
Abstract
Background:
The cervical collar has been used as a common device for the initial stabilization of the cervical spine. Although many cervical collars are commercially available, there is no consensus on which offers the greatest protection, with studies showing considerable variations in their ability to restrict cervical range of motion. The use of the XCollar (Emegear, Carpinteria, CA) has been known to decrease the risk of spinal cord injury by minimizing potential cervical spinal distraction. We compared XCollar with two other cervical collars commonly used for adult patients with cervical spine injury to evaluate the difference in effectiveness between the three cervical collars to restrict cervical range of motion.
Objectives:
This study aimed to evaluate the difference between the three cervical collars in their ability to restrict cervical range of motion.
Method:
A total of 30 healthy university students aged 21–25 years participated in this study. Participants with any cervical disease and symptoms were excluded. Three cervical collars were tested: Philadelphia® Collar, Stifneck® Select™ Collar, and XCollar. A digital camera and an image-analysis technique were used to evaluate cervical range of motion during flexion, extension, bilateral bending and bilateral axial rotation. Cervical range of motion was evaluated in both the unbraced and braced condition.
Results:
XCollar permitted less than a mean of 10° of movement during flexion, extension, bilateral bending and bilateral axial rotation. This was less than the movement permitted by the other two cervical collars.
Conclusion:
XCollar presented superior cervical immobilization compared to the other two commonly used cervical collars in this study. Thus, when cervical collar is considered for an adult patient with cervical spine injury, XCollar might be one of the considerate options as a cervical immobilization device.
Introduction
Cervical spine immobilization techniques are used to limit head and neck movement to minimize the risk of introducing or exacerbating spinal cord injury (SCI) in trauma patients.1,2 Although SCI is uncommon in total pre-hospital trauma patients, exacerbation of SCI during extrication and transportation could be catastrophic.3,4 Thus, the effectiveness of cervical immobilization has great clinical significance in the initial management of trauma patients.
Standard cervical immobilization typically includes the application of a firm cervical collar, rigid spine board, a device or means to prevent rotation of the head and straps for fixing the patient’s torso and extremities to the board. 5
The mostly used cervical immobilization device is the cervical collar. Several cervical collars have been used in adult trauma patients, and each one has variable degrees of immobilization of neck movement.6–8
XCollar (Emegear, Carpinteria, CA; Figure 1) has a cervical splinting system designed to splint the cervical spine by securing the head to the torso above the first cervical vertebrae and below the seventh cervical vertebrae, and this is known to decrease the risk of SCI by minimizing potential cervical spinal distraction. 9

The front view, back view and side view of the XCollar.
We compared XCollar with two other cervical collars commonly used for adult trauma patients. The purpose of this study was to evaluate the difference in effectiveness between the three cervical collars in their ability to restrict cervical range of motion (CROM).
Methods
Study design
We conducted a randomized study to evaluate the difference in effectiveness between the three cervical collars in their ability to restrict CROM. This study was performed at Daejeon Health Institute of Technology in February 2018.
This study was approved by the local ethics committee for human participants in February 2018 (Kangnam Sacred Heart Hospital Institutional Review Board; IRB No. 2017-12-023-001), and written informed consent was obtained from all the participants for their anonymized information to be published in this article.
The study is mainly designed and performed by researcher of Kangnam Sacred Heart Hospital. Daejeon Health Institute of Technology provided a place for the test of this study.
Participants
A total of 30 healthy volunteers from Daejeon Health Institute of Technology participated in this study, and their ages were between 21 and 25 years. Participants were excluded if they had any history of cervical vertebral disease, operation, trauma or cervical spine pain.
Equipment and material
In our study, the three cervical collars tested were: Philadelphia® Collar (Philadelphia Collar Company, Philadelphia, PA), Stifneck® Select™ Collars (Laerdal, Wappingers Falls, NY) and XCollar (Emegear).
A still image of cervical motion was taken with a digital camera (EOS 800D, Canon Inc, Ota, Tokyo, Japan). CROM was measured for each subject by analysing the still images using ImageJ, an image-analysis software (National Institute of Health, Bethesda, MD). 10
Interventions
A total of 30 participants were finally enrolled, and they were allocated into three groups: group A (n = 10), group B (n = 10) and group C (n = 10) in a random order generated by a sequence generator (www.random.org; Figure 2).
