
Abstract
Background:
Ventricular assist devices, improve morbidity and survival in patients with end-stage heart failure.
Objectives:
To evaluate the major causes of emergency department admissions in patients with ventricular assist device support.
Methods:
The charts of 200,000 adult patients who presented to our emergency department between January 2016 and January 2018 were reviewed retrospectively. A total of 444 emergency department visits made by 99 patients with ventricular assist device were included in the study.
Results:
The annual incidence of emergency department admissions of patients with ventricular assist device was 0.1%. The mean age was 55.5 ± 11.1 years and 85.9% of the study population were men. The most commonly encountered diagnoses were abnormal international normalized ratio or international normalized ratio follow-up (18.2%); heart failure, non-specific chest pain, and chronic obstructive pulmonary disease (15.3%); minor/major bleeding (12.1%); neurological disorders such as ischemic stroke, transient ischemic attack, vertigo, migraine, and syncope (11.2%); non-device related infections (10.8%); ventricular tachycardia/fibrillation episode (8.5%); musculoskeletal disorders (7.2%); and device-related complications such as driveline infection and pump thrombosis (6.3%). Of the patients with bleeding, 31.1% had intracranial bleeding, 31.1% had epistaxis, 24% had gastrointestinal bleeding, 11.1% had hematuria, and 1.8% had gingival hemorrhage. Of the 15 patients who died, 73.3% were diagnosed with intracranial hemorrhage.
Conclusion:
Even though the mortality rates of patients with ventricular assist device tends to decrease, these patients still have significant morbidity due to the increase in the prevalence of ventricular assist device use. Except for device-related problems, emergency department management of this patient group does not differ much from other patient groups. As early diagnosis of any device-related problems is mandatory for decreasing mortality, emergency department physicians should be familiar with mechanical support systems.
Introduction
Ventricular assist devices (VAD) may be used for left ventricular, right ventricular, or biventricular support. Left VAD is reported to be the most commonly used VAD in clinical practice, and its use is becoming increasingly widespread in suitable advanced heart failure patients as a bridge to transplantation or as a bridge to life. 1 These devices comprised a pump implanted into a ring attached to the ventricular apex, a graft carrying blood from the pump to the ascending or descending aorta, a system controller connected to the pump by a percutaneous driveline, and a power source (Figure 1). The most common use of VADs is to provide support until a suitable donor is found. However, VAD use may also induce myocardial recovery and eliminate the need for further mechanical support, leading to device explantation. In patients who are deemed unsuitable for heart transplantation due to various reasons, VAD may be preferred as a long-term or permanent therapy (bridging therapy). 1
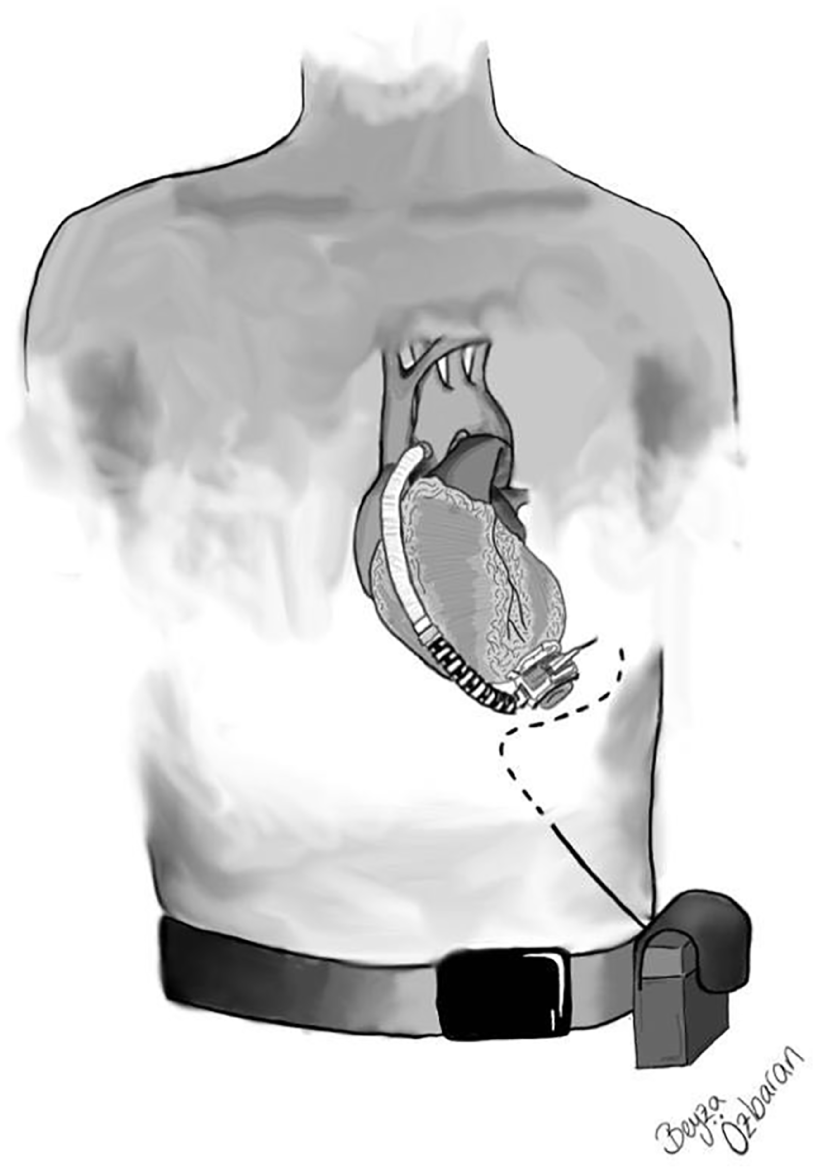
Ventricular assist device (VAD).
In our country, there are numerous centers and physicians experienced in the management of end-stage heart failure. In particular, our Cardiology and Cardiovascular Surgery clinic is one of the leading centers in Europe, averaging 25 heart transplantations and 100 assist device implantations annually. With increasing experience, the number of VAD-implanted patients also rises, which in turn results in an increase in the incidence of emergency department (ED) visits when these patients require immediate medical attention. 2
Literature on the out-of-hospital or ED management of patients with VAD is scarce. To our knowledge, there are very few studies in the literature which investigate the ED admissions and demographic characteristics of patients with VAD.
The aim of this study was to assess this patient population in terms of ED admission, management, diagnosis, and length of stay, and to determine whether there are shortcomings in the management of these patients.
Materials and methods
Study design and setting
This study was conducted in the Ege University Faculty of Medicine, which receives approximately 200,000 visits annually. After local ethics committee approval was obtained, a 2-year retrospective analysis was carried out in order to review the medical records of patients with VAD who presented to the ED between 1 January 2016 and 1 January 2018.
