
Abstract

Dear Editor,
It is very inspiring to learn from the Ruttonjee Hospital emergency department (ED) on reporting the first successful return of spontaneous circulation (ROSC) and Survival-to-Admission (STA) case (though without achieving Survival-to-Discharge (STD)) of a middle-aged obese smoker with refractory ventricular fibrillation (VF) by SKJ Lau et al. in the January issue of 2019 of your esteemed Journal. 1
To improve the success of defibrillation, the following technical skill factors are important:
The earlier the defibrillation, the higher is the survival since there is a 7%–10% decrease for each minute of delay in the first 10 min of cardiac arrest with shockable rhythms and consequently public access defibrillator is important.
The defibrillation paddle or electrode size should be large enough to minimize the electrical impedance while not too big to cause over-proximity leading to arcing (electricity passes through the air directly between electrodes resulting in explosive noises, burns, and reduced current delivery through the heart). The usual recommendation is from 8 to 10–13 cm2. 2
Adequate compression pressure of at least 6 kg f 3 on each hand-held defibrillation paddle with gel-pad contact with the skin if self-adhesive MFE (multi-function electrode) pads are not used.
Defibrillation during the expiration phase if the patient connected to a ventilator can help decrease the transthoracic impedance.
The electrode positions are as follows: (a) Antero-apical: one pad/paddle is applied to the right of the sternum just below the clavicle, and the other is centered lateral to the usual cardiac apex in the anterior or mid-axillary line (V5–6); (b) Antero-posterior: the anterior pad/paddle is positioned over the precordium or apex, and the posterior pad/paddle is placed on the back in the left or right infra-scapular region (should avoid the spine to reduce electrical resistance) though studies have shown four positions (antero-apical, antero-posterior, anterior–left infra-scapular, and anterior–right infra-scapular) are of equal efficacy in in defibrillation (for VF/pulseless ventricular tachycardia (VT)) or elective atrial fibrillation (AF) cardioversion success.
4
This is to address the individual variation and try to maximize the greatest current passing through the heart through the least electrical impedance.
In this case report, the prehospital defibrillation was by Philips HeartStart FR3 AED with self-adhesive electrodes for four times.
In the ED, another four times of biphasic defibrillation ranging from 150 to 200 J was provided by the Nihon Kohden TEC-5531K, but the use of paddles or self-adhesive MFE was not specified.
In view of the failure of the prehospital defibrillation, one may consider to start the ED defibrillation of another biphasic waveform at the maximum available energy with a hope for quicker efficacy instead of escalation since the non-conversion would delay the ROSC with higher neurological sequelae and end-organ hypoperfusion.
Adjuvant pharmacotherapy including vasopressor and anti-arrhythmics was administered. However, ABG assay, NaHCO3 use (despite significant knowledge gap still exists) after prolonged cardiac arrest, endotracheal intubation (ETI) to attain adequate ventilation to prevent paradoxical intracellular acidosis and any dys-kalemia were not mentioned.
Owing to the refractory VF, dual simultaneous external defibrillation (DSED) was attempted with 200 J set on each of the two Nihon Kohden TEC-5531K biphasic defibrillators.
The post-ED arrival time interval till the DSED decision was only 13 min; it would be appreciated not all the pertinent factors were evaluated during the very short period when managing the dire and highly stressful situation.
Although ROSC was attained with rhythm conversion to accelerated junctional rhythm, it is noteworthy that the electrode placement of the DSED as shown in the report (Diagram 1) would need refinement to help enhance success of future application of this novel electrical therapy:
In the antero-lateral placement, the lateral electrodes should be closer to the cardiac apex instead of being placed at the left lower costal margin.
In the antero-posterior position, the back electrode should not be placed over the spine of high electrical resistance but at the infra-scapular position.