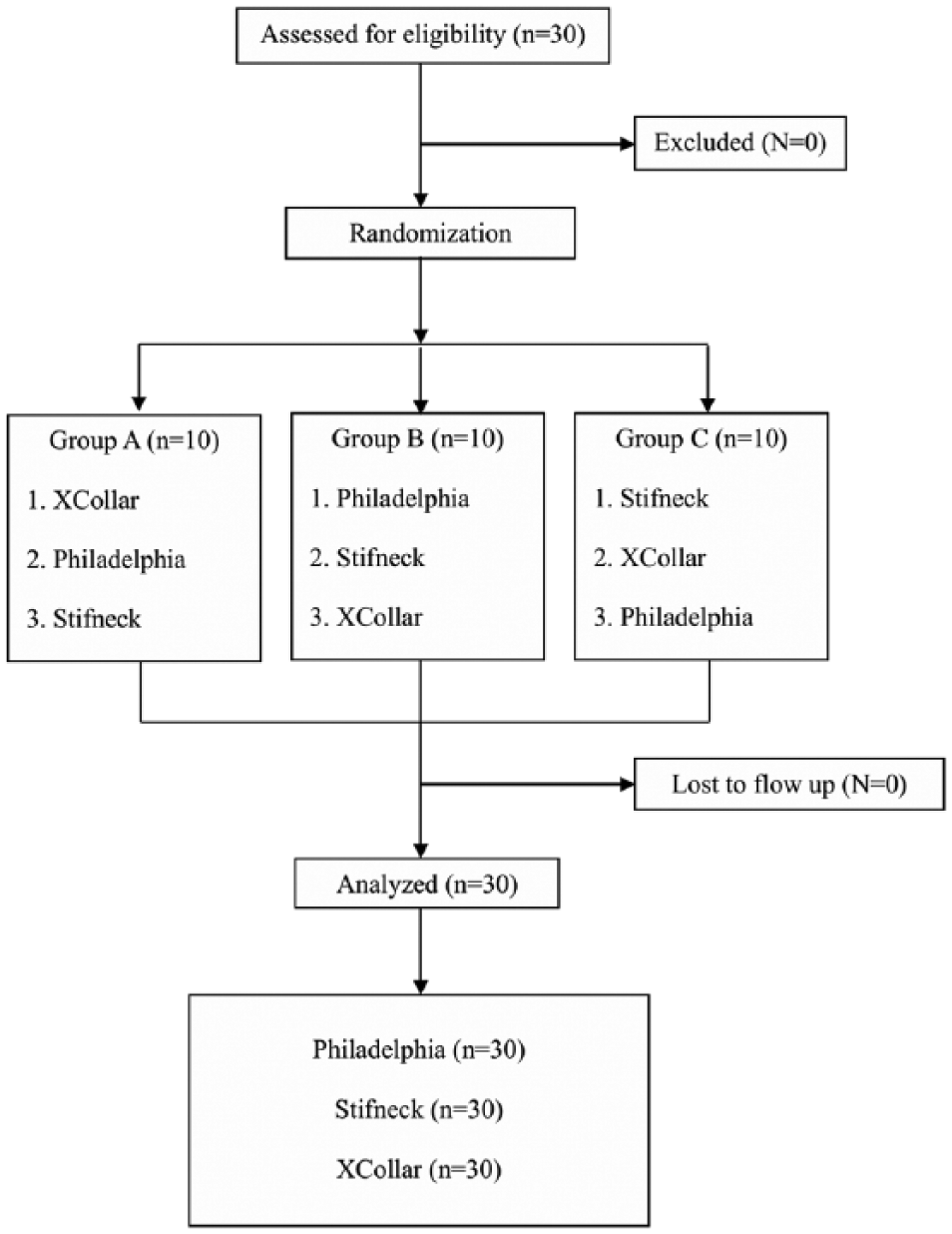
Flow diagram.
One of our investigators placed the three cervical collars consecutively on the participants, and each cervical collar was applied according to the manufacturer’s instructions. All sizes of the three cervical collars were available during the study.
We measured CROM in three planes (involving flexion/extension, bilateral bending, and bilateral axial rotation).6,11,12 Cervical range of flexion and extension were measured in the seated position, and cervical range of bilateral axial rotation was measured in the supine position.
