
Abstract
Introduction:
Allergic acute myocardial infarction with ST-segment elevation is rare, and vasoconstrictor mediators released from mast cells are responsible for its pathogenesis. Several medications have been reported to lead to acute myocardial infarction with ST-segment elevation, as a part of systemic allergic reactions and this entity is known as Kounis syndrome (KS).
Case presentation:
We presented a patient with recurrent KS who had no allergic reactions, except coronary spasm after parenteral diclofenac administration. First, she experienced anterior myocardial infarction with ST-segment elevation after administration of diclofenac 2 years ago. The second presentation was acute inferior-posterior myocardial infarction with ST-segment elevation with atrioventricular complete block leading to cardiogenic shock. She had no significant coronary stenosis responsible for each myocardial infarction with ST-segment elevation. However, she had a catheter-induced coronary spasm of non-dominant right coronary artery. She was considered to have a recurrent allergic myocardial infarction with ST-segment elevation due to parenteral diclofenac usage and treated with a calcium antagonist, statin, and dual antiplatelet agent.
Discussion:
KS can manifest as same as acute coronary syndrome. All drugs or any allergen can cause this event.KS had three variants but In all three conditions, treatment is antithrombotic or vasodilatator regime.
Conclusion:
As atherosclerosis events on coronary, allergic coronary events also may recurs. However, unlike the literature, our case is differentiated by recurrence of similar events in different coronary vessels.
Introduction
Kounis syndrome (KS) is defined as hypersensitivity coronary disorder induced by environmental exposures, drugs, conditions, and stents. It was first described, by Kounis and Zavras 1 in 1991, as an allergic angina syndrome. The first association of cardiac symptoms and an allergic event date back to 1950. 2 Diagnosis needs the concurrent presence of acute coronary syndrome and an allergic event. This syndrome might result in death by myocardial infarction (MI). It is caused by inflammatory mediators such as histamine, neutral proteases, arachidonic acid products, platelet activating factors, and a variety of cytokines and chemokines which are released during the activation process. The release of mediators during allergic insults has been incriminated as a cause of coronary artery spasm and/or atheromatous plaque erosion and rupture. We presented a patient with recurrent myocardial infarction with ST-segment elevation (STEMI) who had no sign of systemic allergic reactions except coronary spasm after parenteral diclofenac administration.
Case
A middle-age patient was presented with weakness and general muscular pain to emergency department. She had previous MI 2 years ago. She has also a history of hypertension, bronchial asthma, and intermittent smoking. There was no Prinzmetal’s angina pectoris history. She was taking aspirin, ramipril, and bronchodilators whenever necessary.
She was administered to emergency department, suffering from squeezing, chest pain in association with sweating and nausea without allergic reactions such as pruritus, erythema, urticaria, and bronchospasm after 5 h of intramuscularly taking diclofenac sodium injection for myalgia. Shortly after chest pain, her medical situation got worsened and her blood pressure was 60/40 mmHg and heart rate was 38 beats/min. Her skin was cold and sweaty. The examination of cardiac and other systems was unremarkable except findings mentioned above. Electrocardiogram (ECG) showed prominent ST-segment elevations in leads II, III-aVF, and V5–6, and ST-segment depression in leads aVL andV1–3 with atrioventricular (AV) complete block (Figure 1). Atropine (1 mg) and rapid saline infusion were intravenously given. AV block was subsequently resolved and blood pressure was increased to 110/70 mmHg, but ST elevation in inferior leads persisted. Acute infero-posterior STEMI was considered and following intravenous morphine sulfate (2 mg) and oral aspirin (300 mg) were given and the patient was taken to catheter laboratory for primary percutaneous coronary intervention. Coronary angiography revealed dominant left circumflex artery (LCx) with non-significant plaque and left anterior descending artery (LAD) with normal appearance. Right coronary artery (RCA) was non-dominant without a fixed stenosis (Figure 2). We considered that non-significant plaque in LCx and RCA were not responsible for the acute infero-posterior STEMI. At the same time, her chest pain was relieved and ST elevation was resolved in the ECG. Since she was considered to have a possible diclofenac-induced vasospastic STEMI, she was given diltiazem (oral 2 × 60 mg), clopidogrel (oral 300 mg and then 75 mg), and enoxaparin (2 × 1 mg/kg subcutaneously) in addition to aspirin. Initial cardiac troponin I was normal, but it was elevated (0.026 ng/mL; normal value <0.006 ng/mL) at 6 h. Other routine biochemical tests were normal except blood sugar (131 mg/dL) and low-density lipoprotein cholesterol (98 mg/dL). White blood cell was slightly high (13.3 cells × 109/L) and eosinophilia (6%) was present in peripheral smear. Echocardiography revealed an ejection fraction of 60% and mild hypokinesia in mid segment of inferior wall of the left ventricle.
