
Abstract
Background:
Out-of-hospital cardiac arrest results in a high mortality rate. The 2015 American Heart Association guideline for post-cardiac arrest was launched and adopted into our institutional policy.
Objectives:
We aimed to evaluate post-cardiac arrest care and compare the results with the 2015 American Heart Association guideline and clinical outcomes of out-of-hospital cardiac arrest patients.
Methods
Included in this study were all adult patients who survived out-of-hospital cardiac arrest and were admitted to the Medical Intensive Care Unit of Songklanagarind Hospital, Thailand. The retrospective review was from 1 January 2016 to 31 December 2017.
Results:
From a total of 161 post-cardiac arrest patients admitted to the medical intensive care unit, 69 out-of-hospital cardiac arrest patients were identified. The most common cause of arrest was presumed cardiac in origin (45.0%) in which the majority was acute myocardial infarction (67.8%). Coronary intervention and targeted temperature management were performed in 27.5% and 13% of all out-of-hospital cardiac arrest patients, respectively. Survival to hospital discharge was 42%. Independent factors associated with survival to discharge were shockable rhythms, lower adrenaline doses, and the absence of hypotension at medical intensive care unit admission.
Conclusion:
Compliance with the 2015 American Heart Association post-cardiac arrest care guideline was low in our institution, especially in coronary intervention and targeted temperature management.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a public health concern. The incidence of OHCA in adult patients is approximately 350,000 and 500,000 cases annually in the United States and Europe, respectively.1–3 The reported survival rates to hospital discharge ranged from 0.2% to 37.8%.4–7
Post-cardiac arrest care is the last link in the chain of survival. 8 There is evidence that high-quality post-resuscitation care improves the chances of survival with good neurological outcomes. 9 However, protocols vary among institutions.10,11 Standard treatment protocol implementation that emphasizes an established appropriate protocol in post-cardiac arrest care improves outcomes within individual units. 12 The 2015 American Heart Association (AHA) guideline update for cardiopulmonary resuscitation and emergency cardiovascular care includes “Part 8: Post-Cardiac Arrest Care.” 13 Our institution implemented this guideline for treatment of post-cardiac arrest patients in 2015.
The 2015 AHA guideline consists of post-cardiac arrest care in seven main areas that include cardiovascular care, targeted temperature management (TTM), neurologic care, respiratory care, critical care interventions, prognostication of outcome, and organ donation. Coronary intervention is implemented in patients who are suspected of acute myocardial infarction. TTM is implemented in comatose patients. These are highlighted as the specific interventions in the adult immediate post-cardiac arrest care algorithm. 13
There are several reports regarding post-cardiac arrest care in the intensive care unit.14–16 However, since Thailand is a middle-income country, there are no audit studies in post-cardiac arrest care of OHCA patients admitted to medical intensive care units (MICUs) that follow the 2015 AHA guideline.
The objective of our study was to ascertain real-life practice for OHCA survivors admitted to an MICU and compare it with the 2015 AHA guideline and clinical outcomes of OHCA patients.
Materials and methods
Design
A retrospective descriptive approach was used. The study was approved by The Research Ethics Committee of the Faculty of Medicine, Prince of Songkla University (REC 60-462-14-1). Patient consent to review the medical records was not required because the electronic medical records data were anonymous, confidential, and not linked to the individuals.
Setting
The retrospective audit was conducted at an MICU in Songklanagarind Hospital, Thailand. This hospital is an 816-bed university-affiliated hospital that has a 10-bed MICU. OHCA survivors at the emergency department (ED) were subsequently admitted to the MICU. At the time of our study, cardiopulmonary resuscitation (CPR) and post-cardiac arrest management followed the 2015 AHA guideline. The TTM protocol was launched in our hospital in October 2012 and included comatose post-cardiac arrest patients whether the initial electrocardiography (ECG) indicated shockable rhythms or not. However, the final decision for TTM was made by an on-duty MICU attending physician. Three cardiologists and two cardiac interventionists were the on-call consultants and made the decision to perform cardiac intervention.
