
Abstract
Background:
High-quality chest compression is crucial for cardiac arrest patients. However, only few studies are focusing on the optimal compression point.
Objective:
The aim of this study was to explore the optimal compression point based on chest-computed tomography.
Methods:
We retrospectively selected 166 adult health subjects between January 2018 and May 2018 in a university-affiliated hospital.
Results:
The median length of sternum was 14.9 cm. The median length from the inter-nipple line to the distal end of sternum was 1.0 cm. The median length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum was −1.4 (–2.2 to 0.0) cm. The median value of the length from the inter-nipple line to the distal end of sternum plus the length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum was 2.0 (1.0–3.1) cm.
Conclusion:
One size does not fit all. The point recommended by the current guideline may not appropriate for Chinese person. Further studies are required focusing on individual chest compression during cardiopulmonary resuscitation.
Introduction
Cardiac arrest has an annual incidence rate of approximately 20–140 per 100,000 people in the general population. 1 The survival to hospital discharge of patients with out-of-hospital cardiac arrest is about 3%-10%.2–5 High-quality cardiac pulmonary resuscitation (CPR) with appropriate compression depth, compression rate, and complete chest recoil is associated with better prognosis.6–9 The optimal chest compression point is crucial for effective CPR. 10 However, there are few studies that focus on this topic. The inter-nipple line was recommended for chest compression in previous guidelines. The recent American Heart Association (AHA) guideline states that the rescuer should place the heel of the hand on the lower half of sternum for chest compression. 11 The aim of this study was to explore the optimal chest compression point using chest-computed tomography.
Methods
Inclusion and exclusion criteria
We retrospectively selected adults who took health examination between 1 January 2018 and 1 May 2018 in a university-affiliated hospital. Inclusion criteria were as follows: age ⩾18 years and people who received chest-computed tomography (CT) exams. Exclusion criteria were as follows: people with valvular disease, dilated cardiomyopathy, myocarditis, severe thorax deformity, various chest trauma, or thoracic surgery or other diseases that might result in mediastinal displacement or deformation of chest and heart would be excluded. The detailed individual information was extracted from an electronic patient record (EPR) system.
Chest-CT techniques
A total of 64 channel multi-detector row CT was performed with standard technique (SOMATOM Definition Flash (slice thickness is 1.5 mm), followed by three-dimensional (3D, Siemens) reconstruction. The data collected were as follows: length from the inter-nipple line to the distal end of the sternum; the main structures under the inter-nipple line; length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum; and sternum length. CT axial image was used for location, and sagittal reconstruction image was used for measure (Figure 1). Two radiologist read each CT images independently. Finally, any discrepancy was resolved by discussion or consultation with the third radiologist.
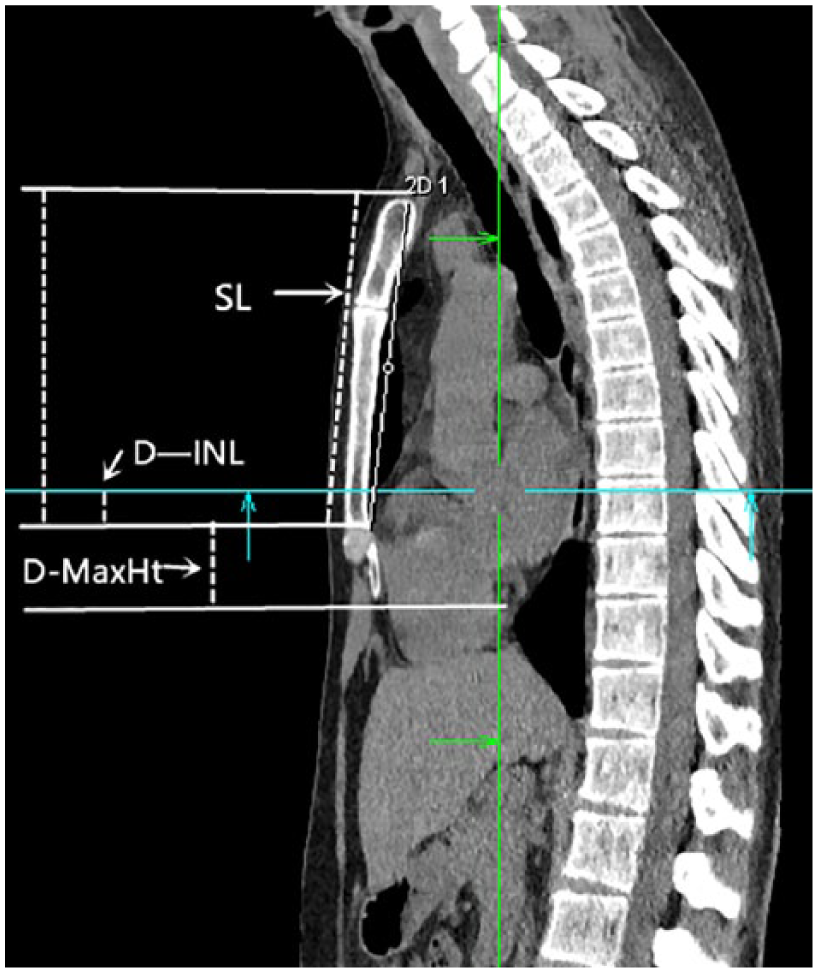
The sagittal image of chest-computed tomography.