The data on age, gender, duration of VAD support, cause of VAD implantation, device type, concomitant diseases, vital signs on admission, presenting complaints, diagnosis, consultations requested, length of stay in the ED and in the hospital, the department the patient was admitted to, and mortality were obtained from the medical records.
Participants
Patients with VAD who were older than 18 years were included in the study. Patients with heart transplantation and patients with VAD who were younger than 18 years were not included in the study. During the 2-year study period, a total of 100 patients with VAD had visited the ED 445 times. One patient who was older than 18 years was excluded from the study.
Statistical analysis
All statistical analyses were performed using the SPSS statistical software (SPSS for Windows, version 22.0; SPSS, Inc., Chicago, IL, USA). Data were expressed as means with standard deviation, medians, and percentages. The chi-square test was used to compare categorical variables.
Results
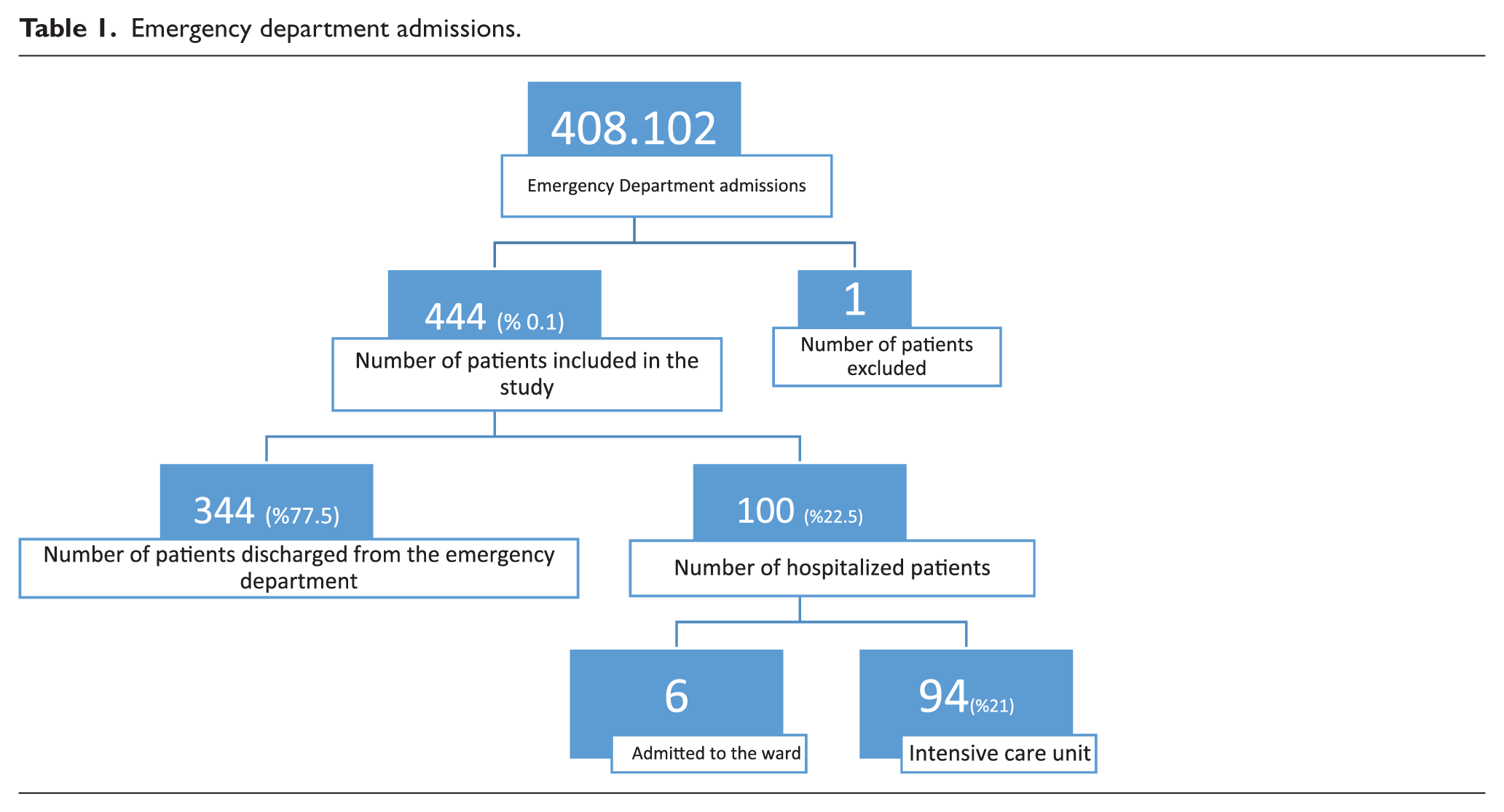
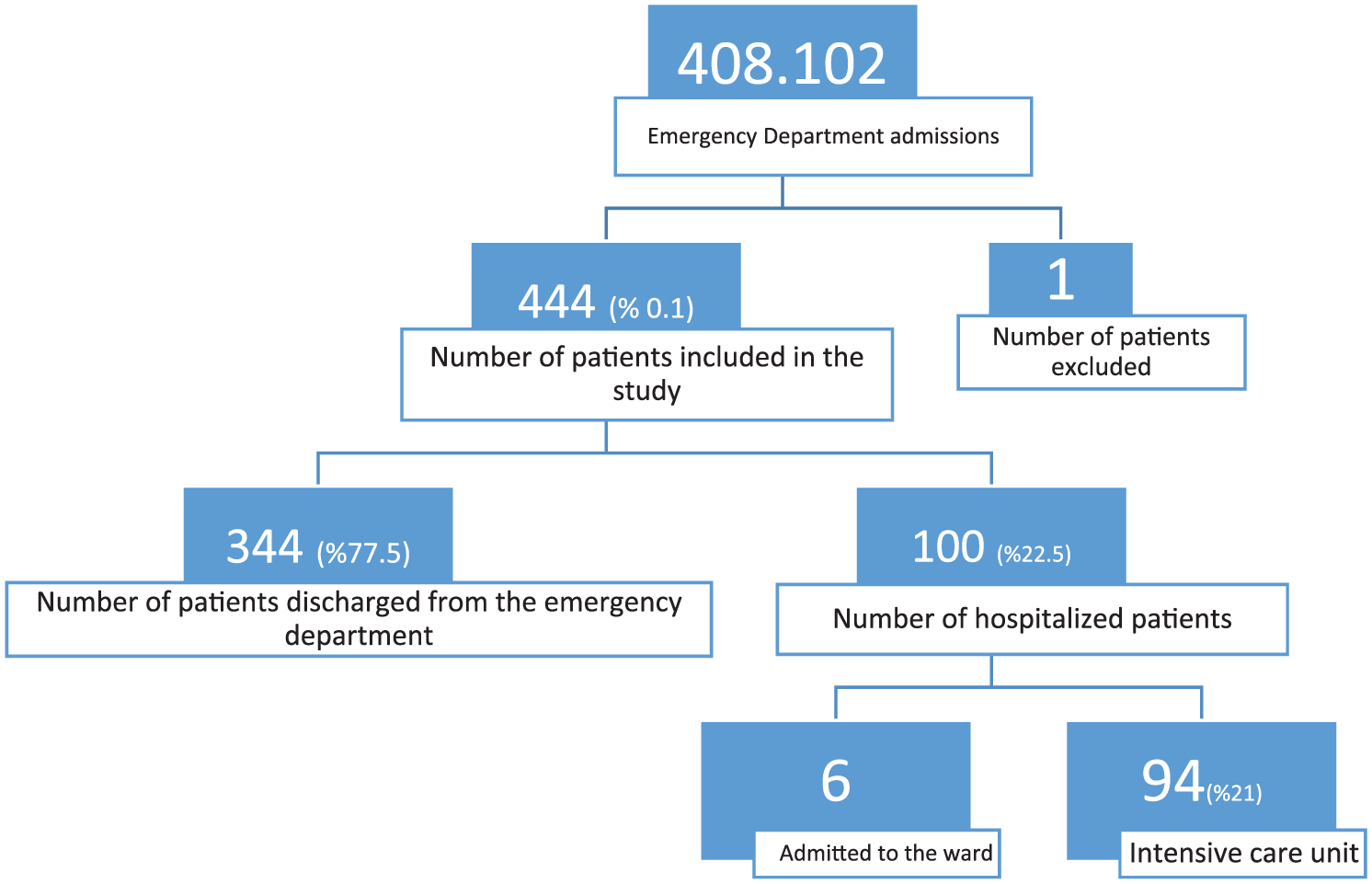
Within the study period, 408,102 patients presented to the ED. Of these, 202,585 presented in the year 2016 and 205,517 presented in 2017. A total of 444 ED visits made by 99 patients who met the inclusion criteria and who presented to the ED within the study period were included in the study (Table 1). The incidence of ED presentations of patients with VAD was 0.1%. The mean age was 55.5 ± 11.1 years, 85.9% of the patients were men, and 14.1% were women.
Emergency department admissions.
The VAD had been implanted due to ischemic dilated cardiomyopathy (ICMP) in 55.6% of patients and due to non-ischemic dilated cardiomyopathy (DCMP) in 44.4% of the patients. The fact that the device was implanted due to ischemic causes in 60% of men and due to non-ischemic causes in 71.4% of women was found to be statistically significant.