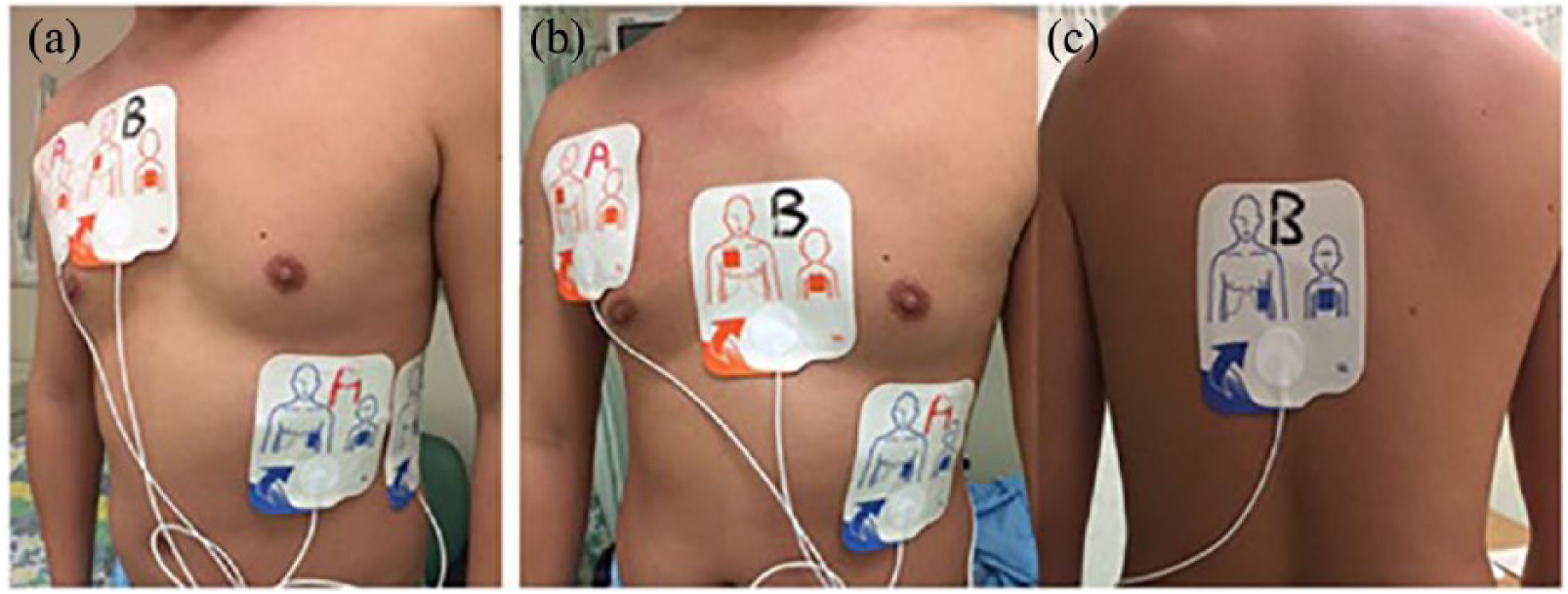
Positions of MFE for DSED indicated in case report. (1) It was difficult to place two pairs of MFE on the anterior chest wall even in an adult owing to the limited surface area, not to mention in females with bulky breasts, (2) for the antero-lateral position (A), the lateral MFE was placed at the lower rib margin, which was lower than the recommended position of centering at the fifth or sixth intercostal space, and (3) for the antero-posterior pair of electrodes (B)—the anterior over lower sternum (body structure of high electrical resistance) and posterior over the spine (bony structure of high electrical resistance) as indicated in the case report were not the best positions.
Although the Nihon Kohden website may not provide good guideline on the back electrode position, 5 the Australasian Guidelines,6,7 an EM Website, 8 and manuals of other brands9,10 offer more precise placement description as indicated in Diagram 2.