Statistical analysis
Baseline characteristics of included people were described using descriptive statistics. Category variables were described as counts and proportions; continuous variables were described using mean (standard deviation (SD)) or median (interquartile range (IQR)) according to their data distribution. Difference of continuous variables between groups was found using t test or Mann–Whitney U test. Difference of category variables between groups was found using Chi-square test, Fisher test, or Mann–Whitney U test. Subgroup analysis was performed according to different body mass index (BMI, <24 vs ⩾24). The agreement between two measurers was found using interclass correlation coefficient. A value of p < 0.05 was considered statistically significant.
Results
A total of 166 objects were included in this study. The median age of cases at baseline was 48 (42–55) years. Among them, 70.5% (117) of participants were male. The median BMI of included objects was 24.0 (21.3–25.9). Around 48.2% (81) of participants were diagnosed with overweight or obese. The median length of sternum was 14.9 (14.0–15.8) cm, and there was significant difference between genders (15.4 (14.8–16.1) cm for men vs 13.5 (13.1–14.1) cm for women, p < 0.001).
In 78 (59%), 30 (18.1%), and 38 (22.9%) subjects, the inter-nipple line were above, below, and coincident with the distal end of sternum, respectively. There was no significant difference between genders (p = 0.13). The median length from the inter-nipple line to the distal end of sternum was 1.0 (0.0–1.9) cm, with no statistic difference between two BMI groups (p = 0.6). In addition, we found the most intrathoracic structures just underneath the inter-nipple line were aortic sections (including ascending aorta and aortic root, 28.3%), left atrium (LA, 63.9%), left ventricle (LV, 50.6%), right atrium (RA, 39.8%), right ventricle (RV, 63.3%), and left ventricular outflow tract (LVOT, 33.7%).
In 21 (12.7%), 111 (67.5%), and 33 (19.9%) subjects, the point at which the maximal left ventricular diameter projected onto the sternum was above, below, and coincident with the distal end of sternum. And among male subjects, the aforementioned values were 16 (13.7%), 72 (61.5%), and 29 (24.8%). Among female subjects, the aforementioned values were 5 (10.2%), 40 (81.6%), and 4 (8.2%). There was statistical difference between different genders (p = 0.03). In addition, the aforementioned values in subjects with a BMI <24 versus ⩾24 were 9 (10.6%), 63 (74.1%), and 13 (15.3%); 12 (14.8%), 49 (60.5%), and 20 (24.7%), respectively. There was no statistical difference between two BMI groups (p = 0.2). The median length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of sternum was −1.4 (–2.2 to 0.0) cm. This length in patients with a BMI <24 was −1.7 (–2.3 to 0.0) cm; and in patients with a BMI ⩾24 was −1.2 (–2.1 to 0.0) cm. The results indicated the point at which the maximal left ventricular diameter projected onto the sternum below the distal end of the sternum and was associated with BMI. And people with lower BMI had greater distance between the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum. Furthermore, we performed a post hoc subgroup analysis based on the median height (height ⩽166.0 cm vs height >166.0 cm). The percentage of subjects with the point at which the maximal left ventricular diameter projected onto the sternum above, below, and coincident with the distal end of sternum was 11.1%, 76.5%, and 12.3%, respectively, in patients with a height ⩽ 166.0 cm. And the percentage of subjects with the point at which the maximal left ventricular diameter projected onto the sternum above, below, and coincident with the distal end of sternum was 14.1%, 58.8%, and 27.1%, respectively, in patients with a height >166.0 cm. The median length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of sternum was −1.6 and −1.15 cm in patients with a height ⩽166.0 versus >166.0 cm. These results indicated people with lower height had greater distance between the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum.
In addition, we also calculated the difference using the length from the inter-nipple line to the end of sternum plus the length from the point at which the maximal left ventricular diameter projected onto the sternum to the distal end of the sternum. The results showed the median value was 2.0 (1.0–3.1) cm. And in 144 (86.7%) subjects, the inter-nipple line was above the point at which the maximal left ventricular diameter projected onto the sternum.