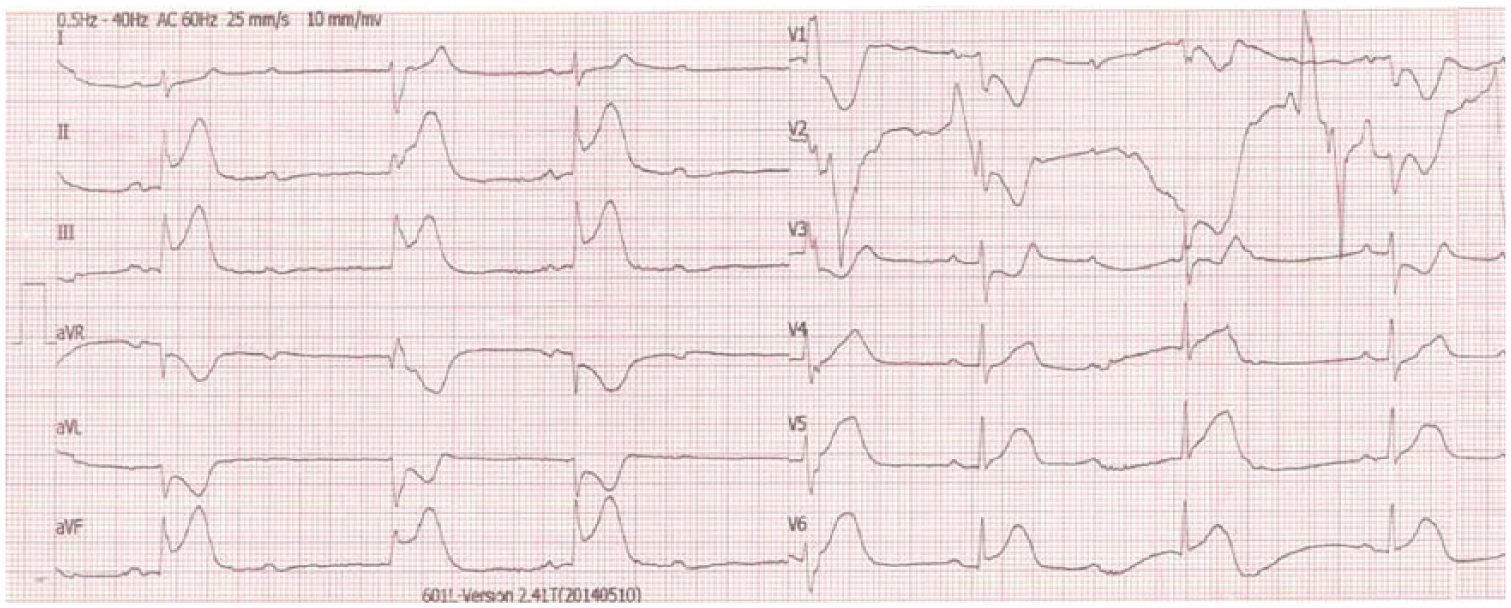
Inferior ST elevation and reciprocal ST depression with AV block.
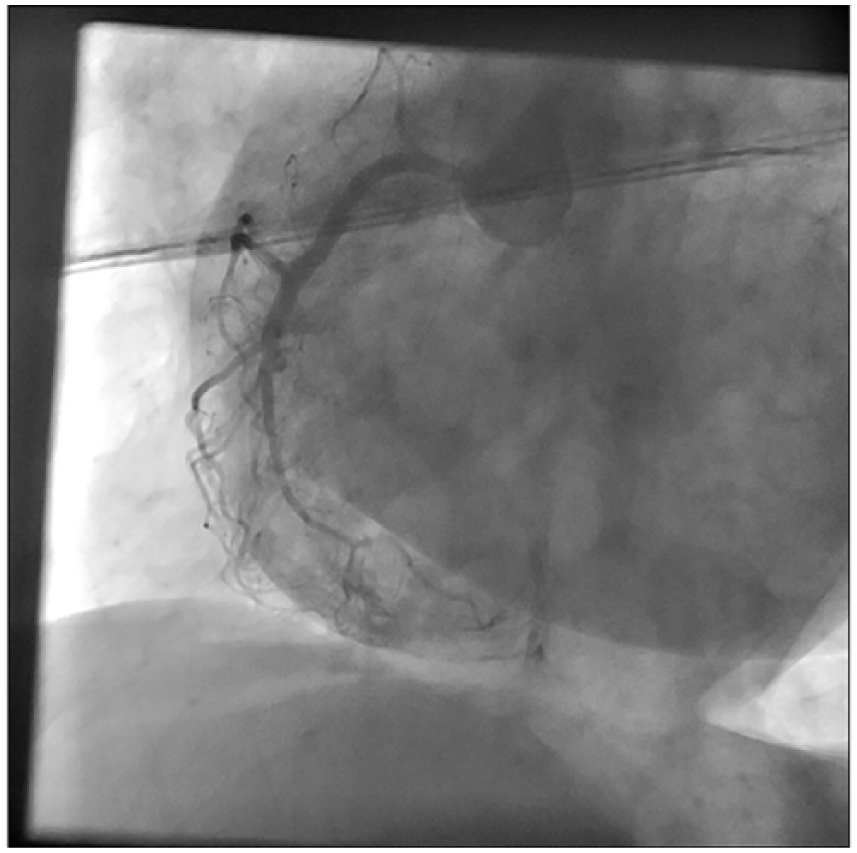
Coronary angiography for RCA at 2016.
