
Abstract
Background:
Rose Angina Questionnaire (RAQ) is a useful screening questionnaire for ischemic heart disease validated in different settings; however, its diagnostic ability to predict myocardial infarction (MI) in the emergency is less clear.
Objectives:
To find out the usefulness of RAQ to predict MI in patients presenting to the emergency.
Methods:
A cross-sectional study was conducted at the BP Koirala Institute of Health Sciences (BPKIHS), a teaching hospital in eastern Nepal from 1 January to 30 March 2017, after ethical clearance from the Institutional Review Committee. Informed consent was obtained from the patients for their anonymised information to be published in this study The samples were collected from 100 patients with chest pain aged 40 to 70 years presenting to the emergency. RAQ was applied and its performance to detect MI was compared with emergency and cardiologist diagnosis of MI. Sensitivity, specificity, positive predictive value and negative value were calculated along with descriptive analysis.
Results:
A total of 100 patients were analysed with the mean age of 63.78 years (SD 11.60) and male to female ratio of 1.94. RAQ detected 58 cases (63.8%) with emergency department (ED) diagnosis of MI (true positive) and identified 3 (33.3%) cases with non-MI (true negative). The true positive rate for RAQ to detect MI after cardiologist consultation was 71.6%. RAQ had a sensitivity of 84.91% (95% confidence interval (CI) 72.41% –93.25%) to detect positive troponin, 63.74% (52.99–73.56) to detect positive electrocardiogram (ECG) and 71.60% (95% CI 60.5% to 81.07%) to detect final diagnosis of MI.
Conclusion:
RAQ is a good screening tool to detect MI in the emergency that can be used in isolation or in combination with other diagnostic modalities to detect it early.
Introduction
Cardiovascular diseases (CVDs) are the number one cause of death globally with an estimated 17.7 million deaths; 7.4 million of these are due to coronary heart disease (CHD) (see study by the World Health Organization (WHO)). 1 This burden of CVDs has become increasingly important in low- and middle-income countries as few data exist on the prevalence of a spectrum of ischemic heart disease in developing countries. 2 Myocardial Infarction (MI), one of the five main manifestations of the CHD, other than stable angina pectoris, unstable angina pectoris, heart failure and sudden death, is a common presentation in the emergency. 3
The baseline data on the spectrum of ischemic heart disease in Nepal are few and far between although the CVD has been listed as the top four killers of non-communicable disease. Maskey et al. reported that the first definite diagnosis of MI in Nepal was made in 1945. Since then, the numbers have climbed steadily with a 40-fold increase in diagnosis by 2003. 4
The WHO Rose Angina Questionnaire (RAQ) was designed in 1962 to assess the probability of underlying coronary artery disease in epidemiologic studies of population groups. Since then, the screening tool has been validated for use in many countries to detect CHD in epidemiological research as well as in ED to detect MI.5,6 However, the sensitivity and specificity of the tool may vary depending on the country and the reference gold standard chosen. 7 . A number of population-based studies in India and Bangladesh used RAQ to detect CHD,8,9 but the use of the tool to screen for MI in ED setting was not found from Nepal. This research was planned with the aim to find out the usefulness of RAQ for diagnostic prediction of MI in a relatively resource-limited setting in an emergency in the eastern part of Nepal.
Methods
This was a hospital-based cross-sectional study conducted in the emergency ward of the BP Koirala Institute of Health Sciences (BPKIHS), a medical university in the eastern part of Nepal from 1 January to 30 March 2017. The study population included patients aged 40 to 70 years with chest pain. Informed consent was obtained from the patients for their anonymised information to be published in this study. Ethical approval was taken from the Institutional Review Committee, BPKIHS. Coding was done to hide the patients’ identity.
The total sample size was calculated considering the sensitivity and specificity of RAQ to detect suspected MI (Sensitivity 51%, 95% CI 45–57; Specificity 96%, 95% CI, 92–98) and all ischemic heart disease (Sensitivity 53%, 95% CI 48–59, Specificity 89%, 95% CI 82–93) as per the study done by Rahman et al. 5 in Bangladesh. With comparable values the total number was rounded off to 100 to allow for non-response and missing data. The alpha error at 5% and permissible error equalling 20% of prevalence was used to estimate the sample size.