Discussions
The results of this study showed that in most people, the point at which the maximal left ventricular diameter projected onto the sternum was below the distal end of sternum. And the inter-nipple line may not be the optimal compression point.
As we all know, high-quality CPR could improve the prognosis of patients with cardiac arrest.12,13 Till now, most studies focus on compression frequency, compression depth, and complete chest recoil, but fewer studies underline the optimal chest compression point. 10 The optimal compression point should be effective in generating perfusion pressure, easily identified, and associated with fewer complications. In the past few decades, the compression point described in different guidelines did not change significantly.11,14 And the lower part of sternum is recommended for hand placement by the AHA guideline, 11 based on the results of two small studies.15,16 In the study by Cha et al., 15 the authors found SPO2 and peak arterial pressure were higher in patients who received external chest compression at the lower end of the sternum than those who received standard chest compression. In another study by Qvigstad et al., the authors compared the point at the center between two nipples with another three different points. They found that there was no significant difference of end-tidal CO2 pressure between the groups. 16 Thus, the authors concluded that the optimal compression points might vary for different patients. 16
In the past, the inter-nipple line was recommended for chest compression. Moreover, several studies reported that chest compression at the midpoint of the inter-nipple line might be much safer.17–19 In this study, we found that the main underlying anatomical structures of this point were LA, RV, and LV, which were similar to the results reported in several previous studies.10,20,21 Moreover, we found that the point at which the maximal left ventricular diameter projected onto the sternum was much lower than the center of the inter-nipple line. These results indicate that the midpoint of the inter-nipple line might not be the optimal chest compression point.10,20
In 2016, Nestaas et al. explored the optimal compression point through magnetic resonance imaging. They proposed that the optimal compression point might be 3 cm left of the junction of sternum and inter-nipple line. 22 Choi et al. 23 put forward that CPR providers need to palpate the suprasternal notch using the little finger and placing the hand heel one heel width from the suprasternal notch. Zhang et al. 24 and Li et al. 25 in their pilot study, even reported active abdominal lifting and CPR could obtain better results in certain situations, including patients with chest wall deformity, rib fracture, or hemopneumothorax. In this study, in most objects, the point at which the maximal left ventricular diameter projected onto the sternum below the end of sternum was similar to the results of a previous published study. 12
Insights into further study
The optimal compression point may be associated with the main mechanisms driving effective blood flow. Currently, “cardiac pump theory” and “thoracic pump theory” are two mainly accepted mechanisms. In addition, Ma et al. 26 put forward the third mechanism (left atrium pump). Georgiou et al. 27 systematically reviewed studies focusing on these mechanisms and concluded that both theories might be useful. With the development of science and technology, like invasive/non-invasive measurements, echocardiography, radiolabeled microspheres, 3D printing, simulation model and 3D finite element analysis model, the main mechanism may be elucidated in future studies. The prognosis of patients with cardiac arrest varies, and the survival rate of these patients in developing countries is lower than that in developed countries. 28 One of many factors that may account for this inconsistent outcome is low-quality CPR. The results of a previous study we published showed chest compression with 5–6 cm depth might be inappropriate in Chinese people, and the optimal compression depth should be the one-fourth to one-third of external anteroposterior diameter of their thoracic diameter. 29 Along with the results of this study, individual CPR may be required. In the future, an automatic mechanical CPR device or an artificial-intelligence robot, being able to identify the optimal compression point by ultrasonography or other mechanisms, being able to measuring exactly the external anteroposterior diameter of the patient’s thoracic, being able to make real-time feedback on quality of CPR, may become available.
Limitations of this study
First, the results of this study were based on static measure and may be different from reality during dynamic CPR. Second, linear measurement was used in this study, which could have biased the results. Third, the limited sample size and all included objects were Chinese may affect the generalization of this study’s results.
Conclusion
The result of this study showed that the optimal chest compression point might be below the end of the sternum. And individualized chest compression should be the focus of further studies.
Footnotes
Acknowledgements
The authors are grateful for the help of all physicians in the Department of Emergency Medicine, The Second Affiliated Hospital, School of Medicine, Zhejiang University. J.M. and L.J. are co-first authors of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Zhejiang medical and health science and technology project (Grant No.: 2017ky372).
Availability of data and materials
The data sets used in this study are available from the corresponding author on reasonable request.
Ethical approval
The study was approved by the ethical committee of The Second Affiliated Hospital, School of Medicine of Zhejiang University.
Informed consent
Due to the retrospective nature of the study, informed consent was waived.