Sample
The eligibility for inclusion in this study were adult patients ⩾18 years, suffered an OHCA, required ED management, and survived to be admitted to the MICU from 1 January 2016 to 31 December 2017. Referred patients or patients who died in the ED were excluded.
Data collection
The data included in this study were collected from the MICU database and the electronic hospital information system. The collected data included baseline characteristics, cardiovascular care (i.e. coronary angiography (CAG), percutaneous coronary intervention (PCI)), TTM, neurologic care, respiratory care, and critical care interventions. Patients were followed until discharge from the hospital or death whichever occurred first. Neurological outcomes were defined using the Cerebral Performance Category (CPC) score. 17 The CPC scores ranged from 1 to 5, where 1 = good cerebral performance or minor disability, 2 = moderate cerebral disability (function is sufficient for independent activity of daily life), 3 = severe cerebral disability, 4 = coma or vegetative state, and 5 = brain death. Good neurological outcomes were classified if the CPC score at hospital discharge was ⩽2.
Primary and secondary outcomes
The primary outcomes were the proportion of patients who received post-cardiac arrest care following the 2015 AHA guideline 13 and the focus was on (1) CAG that should be performed immediately on OHCA patients suspected of acute myocardial infarction (ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction) and (2) all comatose OHCA patients who had TTM if there were no contraindications. The secondary outcomes were survival to hospital discharge, neurological outcomes, and factors associated with survival to hospital discharge.
Statistical analysis
Data were summarized using descriptive statistics. Categorical data were demonstrated as percentages. Continuous data are shown as median with minimum and maximum and interquartile range (IQR) that depended on the distribution of the data. The data were tested for normality using the Kolmogorov–Smirnov goodness-of-fit test. Selected variables with p < 0.1 were introduced into a multiple logistic regression model after testing for association. Odds ratios and their 95% confidence intervals (CIs) were used to identify the significant independent factors that influenced in-hospital mortality. Two-tailed values of p < 0.05 were deemed statistically significant. All statistical analyses were computed with R software version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 161 post-cardiac arrest patients were admitted to the MICU during the 2-year period. More than half of the patients (87/161, 54%) suffered from OHCA. When the referred patients were excluded, 69 patients were included and analyzed (Figure 1). The baseline characteristics are shown in Table 1. Although the majority of the patients were witnessed cardiac arrest (88.4%), 34.8% of the patients received bystander CPR. The common initial rhythm was non-shockable (74.0%). The median CPR time was 11 min (IQR: 6–20), the most common cause of cardiac arrest was cardiac cause (45.0%), and the majority (67.8%) was acute myocardial infarction.
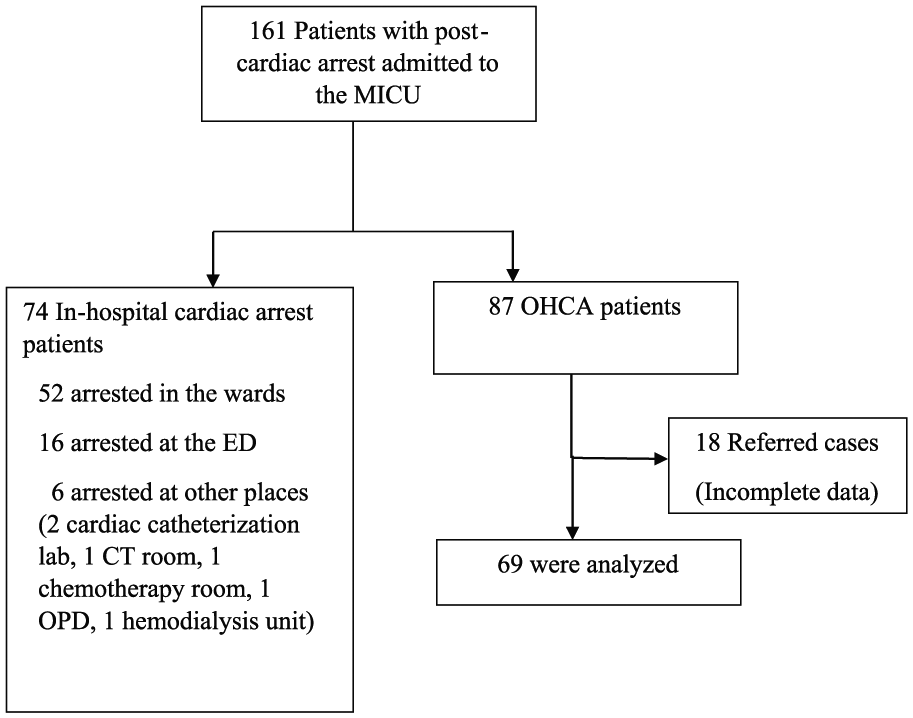
Flow diagram.