Study tools
RAQ
It is a validated tool used in different settings for the diagnosis of ischemic heart disease including MI. The questions only included the part for the diagnosis of incident MI and positive RAQ was defined as an affirmative response to both question 1 and question 2.
RAQ possible MI questionnaire
Within the last one year, have you ever had a severe pain across the front of your chest lasting for half an hour or more? Yes/No If No, go to the ‘angina of effort questionnaire’ If Yes, ask the following question:
Did the pain occur for the first time in the last year? Yes/No If Yes to Q1 and Q2, diagnose as ‘incident case of possible MI’
Diagnosis of myocardial infarction
All the patients were triaged with a high priority score for chest pain suggestive of cardiac aetiology. The patients underwent ECG at presentation and a requisition for cardiac marker troponin was sent. An initial diagnosis of MI was formulated by emergency doctors based on their expertise with no interference from researchers. The current protocol in the emergency is to give Australasian Triage score two for chest pain. An ECG is obtained within five to ten minutes in emergency. A brief initial assessment history is then taken. The protocol recommends using the definition of MI as given by WHO. WHO recommended that the descriptors of chest pain suggestive of MI are various combinations of chest, upper extremity, jaw or epigastric discomfort with exertion or at rest; the discomfort usually lasts more than 20 min, often is diffuse, not localised, not positional, not affected by movement of the region and it may be accompanied by dyspnoea, diaphoresis, nausea or syncope. 10
ECG criteria used
The criteria used for positive ECG are as per the WHO guidelines 10 and included
ECG changes indicative of new ischaemia (new ST-T changes or new left bundle branch block (LBBB)–Minnesota codes: ST-depression 4.1; 4.2; ST-elevation 9.2; LBBB 7.1);
Development of pathological Q waves in the ECG (Minnesota codes: 1.1.1 through 1.2.5 plus 1.2.7), 17 including no unequivocal pathological Q waves in the first ECG or in event set of ECG(s) followed by a record with a pathological Q wave or any Q wave in leads V2–V3 ⩾ 0.02 s or QS complex in leads V2 and V3 or Q wave ⩾0.03 s and ⩾0.01 mV deep or QS complex in leads I, II, aVL, aVF or V4–V6 in any two leads of a contiguous lead grouping (I, aVL, V6: V4–V6: II, III, aVF).
Cardiac marker troponin
Troponin was measured using a qualitative test kit ‘cTnl one step troponin I test’. The cut-off level used in this test kit is 0.5 ng/mL. Troponin test was repeated after 6 hours in early presentations and initial negative test.
The standards of diagnosis for MI were ED diagnosis based on history and ECG findings, troponin positivity and the final diagnosis of MI, which was made after consultation with the cardiologist on duty.
The patients were subsequently divided into RAQ positive and negative groups and compared for diagnostic sensitivity, specificity, positive predictive value, negative predictive value and accuracy to predict positive ECG, positive troponin and final diagnosis of MI in the emergency. The statistical software used Microsoft Excel and SPSS for data management and analysis. Descriptive analysis was performed for socio-demographic profile and risk factors for CHD.
Results
A total of 100 patients were included in the study with the mean age of 63.78 years (SD 11.60). The male to female ratio was 1.94 and the majority were literate (64%). History of hypertension was present in 59% and 57% were smokers (Table 1).
Population characteristics (n = 100).