Of the patients included, 74.7% had Heartware (Heartware, Medtronic), 12.1% had Heartmate II (St. Jude Medical), 7.1% had Heartmate III (St. Jude Medical), 4% had Heart assist 5 (Reliant Heart), and 2 patients had biventricular Heartware VAD. The mean duration of VAD support was 18.4 ± 16 months (min: 1 month, max: 61 months).
As concomitant diseases, 53.5% of the patients had hypertension (HT), 51.5% had coronary artery disease (CAD), 32.3% had diabetes mellitus (DM), 22.2% had hyperlipidemia, 20.2% had cerebrovascular disease (CVD), 10% had chronic obstructive pulmonary disease (COPD), 4% had atrial fibrillation, and 2% had chronic renal failure (CRF). Prior to VAD implantation, 53.5% of the patients had undergone implantable cardioverter defibrillator, cardiac resynchronization therapy, or pacemaker implantation. Five patients had undergone coronary artery bypass graft, four patients had undergone mitral valve replacement, and one patient had undergone aortic valve replacement.
For most patients, it was impossible to measure the blood pressure during triage due to the absence of a palpable pulse and only 2.9% of the patients had their mean arterial pressures measured using Doppler ultrasonography. The mean heart rate was 86.7 ± 25.5 (min: 30/min; max: 240/min) and mean respiratory rate was 19.4 ± 2.3/min. Of the patients, 5.6% had a body temperature ⩾ 38°C, 2.5% had oxygen saturation (SaO2) < 90%, and 11% had an SaO2 between 90% and 94%. The presenting complaints and discharge diagnoses of patients are presented in Table 2.
Presenting complaints and discharge diagnoses.
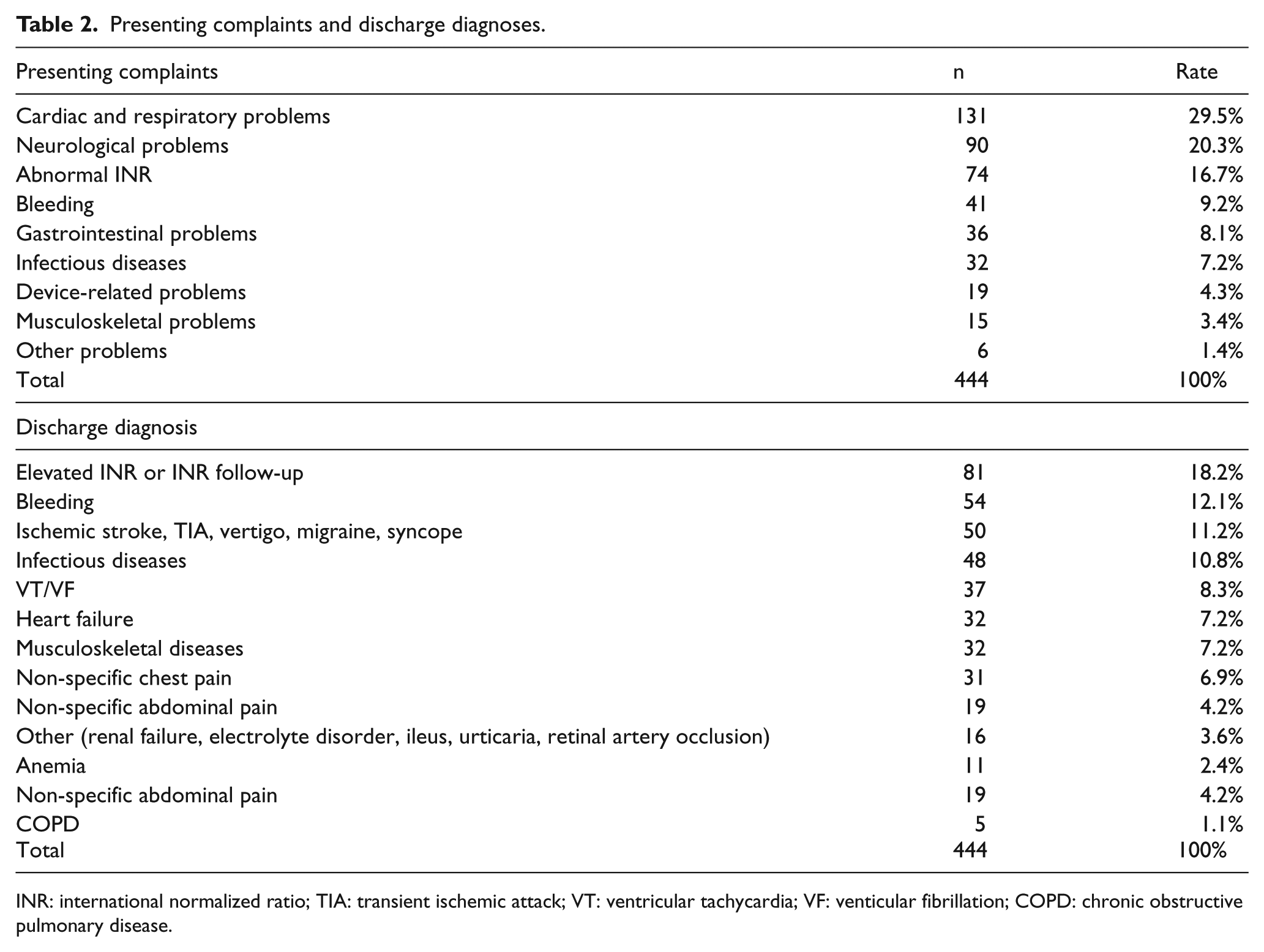
INR: international normalized ratio; TIA: transient ischemic attack; VT: ventricular tachycardia; VF: venticular fibrillation; COPD: chronic obstructive pulmonary disease.