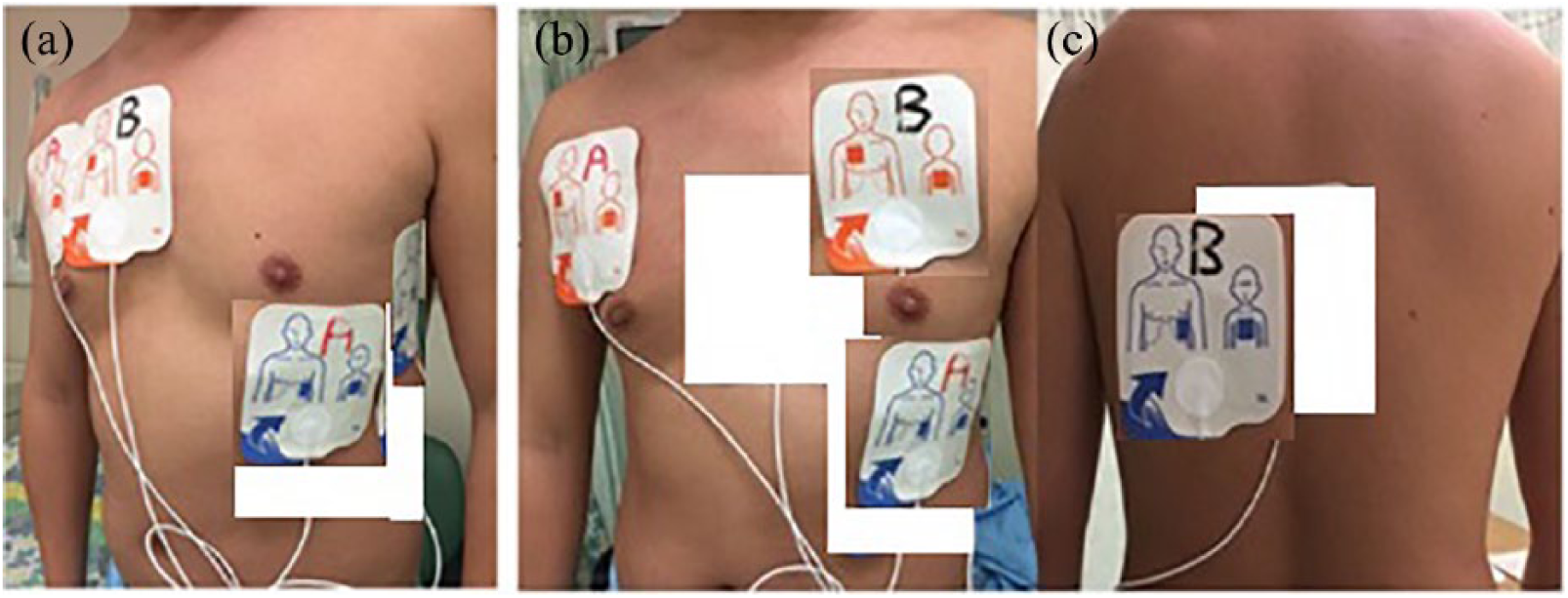
The preferred alternative positions of MFE for DSED: (1) for the antero-lateral position (A), the lateral MFE should be centered at the fifth or sixth intercostal space or as close as possible while avoiding the nipple and (2) the preferred antero-posterior (anterior: cardiac apex or precordium; back: left infra-scapular) electrode position to reduce the transthoracic impedance by avoiding the large bony structures.8–10
Past experience of incorrect placement of the back electrode (over the scapula or spine) has caused failure in external cardiopacing.
In the monophasic defibrillator era about 10 years ago in Hong Kong, a stack of three defibrillation from 200, 300, and 360 J was applied as the initial electrical therapy for VF/pulseless VT with the rationale that the preceding shock could enhance the efficacy of the subsequent one by lowering the transthoracic impedance. However, the charging time for each shock could take 10–30 s (depending on the brand and model durability) and hence would result in a prolonged period of 30–90 s of no External Cardiac Massage (ECM). With the commencement of biphasic defibrillator in the past 10 years, the stack of three was replaced by one shock since stacking did not add significant success benefit as elucidated in the AHA ALS (American Heart Association Advanced Cardiovascular Life Support) Guidelines in 20102 and 2015. 11
Most biphasic defibrillators can only produce energy up to 200 J, while some models can generate up to 360 J, 10 addressing the non-conversion cases by 200 J.12–14 However, most ED would only keep one to two brands of biphasic defibrillators and hence access to higher energy might not be available. The important DSED principle lies on facilitation and greater energy.
Human studies on biphasic truncated exponential (BTE) Waveform defibrillation have not identified cardiac injury as demonstrated by biomarker, ECG, or ejection fraction with energy level reaching 360 J. 15 However, we would require future Prospective Randomized Control Trial (PRCT) to evaluate the advantages and complications of the DSED of up to 400 J of energy or higher.
Saving the life together with good neurological outcome of a patient does not merely bring positive impact to the family, but the community as a whole to diminish healthcare burden.
I would be most delighted to learn the subsequent discussion of the learned authors and wish them very fruitful clinical researches to maximize the prognosis of the critically ill patients!
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.