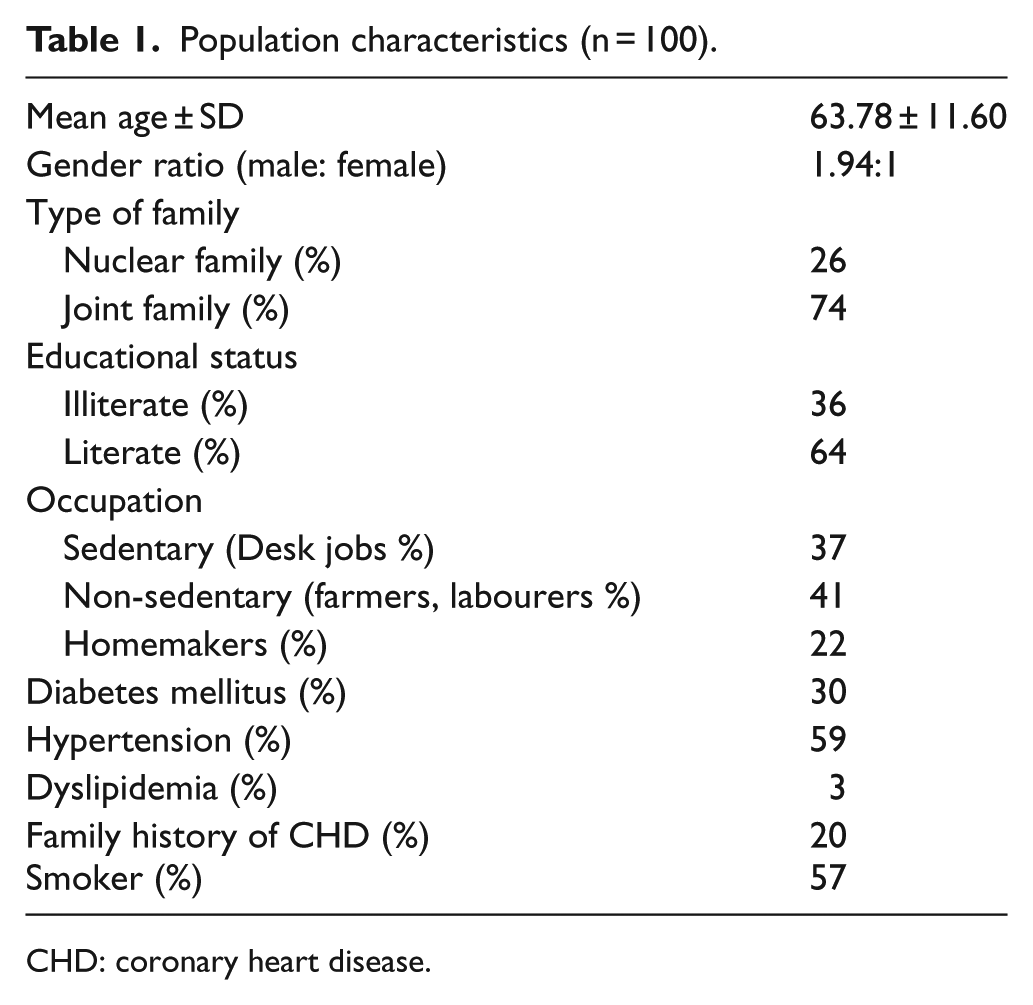
CHD: coronary heart disease.
ECG was suggestive of MI in 91 cases. The initial diagnosis of MI with ST elevation was made in 45 cases, non-ST-elevation MI was made in 46 cases and 9 cases were labelled as non-cardiac chest pain. Troponin was positive in 53 cases. The final diagnosis of MI in emergency after cardiologist consultation was made in 81 patients. RAQ was positive in 64 patients.
RAQ detected 58 cases (63.8%) with positive ECG (ED diagnosis of MI, true positives). It was able to correctly identify 3 (33.3%) cases labelled as non-MI chest pain in ED (ED diagnosis of non-MI true negative). The true positive rate for RAQ as the screening test to detect the final diagnosis of MI after cardiologist consultation was 71.6%, (true positive). Among 19 cases with non-MI final diagnosis, RAQ detected 13 cases (true negative). The true positive rate for RAQ as the screening test to detect MI based on troponin positivity alone was 84.9%, among 47 patients with negative troponin, RAQ detected 28 cases (true negatives) (Table 2)
Clinical and Rose Angina Questionnaire diagnosis of myocardial infarction (n = 100).