Of the patients with bleeding, 31.1% had intracranial hemorrhage (ICH), 31.1% had epistaxis, 24% had gastrointestinal bleeding, 11.1% had hematuria, and 1.8% had gingival hemorrhage.
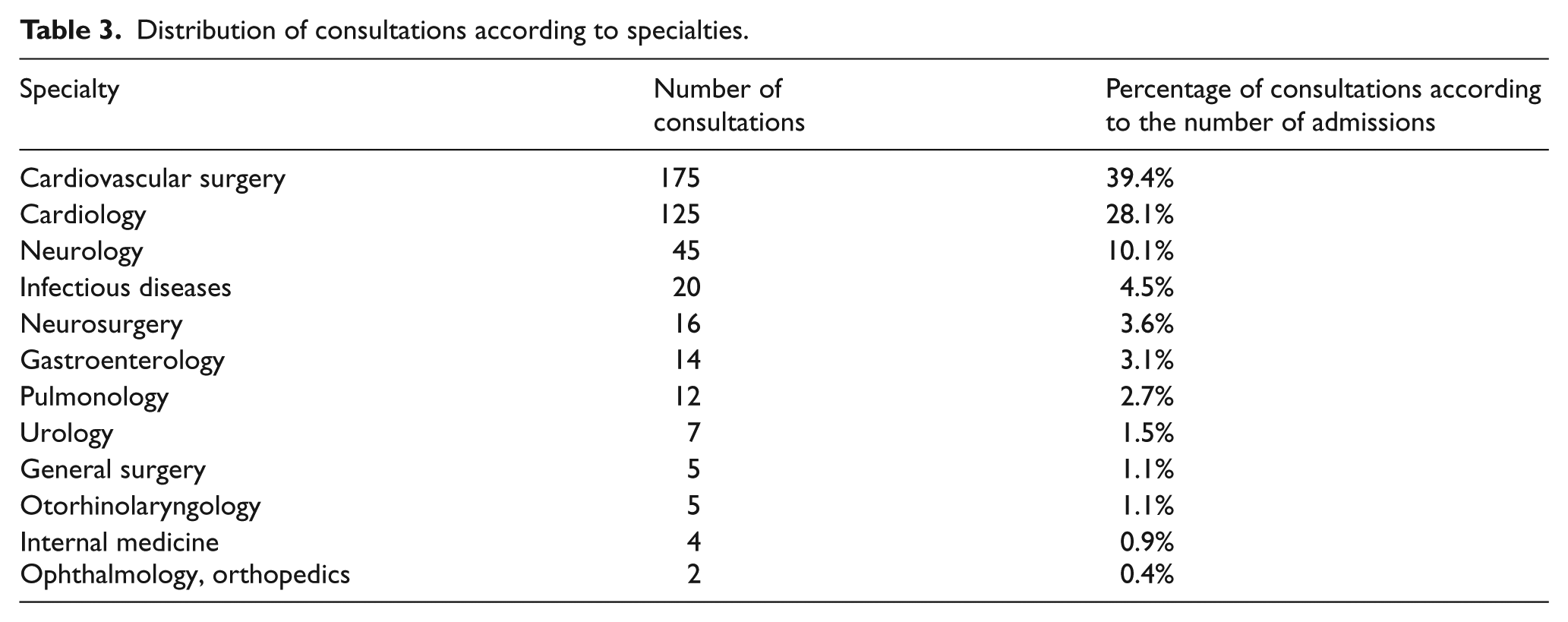
When consultations requested by ED physicians were evaluated, it was observed that no consultations were requested for 48.1% of the patients. Cardiovascular surgery was the most commonly consulted specialty (39.4%; Table 3).
Distribution of consultations according to specialties.
It was observed that 98.7% of the patients with international normalized ratio (INR)-related issues, 89.4% of the patients with non-specific abdominal pain, 68.7% of the patients with musculoskeletal disorders, 63.1% of the patients with epistaxis, 53.1% of the patients with non-device related infections, 51.6% of the patients with non-specific chest pain, 46.8% of the patients with acute heart failure, and 20% of the patients with COPD were treated and discharged solely by emergency medicine physicians, without requesting any specialty consultations (Table 4). The mean INR of patients with an INR-related discharge diagnosis was 2.29 ± 0.68, whereas the mean INR of patients with ICH was 2.98 ± 1.4.
Distribution of consultations according to diagnosis.