Baseline patient characteristics (N = 69).
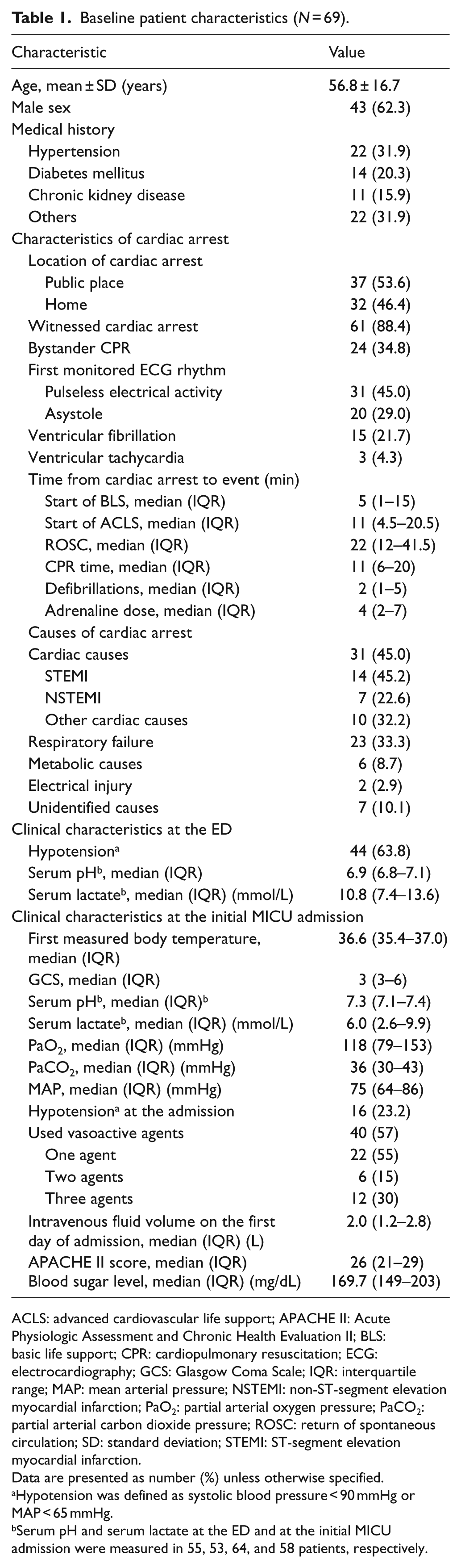
ACLS: advanced cardiovascular life support; APACHE II: Acute Physiologic Assessment and Chronic Health Evaluation II; BLS: basic life support; CPR: cardiopulmonary resuscitation; ECG: electrocardiography; GCS: Glasgow Coma Scale; IQR: interquartile range; MAP: mean arterial pressure; NSTEMI: non-ST-segment elevation myocardial infarction; PaO2: partial arterial oxygen pressure; PaCO2: partial arterial carbon dioxide pressure; ROSC: return of spontaneous circulation; SD: standard deviation; STEMI: ST-segment elevation myocardial infarction.
Data are presented as number (%) unless otherwise specified.
Hypotension was defined as systolic blood pressure < 90 mmHg or MAP < 65 mmHg.
Serum pH and serum lactate at the ED and at the initial MICU admission were measured in 55, 53, 64, and 58 patients, respectively.
General MICU care
The majority of the patients were comatose (median Glasgow Coma Scale score: 3, IQR: 3–6) and had hypotension at MICU admission (16/69, 23.2%). Mechanical ventilation was provided in all patients to provide adequate ventilation and oxygenation. Vasoactive agents were used in 57%, and the most common agent was norepinephrine (22/40, 55%). An insulin protocol was used to control blood sugar and the median blood sugar level was 169.7 mg/dL (Table 1).