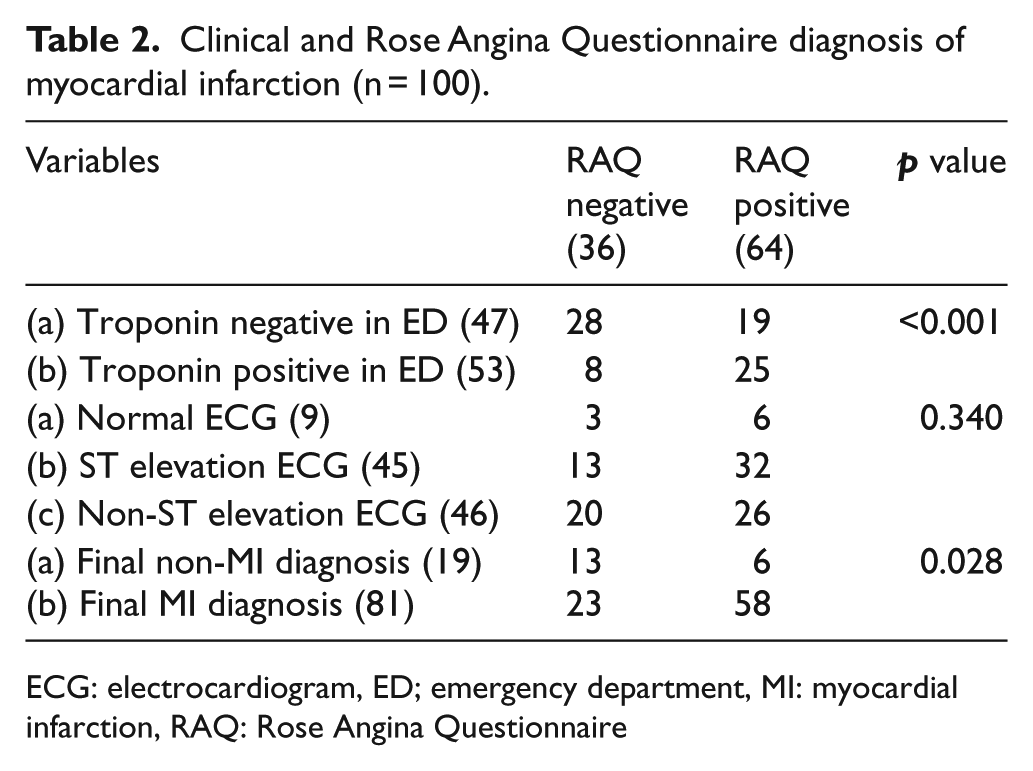
ECG: electrocardiogram, ED; emergency department, MI: myocardial infarction, RAQ: Rose Angina Questionnaire
Angiography was done in 30 cases. RAQ was positive in 28 cases. In this group undergoing angiography true positive rate for RAQ as a screening tool was 95.8%, the false negative was 4.2%, true negatives were 16.7% and false positive was 83.3% (n = 30, p<0.001, chi-square).
The sensitivity of RAQ to detect chest pain in patients with positive troponin was 84.91% (72.41% to 93.25%), specificity was 59.57% (44.27% to 73.63%) with a positive predictive value of 70.31 (62.18 to 77.34). The sensitivity of RAQ to detect chest pain in patients with positive ECG was 63.74% (52.99% to 73.56%), specificity (CI) 33.33% (7.49% to 70.07%) with a positive predictive value of 90.63 (85.59 to 90.04). The sensitivity of RAQ to detect the final diagnosis of MI was 71.60% (95% CI 60.50% to 81.07%) and specificity was 68.42% (95% CI 43.45% to 87.42%) with a positive predictive value of 90.63 (83.10 to 95) (Table 3). The receiver operating characteristic curve (ROC) curve for RAQ showed area under the curve (AUC) of 0.865. (Figure 1)
Performance of Rose Angina Questionnaire to detect troponin positivity, emergency and final diagnosis of myocardial infarction.