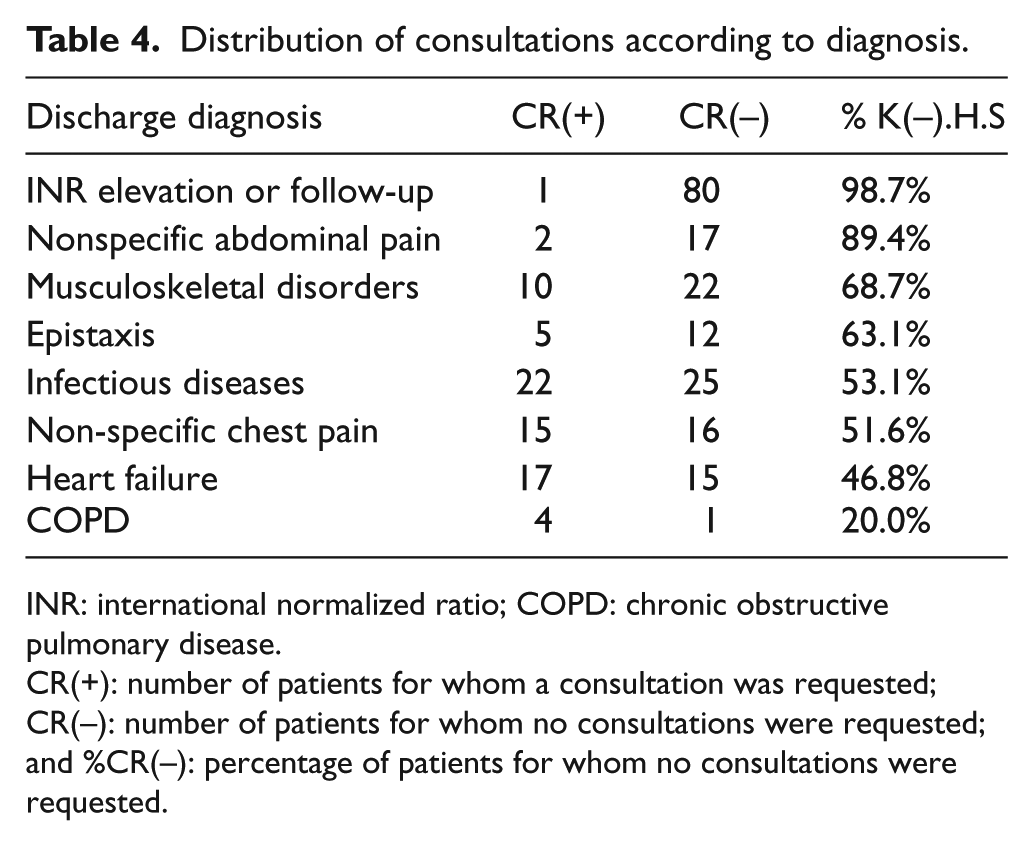
INR: international normalized ratio; COPD: chronic obstructive pulmonary disease.
CR(+): number of patients for whom a consultation was requested; CR(–): number of patients for whom no consultations were requested; and %CR(–): percentage of patients for whom no consultations were requested.
The mean length of stay in the ED was 9.7 ± 12.8 h. For the 214 patients for whom no consultations were requested, the mean length of stay in the ED was 4.3 ± 4.2 h. For the 230 patients who were consulted with other specialties, the mean length of stay in the ED was 14.8 ± 15.7 h. Of the ED admissions, 77.5% were discharged from the ED and 22.5% were hospitalized (21.2% to the intensive care unit and 1.3% to the ward). The mean hospital length of stay of the patients who were hospitalized was 2.2 ± 5.6 days. Of all patients who presented to the ED, 11.7% were admitted to the cardiovascular surgery department and 8.1% were admitted to the cardiology department. Of the patients who were admitted to the hospital, 49.5% were admitted to the cardiovascular surgery department, 34.2% were admitted to the cardiology department, and 16.3% were admitted to other departments.
Eleven patients were diagnosed with ICH, one was diagnosed with sepsis, one was diagnosed with pneumonia, and one was diagnosed with ventricular tachycardia (VT)/venticular fibrillation (VF). A total of 15 patients died. This number constitutes 15.1% of the patients included in the study. The relationships between mortality rates and gender, cause of VAD implantation, device type, and concomitant diseases (such as congestive heart failure (CHF), CAD, HT, CRF, DM, CVD, and COPD) were not found to be statistically significant. ICH was the cause of 73.3% of all deaths and 3.3% of all ED admissions. Mortality rate was statistically significantly higher in patients diagnosed with ICH compared to those without ICH (Table 5).
Relationship between intracranial hemorrhage and mortality.
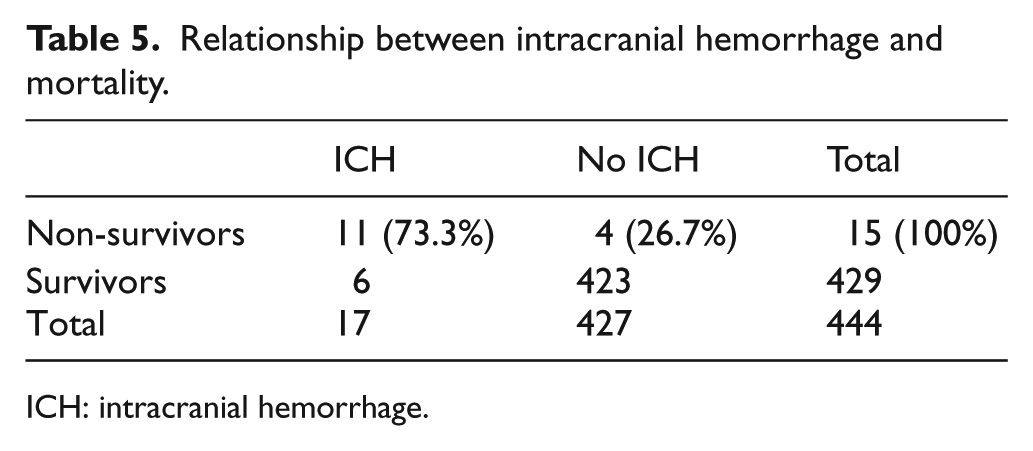
ICH: intracranial hemorrhage.
Discussion
Significant advancements in pump technologies, candidate selection, and clinical management have led to an increase in the number of patients with VADs as well as prolonging life expectancy in this patient group. In the eighth annual Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) report, the 1- and 2-year survival rates were reported to be 80% and 70%, respectively. 3 Likewise, according to the data of the cardiovascular surgery department of our hospital, the 1- and 2-year survival rates for this patient group was found to be 89% and 75%, respectively.
In a multicenter, 9-year study with 837 patients, the mean age of the patients enrolled was found to be 55 ± 14 years. 4 Similarly, in our study, the mean age was 55.5 ± 11.1 years. Most studies in the literature report that the incidence of CAD is higher among men compared to women. 5 Thus, ischemic cardiomyopathy due to CAD is more common in men compared to women.
When the devices implanted to patients were evaluated according to their brands, it was observed that the most commonly implanted brand was Heartware (Heartware, Medtronic). There are a few possible explanations for this. First, the healthcare system in our country covered only Heartware in the beginning, leading to increased experience with Heartware compared to Heartmate. Second, the smaller volume of the Heartware device renders it a better option for patients with low body mass index (BMI), including pediatric patients.
However, the risk of pump thrombosis was found to be higher with Heartmate II compared to other devices. Thus, the manufacturer stopped producing Heartmate II and developed a new generation pump called Heartmate III which, allegedly, has the lowest risk of thrombosis. However, Heartmate III is a larger device which is mostly preferred in men with high BMI.