Specific procedures
Coronary intervention
In the cases of diagnosed acute myocardial infarction (n = 21), CAG was done in 11/21 (52.4%) and PCI in 9/21 (42.9%). The median time from return of spontaneous circulation (ROSC) to CAG was 3 h (IQR: 2–4; Table 2). The two most common culprit lesions were located at the left anterior descending and right coronary arteries (4/9, 44%).
Procedures (N = 69).
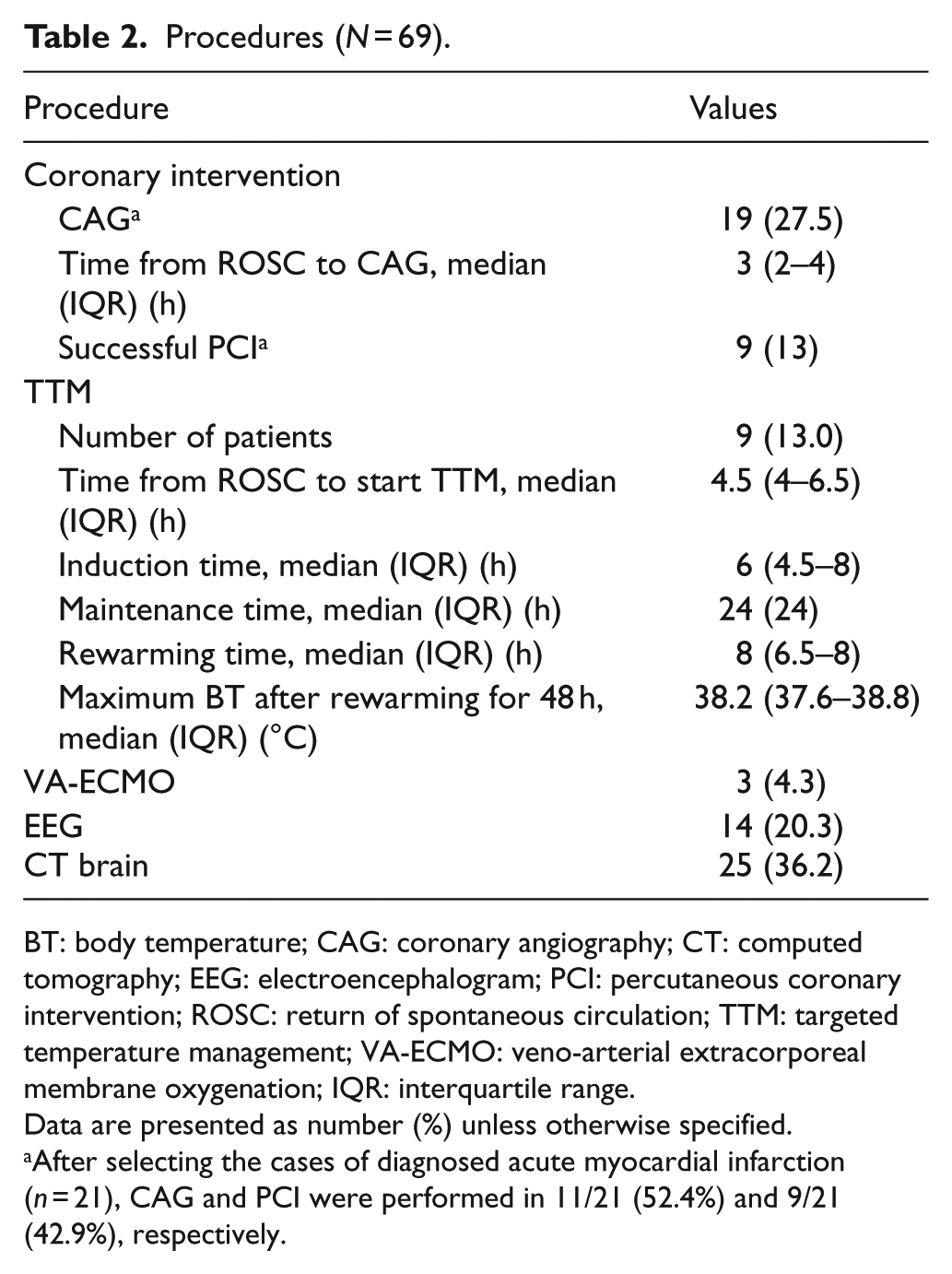
BT: body temperature; CAG: coronary angiography; CT: computed tomography; EEG: electroencephalogram; PCI: percutaneous coronary intervention; ROSC: return of spontaneous circulation; TTM: targeted temperature management; VA-ECMO: veno-arterial extracorporeal membrane oxygenation; IQR: interquartile range.