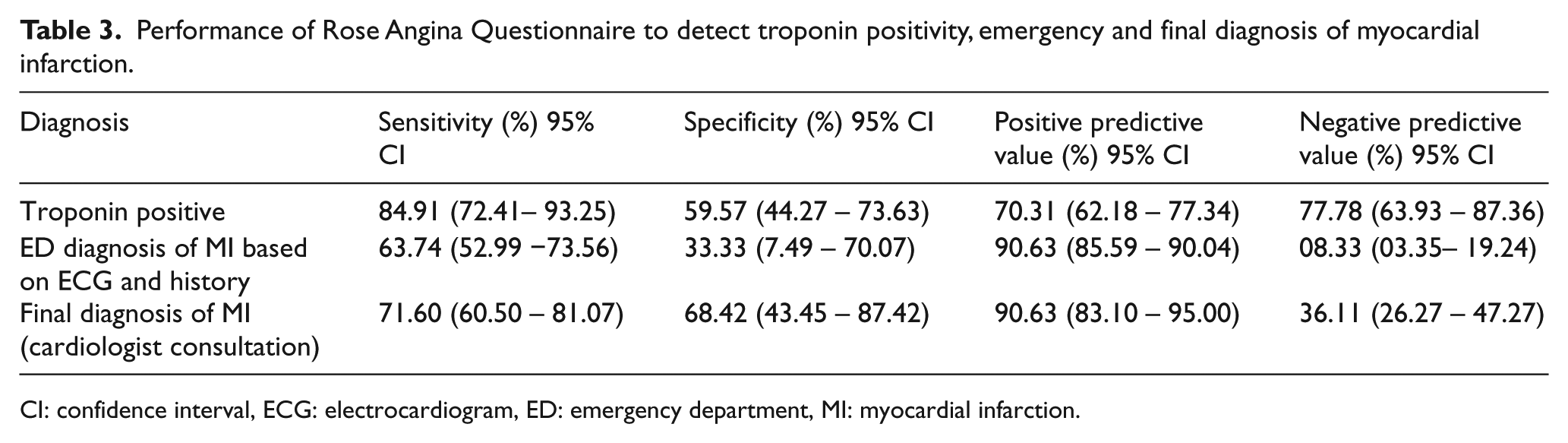
CI: confidence interval, ECG: electrocardiogram, ED: emergency department, MI: myocardial infarction.
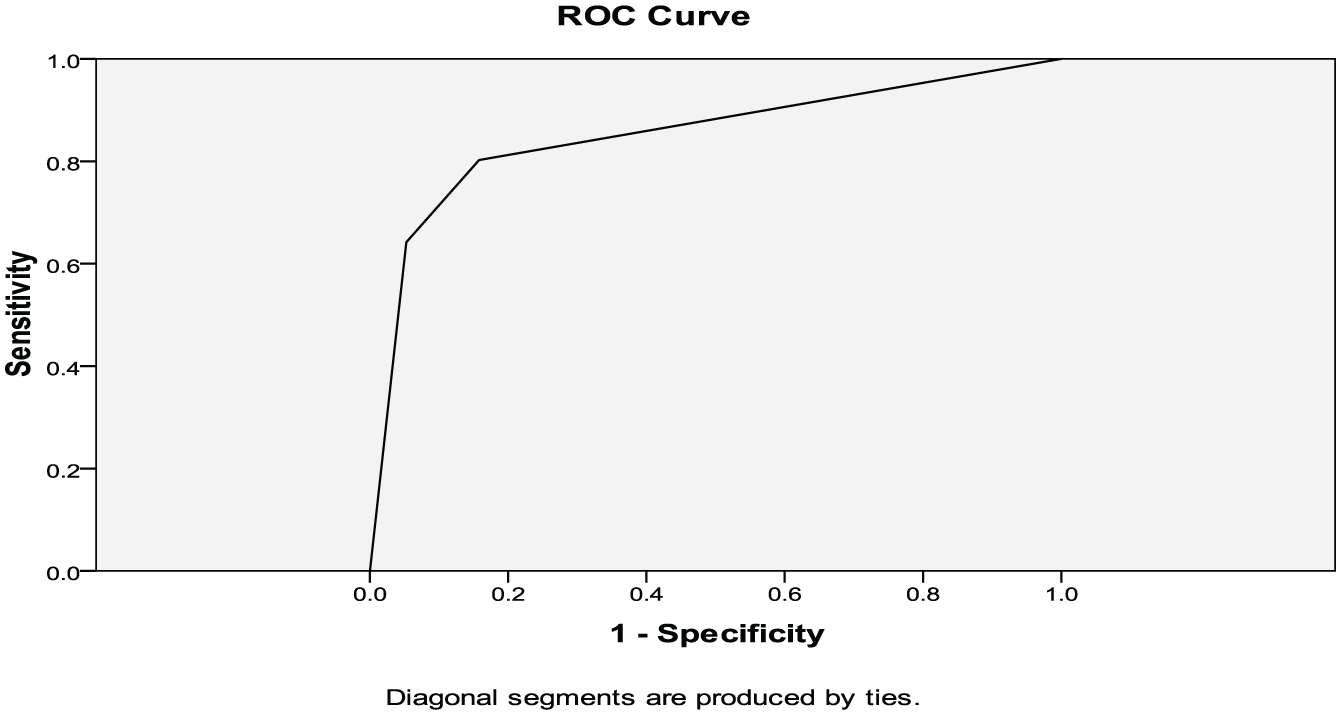
Diagonal segments are produced by ties.