Currently, continuous-flow VADs have replaced pulsatile VADs because of their improved durability. However, continuous-flow VADs cause a difficulty in blood pressure measurement because they usually do not produce a palpable pulse. Due to the necessity of a Doppler device to measure the blood pressure in this patient group, the blood pressure measurements of most patients in our study could not be obtained in the triage area. In our study, one of the most important shortcomings in the ED management of this patient group was the fact that the blood pressures of the patients could not be evaluated properly. In order to prevent inadequate assessment during triage, we believe that triage nurses should be trained to measure the blood pressure using Doppler ultrasound. Patients with VAD who present to our ED are transferred to the critical care section where their blood pressures are measured using Doppler USG and a manual blood pressure cuff or by radial artery cannulation. However, when we evaluated our data, we realized that special care must be taken to ensure that these patients are evaluated on admission. Studies on the ED management of patients with VAD recommend to measure the blood pressure using a Doppler device and a manual blood pressure cuff.2,6–8 Evaluating perfusion on arrival is of utmost importance because hemodynamic instability may indicate decreased preload, increased afterload, mechanical failure, dysrhythmias, infection, and bleeding. A mean arterial pressure (MAP) greater than 90 mm Hg in patients with VAD has been reported to be an important risk factor for ischemic or hemorrhagic stroke, aortic insufficiency, and pump thrombosis.9–11
Patients with VADs may present to the ED with complaints that are not related to the VAD. In our study, more than 60% of ED presentations were due to problems that were not related to VAD. Emergency medicine physicians are recommended to determine which type of device has been implanted to the patient and to contact the surgical team that implanted the VAD.7,8 In our study, regardless of whether the problem was device-related or not, cardiovascular surgery was consulted in only 39.4% of cases. We attributed this result to the fact that the emergency medicine physicians in our clinic believe that consulting a cardiovascular surgeon for every patient is unnecessary because it will not affect patient management and outcome in non-device related problems.
When the presenting complaints and diagnoses were examined in detail, it was observed that the vast majority of ED admissions were associated with warfarin sodium use, with 18.2% of the patients referring to the ED with an abnormal INR value or to get their INR levels checked. Warfarin-related or device-related bleeding was observed in 12.1% of the patients. The ED management of these patients is similar to the management of patients with bleeding who receive warfarin for other indications. Patient management is similar to non-VAD patients except for device-related infections, mechanical failure, and pump thrombosis.
In patients with suspected pump thrombosis, it is important to check the lactate dehydrogenase (LDH) level. Previous studies have shown that LDH levels increase in patients with pump thrombosis. LDH levels are typically not normal in VAD patients, even in the absence of thrombosis because these patients may have acquired Von Willebrand disease or hemolysis occurring without pump thrombosis. 12 An LDH level greater than three times the normal upper limit or a significant increase in LDH compared to the patient’s baseline value prompt evaluation for pump thrombosis. Especially, if LDH elevation is accompanied by changes in the flow and watt values of the pump or by a pump alarm, the patient may have pump thrombosis.4,13 In our study, the mean LDH level of the 12 patients who were diagnosed with pump thrombosis was 1675 ± 885 U/L (normal range: 135–225 U/L). The mean LDH levels of these patients during their previous follow-ups was 526 ± 368 U/L. In accordance with the literature, none of the patients underwent magnetic resonance imaging because the VAD devices were not magnetic resonance-compatible. 14
Length of stay in the ED may vary among hospitals. In our study, the mean ED length of stay of patients for whom a consultation was requested was more than 10 h longer than patients for whom no consultations were requested. In our study, the fact that the mean ED length of stay was 9.7 h was attributed to the fact that at our institution, patients who do not require long periods of hospital admission are discharged from the ED after necessary examinations and treatments are complete. Of the patients who presented to the ED, 22.5% were hospitalized. Of the patients who were hospitalized, 49.5% were admitted to the cardiovascular surgery clinic even if the patient was diagnosed with a non-device-related condition. This may stem from the fact that patients with VAD are regarded to be special due to the expensive and specific nature of the treatment. The leading cause of death in most studies is hemorrhagic stroke.3,6,15 Similarly, in our study, 73.3% of the patients were diagnosed with ICH and 64.7% of those diagnosed with ICH died. For this reason, when evaluating these patients in the ED, a careful neurologic examination should be performed to look for signs of ICH.
Limitations
The main limitation of this study is that it is retrospective.
Conclusion
Even though the mortality rates of patients with VAD tends to decrease, these patients still have significant morbidity due to the increase in the prevalence of VAD use. Except for device-related problems, ED management of this patient group does not differ much from other patient groups. However, it is important to determine whether the complaint is related to the device. Thus, emergency medicine physicians should have more information on the subject. As VAD implantation is a special and expensive treatment, it will be beneficial to inform the transplantation team about the ED visits of this patient group.
Case 1
A 60-year-old male patient had VAD implanted 2 years ago. He presented with sudden visual impairment and visual acuity in his right eye. On arrival to the ED, blood pressure could not be measured, and other vital signs and the neurological examination were normal. With Doppler ultrasonography and a sphygmomanometer MAP was 80 mm Hg. In computed tomography images, approximately 3.5 cm × 0.2 cm hemorrhagic area (Figure 2) was detected in the occipital region. Most noticeable in laboratory values was the INR level which was 6.4. Human prothrombin complex, intravenous vitamin K, and anti-edema treatments were started to the patient of high INR level due to warfarin use. After treatment, the INR value was 1.4. The patient was bringed to the neurosurgery consultation. The patient not planned operation and admitted to cardiovascular surgery was discharged 1 week later.
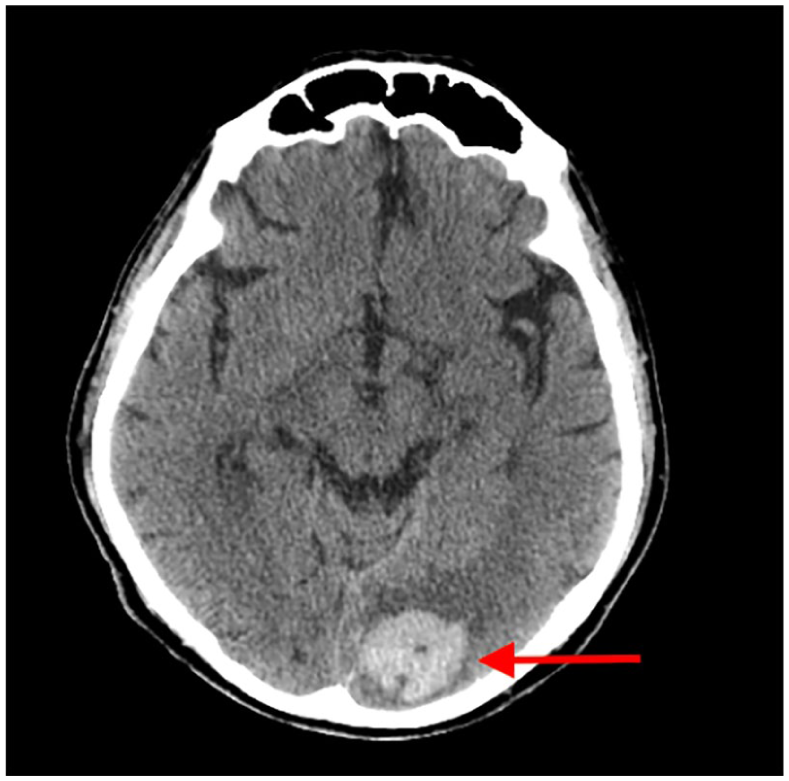
Occipital hemorrhage.