Data are presented as number (%) unless otherwise specified.
After selecting the cases of diagnosed acute myocardial infarction (n = 21), CAG and PCI were performed in 11/21 (52.4%) and 9/21 (42.9%), respectively.
TTM
When the excluded patients were those who could follow verbal commands (n = 10) and those who had hemodynamic instability (n = 14), TTM was done in 9/45 cases (20%). When we selected patients with shockable rhythms, TTM was performed in 5/14 patients (35.7%). All TTM procedures were started at the MICU with a median time of 4.5 h after ROSC. Patients were cooled to 33°C in a median time of 6 h, maintained for 24 h, and then rewarmed at a rate of 0.25°C–0.5°C per hour (Table 2).
Electroencephalography
Continuous electroencephalography (EEG) monitoring was not provided in any of the patients. The neurologists were consulted and EEG monitoring was performed in suspected seizure or non-convulsive status epilepticus. EEG monitoring was performed in 20.3% which found status epilepticus in 4.3% (Tables 2 and 3).
Patients outcomes (N = 69).
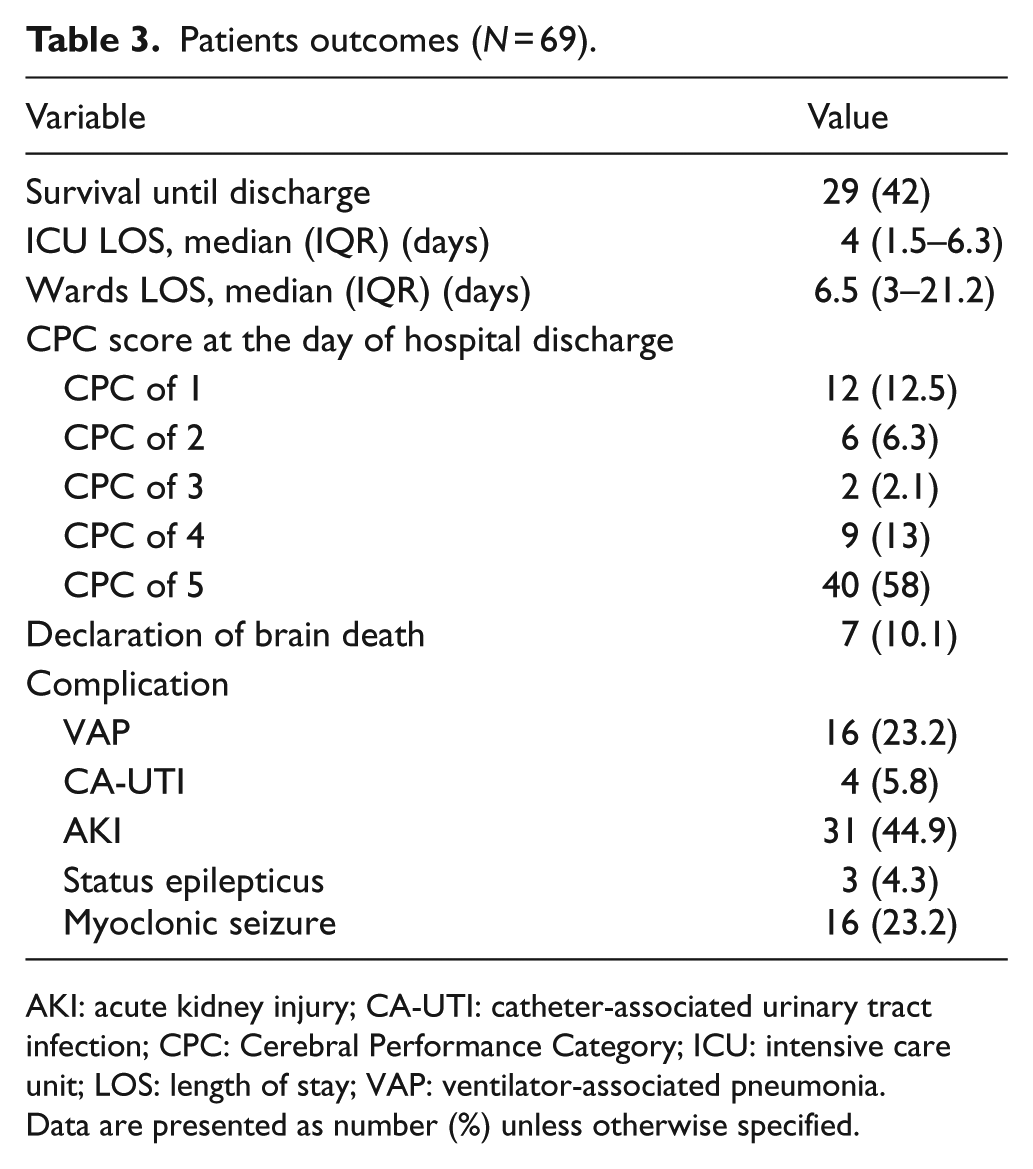