Discussion
RAQ had been used as a tool in a community-based study in the same city where the study was carried out to detect the burden of probable CHD in 2009. In this study, Vaidya et al. 11 reported the prevalence of CHD at 5.7% using RAQ and ECG. Distribution of risk factors from Vaidya’s study compared to this study was a family history of CHD 16.1% (current study 20%), tobacco consumption 7.3% (57%) and hypertension 35% (59%). Among other risk factors, diabetes was present 30% in our study. An apparent increase in the risk factors may reflect the high-risk population that presents to the emergency. The identification, timely triage, rapid assessment and the reperfusion decision has been the standard of care for suspected MI in the emergency. Early ECG and use of cardiac markers have been the diagnostic modalities, as well as a supplement for the identification and early initiation of care leading to maximal benefit; however, both have their limitations as diagnostic tools.12–14 The RAQ was designed to identify subjects with the likelihood of having coronary artery disease when used as an epidemiologic tool. 5 But its role in the diagnosis of MI in hospital and emergency setting is less clear. Haywood and others 6 reported that RAQ positive patients had a lower chance of a discharge diagnosis of MI compared to RAQ negative patients (OR 0.73) in a large hospital-based study. A past history of MI increased this odds ratio in the younger population (OR 2.11). Rahman et al. 5 in Bangladesh showed that RAQ had a moderate sensitivity but a higher specificity to diagnose CHD (53% sensitivity, 89% specificity) and MI (51% sensitivity, 96% specificity). We tested the diagnostic accuracy against three standards: final diagnosis (after cardiology consultation), ED diagnosis (history and ECG) and troponin positivity in ED. Our study had a sensitivity of 72% and a specificity of 68% to detect a final diagnosis of MI made after cardiologist consultation. The sensitivity to detect the initial diagnosis at emergency that was largely based on ECG findings and clinical history was however moderate (64%) with still lower specificity (33%) compared to Gupta and Sakthiswary 14 who found moderate sensitivity (55%) but a higher specificity (71%). The ECG criteria taken for this study was ST elevation, ST depression and T inversion only, which might explain the higher specificity detected along with population variation. 14 The sensitivity for troponin was 85% and specificity was 60% compared with Gupta and Sakthiswary 14 with 44% sensitivity, 96% specificity and Baheti et al. 15 with 65% sensitivity and 71% specificity. Both of these studies were based in the Asian region but varied in ethnic and methodological issues. Local availability of resources seems to govern the diagnostic choices in most of the studies conducted in the region. The average population in our study was 63 years and missed relatively younger population compared to Rahman et al. 5 (53 years) and Haywood 6 (53 years and 61 years in two cohorts). This suggests that although RAQ, when used alone, may miss some cases it can be a useful tool to augment the diagnostic accuracy along with the initial ECG. This can also supplement the nurse-led triage because of brevity and easiness to administer.
Limitations
This is a single centre study with a limited sample size of 100 patients. The study was done in a major centre for referrals from the eastern part of Nepal and the results should be analysed considering the high-risk chest pain referrals. Angiography could only be performed in 30 patients due to the limited availability and other socioeconomic factors at that time.
Conclusion
Our study shows that RAQ is an effective, feasible and cost-effective tool with moderate sensitivity and high specificity for detecting MI that can aid in early diagnosis of MI. It has a role in isolation, as well as an addition to conventional methods like ECG, clinical history and cardiac markers for fast track care to early intervention and management of MI.
Footnotes
Acknowledgements
M.P. and R.B. helped in the concept analysis, design, data collection, interpretation of data, literature review, preparation of initial and final draft.
G.M., S.U. and R.C. helped in literature review, draft preparation and analysis
D.D.B. helped in literature review and interpretation of data
S.K.S. helped in concept, analytics and final draft
All the authors read and approved the final draft
Declaration of conflicting interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Institutional Review Committee of BPKIHS, Nepal.
Approval number obtained is: ref no 111/073/074 - IRC.
Human Rights
No human rights were violated during this study and the study was in accordance with Declaration of Helsinki.
Informed consent
All participants gave their written, informed consent prior to their inclusion in the study.