Case 2
A 64-year-old male patient had a VAD implanted 3 years ago. He had a cough, fever, and pain in the left upper quadrant for 3 days. Blood pressure was not measured on arrival, pulse: 67/min, respiratory rate: 20/min, body temperature: 38.7°C, and saturation: 94%. On physical examination, general condition was good, throat examination findings were normal, respiratory sounds were as coarse, and on the left side, thin rhonchus and long expiration were detected. Laboratory values were remarkable as white blood cell: 20.5 × 103/20 L and C-reactive protein (CRP): 25 mg/dL. The urine test was normal. The paracardiac area and the left lower lobe could not assessed in the chest X-ray due to the device on the left (Figure 3). And, with the thoracic computed tomography, pneumonic infiltration was seen in the posterior left lower lobe (Figure 4). MAP was 70/min and so the patient given antibiotic therapy was called for polyclinic control.
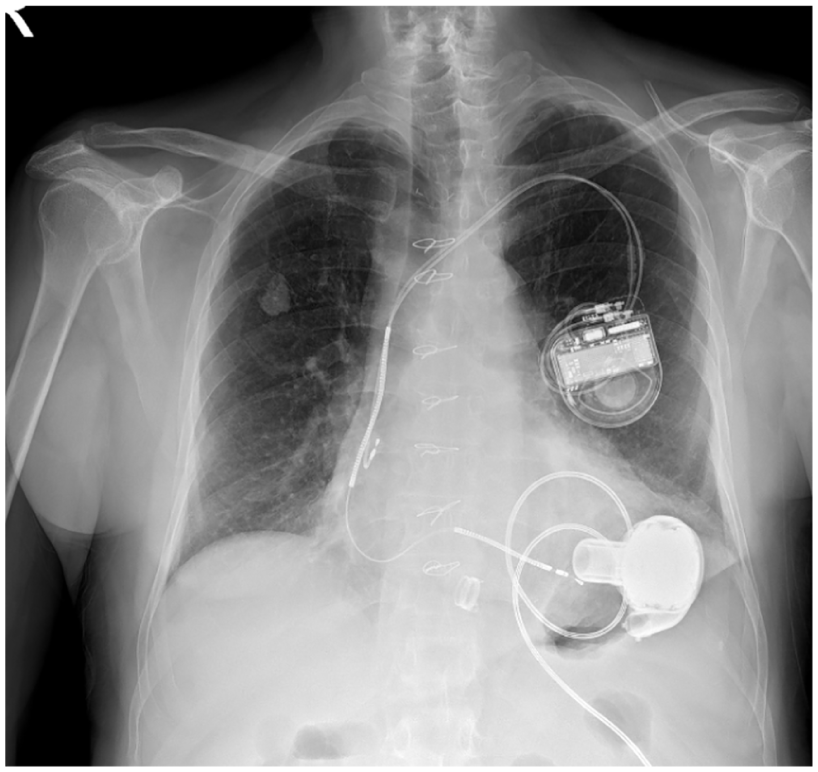
Chest X-ray.
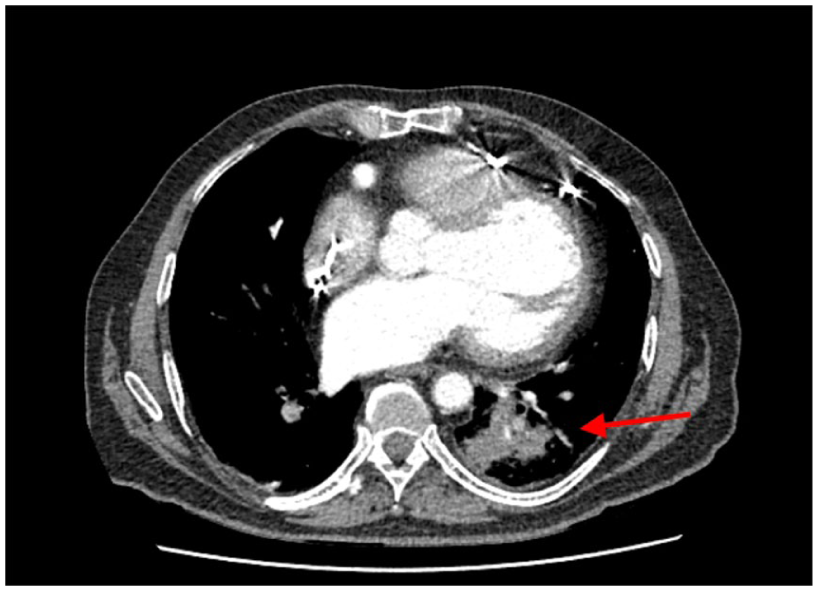
Thorax tomography.
Case 3
A 54-year-old female patient had a VAD implanted 4 years ago. With the cause of dizziness, vomiting, and nausea, she was admitted to the ED. Blood pressure was not measured at the arrival, pulse: 178/min, respiratory rate: 18/min, blood temperature: 36.8°C, and saturation: 93%. QRS tachycardia and VT torsades were revealed in electrocardiogram (ECG) (Figure 5). Synchronized cardioversion was performed with sedation. Patient returned to the normal sinus rhythm (Figure 6) was checked up by the cardiology consultant, then was admitted to the intensive care unit. After implantable cardioverter defibrillator (ICD) insertion, she was discharged.
