly lengthened, but has the same inner diameter as the standard tube.
Footnotes
Acknowledgements
We thank the patient for signing the informed consent for publication.
Author contributions
W-H.C., C-H.C., C-C.Y., and W-C.T. contributed to writing the manuscript. W-H.C., H-K.H., and W-C.T. contributed to clinical care. All the authors read and approved of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials from the patient’s medical record.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee of the institute.
Informed consent
We certified that the informed consent was obtained. The patient has given her consent for her images and other clinical information to be reported in the journal.
Human rights
All we have done obeyed the patient’s basic human rights.