AKI: acute kidney injury; CA-UTI: catheter-associated urinary tract infection; CPC: Cerebral Performance Category; ICU: intensive care unit; LOS: length of stay; VAP: ventilator-associated pneumonia.
Data are presented as number (%) unless otherwise specified.
Veno-arterial extracorporeal membrane oxygenation
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was performed as extracorporeal CPR in three cases (Table 2). Only one of the three patients survived and was discharged with good neurological status.
Patient outcomes
The survival rate at hospital discharge was 42% (29/69). For those patients who survived, 62% (18/29) had good neurological outcomes (CPC 1–2; Table 3). When adjusted for severity, the factors associated with survival to hospital discharge were shockable rhythm, lower adrenaline dose, and the absence of hypotension at MICU admission (Table 4).
Multiple logistic regression analysis of the factors associated with survival to discharge by adjusted odds ratio (aOR).
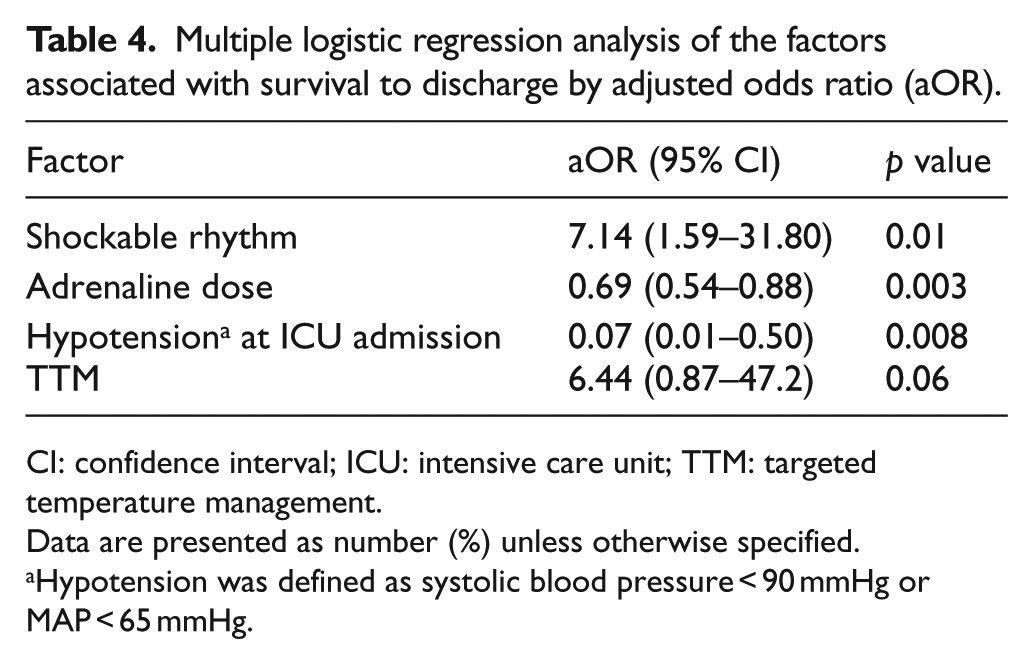
CI: confidence interval; ICU: intensive care unit; TTM: targeted temperature management.