When taking detailed medical history, we noticed that she had experienced acute anterior STEMI 25 months ago after having taken intramuscular diclofenac sodium for headache and ear pain in emergency department (Figure 3). She had immediately undergone coronary angiography, but no significant stenosis in the LAD and subsequently received medical therapy with oral long-acting nitrate and aspirin. In addition, any ruptured plaque responsible for anterior STEMI had been observed on intravascular ultrasound (IVUS) imaging.
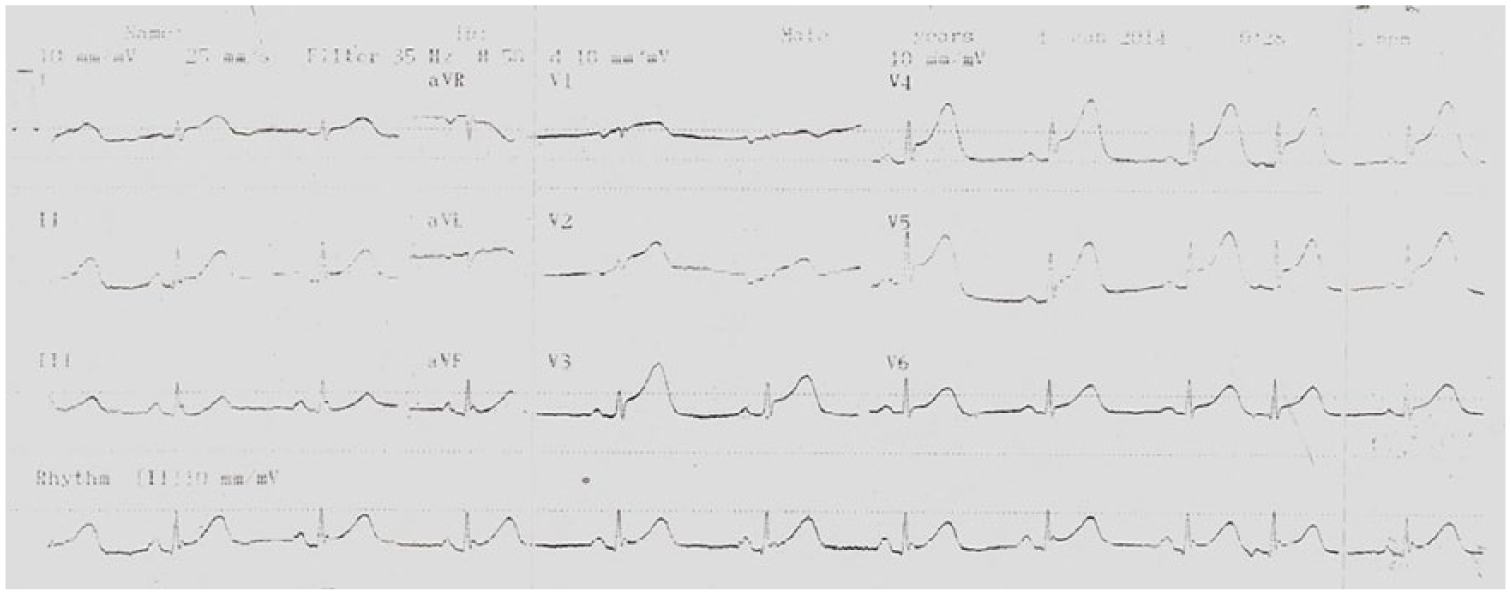
Anterior MI with ST elevation 25 months ago.
To investigate the etiology of STEMI, further hematological tests were performed. The activities of protein C, protein S, antithrombin III, and activated protein C were within normal limits. Serum homocysteine level was also normal. Anti-phospholipid antibodies and Factor V Leiden mutation were negative. Immunoglobulin E level was high.