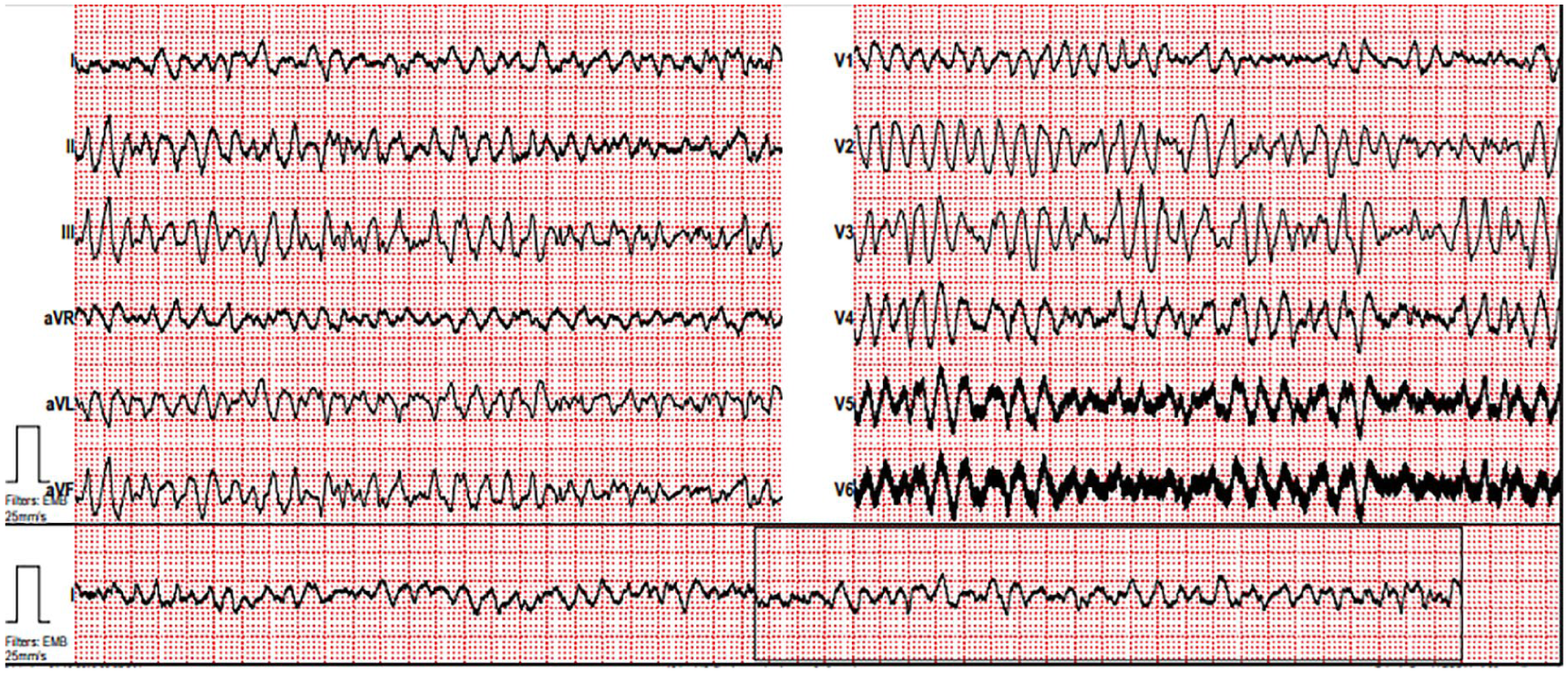
ECG-1.
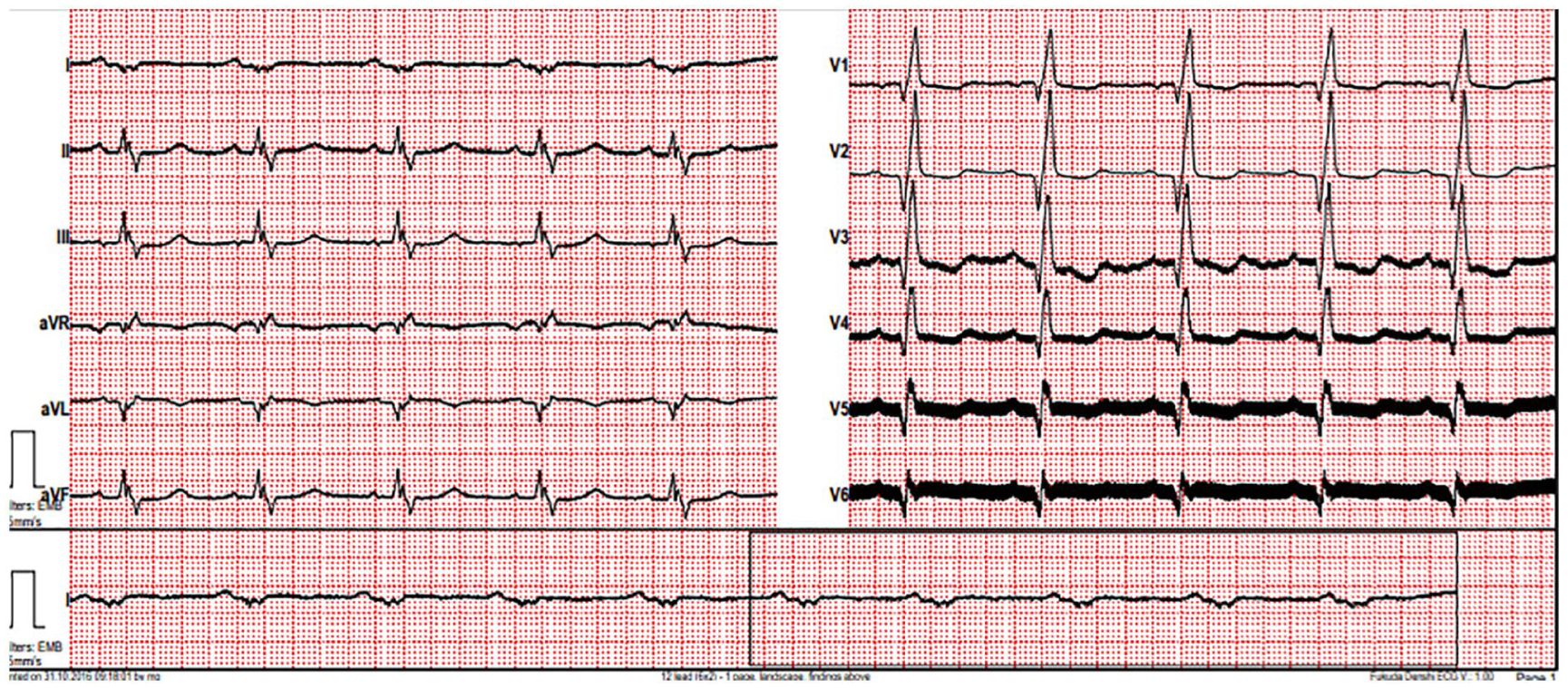
ECG-2.
Case 4
A 55-year-old male patient had a VAD implanted 1.5 years ago. He applied to the ED due to alarm of the device (high power spikes noted on his device). On arrival, blood pressure could not be measured and other vitals were normal. After monitoring, MAP was 75 mm Hg with a Doppler and a sphygmomanometer. Bed-head echocardiography showed a low diastolic flow rate at the outlet of aortic cannula. Total bilirubin: 3.65 mg/dL (N: 0.1–1), direct bilirubin: 2.49 mg/dL (N < 0.25), and LDH: 991 U/L (N: 135–225). INR was 1.7 and so pump thrombosis was considered. After cardiovascular surgery consultation, thrombolytic therapy was given and then patient was discharged.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.