Data are presented as number (%) unless otherwise specified.
Hypotension was defined as systolic blood pressure < 90 mmHg or MAP < 65 mmHg.
Discussion
To our knowledge, this is the first Thai audit study of post-cardiac arrest management at an MICU. This may be reflective of the real-life practice of an MICU in a middle-income country after launching the 2015 AHA guideline. There were some issues that deviated from the standard guideline.
Over half of the patients developed cardiac arrest in a public place. Most of them were witnessed cardiac arrest but bystander CPR was very low (34.8%). The median times from the cardiac arrest event to the start of basic life support and advanced cardiovascular life support were 5 and 11 min, respectively. The numbers of witnessed arrest patients and bystander CPR in this report were not quite different from our previous report 18 and other studies in Thailand.19,20 The chain of survival is weak in low- to middle-income countries.21,22 The small number of bystander CPR events in our report reflected the levels of awareness, knowledge, and skills of the people. We encourage the general public to incorporate mandatory basic life support curriculum in secondary or high schools and workplaces. Emergency medical service (EMS) utilization in Thailand is low and also problematic. 20 Some patients in our study were transported to the hospital in private vehicles without CPR or without activation of the EMS system similar to a case report from Hanoi, Vietnam. 23 Thailand, Malaysia, and Vietnam have hospital-based EMS systems that differ from other Asian countries that have fire department–based systems. 24 Shorter EMS response time is associated with neurologically intact survival. 25 We suggest developing a Thai EMS network using community and fire department involvement to improve the chance of survival in cardiac arrest patients.
Although the most common cause of arrest in our patients was cardiac, coronary interventions were performed in only 27.5%. For selected acute myocardial infarction, these interventions were done in only 52.4%. The median time from ROSC to CAG was 3 h (IQR: 2–4). Multiple observational studies demonstrated better survival in both ST-segment elevation myocardial infarction and non-ST-segment myocardial infarction post-cardiac arrest patients who received immediate CAG and PCI (when indicated) compared to those that did not receive immediate CAG.26–28 According to the 2015 AHA guideline, CAG should be performed immediately in OHCA patients with presumed cardiac cause of arrest and ST-elevation on ECG whether the patient is comatose or awake. 13 The reasons for poor guideline compliance were due to the lack of a protocol for CAG in OHCA patients, cardiac interventionists who selected favorable prognosis cases for CAG from their own personal experience, and dependence on the availability of a catheterization lab. Coronary intervention needs costly equipment and experienced interventionists who are not available in every tertiary care hospital in Thailand. We suggest selected patients who have favorable clinical features 29 to be the first priority with fast tract to receive coronary intervention in the nearest hospital.
About two-thirds of patients developed hypotension after ROSC. The median mean arterial pressure (MAP) in our report was 75 mmHg. Some patients (16/69, 23.2%) had a MAP less than 65 mmHg at the time of ICU admission. The guideline recommends correction of hypotension (systolic blood pressure less than 90 mmHg or MAP less than 65 mmHg) during post-resuscitation care. 13 Most of our patients with hypotension (14/16, 87.5%) were very severe and finally died in the hospital. Hypotension was also one of the factors associated with in-hospital mortality in our report.