Since she experienced chest pain relevant to STEMI after diclofenac administration at both presentations, she was considered as having an allergic STEMI without any systemic allergic reaction and discharged with diltiazem, ramipril, aspirin, clopidogrel, statin as well as inhaler bronchodilator therapy if required. She remained uneventful at first month follow-up.
Discussion
The clinical manifestations of the KS focus on typical cardiac signs and symptoms such as chest pain and electrocardiographic alterations in ST segment. 1 Antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs) are the most frequently involved drugs. 3
We presented a patient with recurrent, wandering STEMI who had no sign of systemic allergic reactions. Classical presentation of KS has a spectrum from various allergies to hypersensitivities, such as hypotension, pruritus or dyspnea. Out of the typical presentation of this syndrome, our case mainly had chest pain. Diagnosis of KS without systemic allergic sign may be difficult because of insignificant clinic. This may be an aggravated type of Prizmental angina. This situation is about the local coronary allergic reaction, as total spasm, to diclofenac administration. KS frequently reported from Spain, Italy, Greece, and Turkey. 4
In the largest series that we can access, Renda et al. 3 presented 51 KS cases. The incidence and etiology are unclear. They collected two diclofenac-induced KS.
Also in our data screening, because the spectrum of KS is wide and cardiac symptoms are more vital that they are at the forefront of the treatment, we cannot reach any definite data on noncardiac symptoms and frequents.
KS has three variants—Type I, Coronary vasospasm type: In patients with normal coronary arteries, there is no atherosclerosis. Acute release of inflammatory mediators can induce coronary artery vasospasm. This vasospasm may cause angina without increase of cardiac enzymes or may progress to acute MI with raised cardiac enzymes. Type II, Coronary atherosclerosis: This occurs in patients with culprit, but stable basal atheromatous disease, in whom the acute release of inflammatory mediators can induce coronary artery vasospasm. This vasospasm may cause angina without increase of cardiac enzymes if only vasospasm occurs without plaque rupture/erosion or may progress to acute MI with raised cardiac enzymes if plaque rupture/erosion occurs. 5 Type III, Drug-eluting stent thrombosis: Observed in patients with coronary thrombosis (including stent thrombosis), aspirated thrombus specimens had eosinophils and mast cells form thrombus. Furthermore, type III variant occurs in stented patients who died suddenly and histological examination of coronary artery showed that stent was infiltrated by eosinophils and/or mast cells. 6
In all three conditions, coronary event was triggered with allergic reactions and treatment is similar with acute coronary syndromes if there is a plaque rupture and thrombus formation in coronary. But if clinic is only vasospasm without plaque rupture, there will be no need for coronary intervention after dissection of vasospasm. Treatment of vasodilator (nitrate, calcium channel blocker) medications is the main treatment option.
Our patient’s clinical situation was between type 1 and 2. She has a coronary disease with elevated troponin levels, but no severe stenosis and plaque erosion or rupture. Since she experienced chest pain relevant to STEMI after diclofenac administration at both presentations, she was considered as having an allergic STEMI without any systemic allergic reaction. In first presentation of acute anterior MI, there wasn’t any symptom of systemic allergic reaction like erythema, urticaria, angioedema, and hypotension and she did not say anything about diclofenac injection. We performed IVUS after coronary angiography for LAD, but we couldn’t find something that explains clinic situations. In second presentation of acute inferior MI, there wasn’t any symptom of systemic allergic reactions again. She had AV complete block and hemodynamically unstable, life threatening situations. Coronary angiography was normal again. That’s the first case that we know who has reactive different coronary artery for diclofenac administration at the different time and she hasn’t any systemic alert for allergies.
Treatment of KS is still debated. Treatment of the allergic reactions, both H1 and H2 antihistamines, such as diphenhydramine and glucocorticoids, crystalloid, and normal saline, is important when a systemic allergic reaction happens. In our case, chest pain relevant to STEMI without any systemic allergic reaction was experienced, therefore we discharged her with diltiazem, ramipril, aspirin, clopidogrel, statin as well as inhaler bronchodilator therapy if required. She remained uneventful at first month follow-up.
Footnotes
Author contributions
E.Ö. made a contribution to the concept of the case and analyzed the collected data. Z.K. drafted the article and revised critically. M.K. and U.P. collected necessary data for the work. F.T. approved the version before publishing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data collected for the work can be obtained from the database of İzmir Atatürk Training and Research Hospital. The figures we published do not have patient’s name.
Ethical approval
Ethical approval is not required as it is a case report.
Human rights
There is no violation of human rights.
Informed consent
All procedures were performed with approval of patient under clinical ethic.