The 2015 AHA guideline recommends TTM for comatose adult patients with ROSC whether or not they have shockable rhythms. 13 Our institution has a protocol for TTM but it was performed in only 20% of our comatose OHCA patients. A previous report from seven Asian countries revealed that TTM was performed in only 1% of OHCA patients. 24 The final decision to start TTM is up to the attending ICU physician which is one reason for the deviation from the guideline. All TTM procedures were started at the MICU. This explained the median time of 4.5 h (IQR: 4–6.5) from ROSC to induction. A study reported that the pre-induction time was independently associated with good neurological outcomes at hospital discharge. 30 Our patients had a median maximum body temperature after rewarming of 38.2°C. Studies showed a worse outcome in hyperthermia patients during the first few days of cardiac arrest.31,32 Therefore, the guideline recommends preventing fever in comatose patients after TTM. We recommend establishing a local protocol for TTM adapted to the available infrastructure and equipment. In resource-limited institutions, the TTM protocol should be selective in patients with initial shockable rhythm and who received bystander CPR which is associated with a higher chance to improve neurological outcome and survival. 33
Some of our patients developed myoclonic seizure (23.2%) and status epilepticus (4.3%) during MICU admission. EEG monitoring was performed only in 20.3% of cases. The guideline recommends that EEG should be monitored frequently or continuously in comatose patients after ROSC. 13 The recommendations were not followed because our institution had only two portable EEG devices and the technicians were not available at night or on the weekends.
The respiratory care in our MICU provided more than adequate oxygenation (median PaO2: 118 mmHg) and ventilation (median PaCO2: 36 mmHg). The guideline suggests maintaining normocarbia (PaO2: 35–45 mmHg) and avoiding hypoxia in adults with ROSC after cardiac arrest. 13 Evidence shows that hyperoxia (PaO2 > 300 mmHg) is independently associated with an increased in-hospital mortality.34,35 Seven patients (7/69) had hyperoxia, of which three (3/7, 42.9%) died in the hospital.
Our patients had a median blood glucose level of 169.7 mg/dL. Nowadays, the benefit of target control of blood glucose is uncertain in post-cardiac arrest patients. We followed the results from a controlled trial in critically ill patients that suggested keeping the blood sugar level less than 180 mg/dL using our insulin protocol. 36
The survival rate until ICU discharge in our report was 42%. Our findings were similar to a report of in-hospital mortality which averaged 60% in post-cardiac arrest patients admitted to an ICU with an inter-institutional variability of 40%–80%. 11 Shockable rhythms, adrenaline dose, and hypotension at the MICU admission were the factors associated with survival until hospital discharge as in our previous report 37 and other studies.12,16 TTM was associated with survival but it was not statistically significant. However, since the frequency of the TTM procedure was quite low, the power was not sufficient to show a benefit in our study.
Although the diagnosis of brain death was done in the ICU (7/69, 10.1%), no organ donation was documented. The rate of organ donation is quite low in Thailand. It depends on the patients, religious beliefs of the relatives, the neighbor effect, 38 preparedness of the transplant center, and national policy.
Our findings suggested that many interventions need to be developed to improve post-cardiac arrest care to maximize patient outcomes, such as basic life support training for the layman, establishing a protocol for CAG, strictly following the TTM guideline, providing EEG monitoring, and encouraging organ donation. These interventions are needed for institutional policy and multidisciplinary co-operation.
There were a number of limitations that should be considered when interpreting the findings of our study. This study has inherent limitations due to the retrospective nature of the audit. Some data were not available and it was not possible to understand the rationale behind the decision of care. This study was a single-center study that may not reflect other institutions.
Conclusion
The 2015 AHA guideline in post-cardiac arrest care was not adopted into the real-life practice in the MICU of a middle-income country, especially in coronary intervention and TTM. Our findings suggest establishing an institutional policy with a multidisciplinary approach to achieve compliance with the standard guideline.
Footnotes
Acknowledgements
The authors gratefully acknowledge Mr Glenn Shingledecker in the International Affairs Department, Faculty of Medicine, Prince of Songkla University for the language correction services. All authors contributed to data analysis and drafting and revision of the paper and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethical approval
The study was approved by The Research Ethics Committee of the Faculty of Medicine, Prince of Songkla University (REC 60-462-14-1).
Human rights
This research was conducted according to the World Medical Association Declaration of Helsinki.
Informed consent
Patient consent to review the medical records was not required because the electronic medical records data were anonymous, confidential, and not linked to the individuals.