The participants were asked to perform neck motion without moving their chest and shoulders by bringing their chin to their sternum, their occiput to their back during flexion-extension, their ear to their shoulder during lateral bending (bilaterally) and turning their nose during axial rotation (bilaterally).
CROM was measured first without a cervical collar in the unbraced condition, then, the same test was performed with the cervical collars. During the test, the participants were asked to perform neck movement to their maximal ability and hold still while images were taken for the measurement of CROM.
Cervical range of flexion and extension (sagittal plane) was measured by calculating the difference in the angle of the external occipital protuberance in the flexion or extension position compared to the neutral position using a lateral view picture of the participants in the sitting position.
Cervical range of bilateral bending (coronal plane) was measured by calculating the difference between two angles of the most superior point of the external ear in both the maximal lateral bending position and neutral position using the anterior and posterior view pictures of the participants in the sitting position.
Cervical range of bilateral axial rotation (transverse plane) was measured from a calculation of the difference between two angles of the nose indicator in both the maximal lateral bending position and neutral position using a vertex view picture of the participants in the supine position.
Data are expressed as the mean and standard deviation. Range of motion is reported in degrees.
Outcomes
The outcome was the restricted ranges of cervical motion between the three cervical collars.
Statistical analysis
The data were compiled using a standard spreadsheet application (Excel, Microsoft, Redmond, WA) and analysed using the Statistical Package for the Social Sciences (SPSS) 20.0 for Windows (SPSS Inc, Chicago, IL). We generated descriptive statistics and presented them as means with standard deviation (mean ± SD) for continuous data. To compare CROM among the three cervical collars, the repeated measures analysis of variance (ANOVA) and Friedman test were used for continuous variables. A post hoc analysis was conducted with the Wilcoxon signed-rank test or a paired t-test using the Bonferroni correction.
For all analysed data, P < 0.05 was considered statistically significant. In contrast, in the post hoc analysis, P < 0.017 was considered significant.
Results
A total of 30 participants (15 men; 15 women) completed the study. The baseline characteristics of the participants are shown in Table 1.
Baseline characteristics.
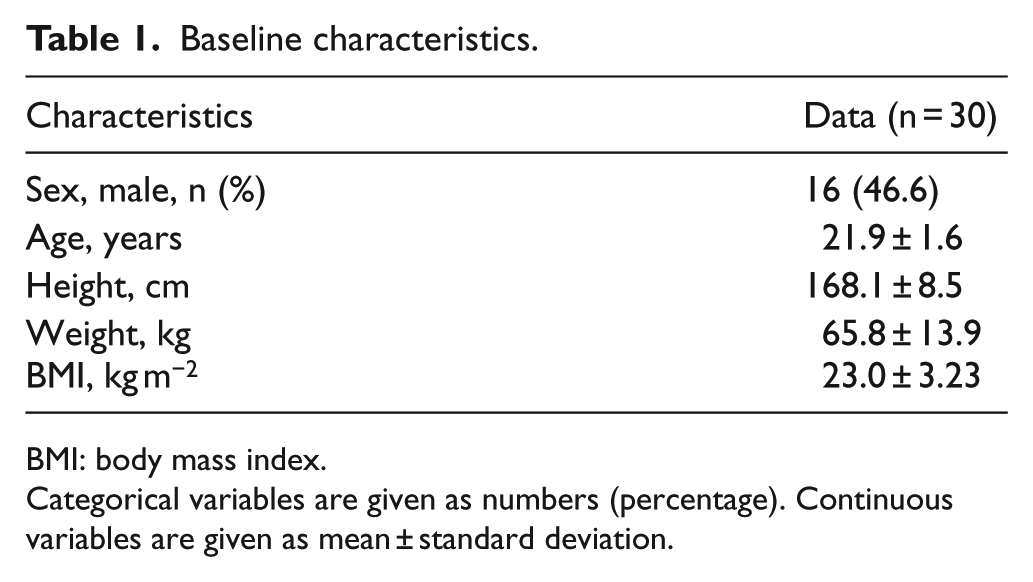
BMI: body mass index.
Categorical variables are given as numbers (percentage). Continuous variables are given as mean ± standard deviation.
The CROM obtained during flexion, extension, bilateral bending and bilateral axial rotation for each collar is presented in Table 2. The CROM measured in the collar-wearing condition was significantly different from that in the unbraced condition. The comparison of CROM between each neck collar also presented significant differences.
Mean range of cervical movement in the three planes in different collars.
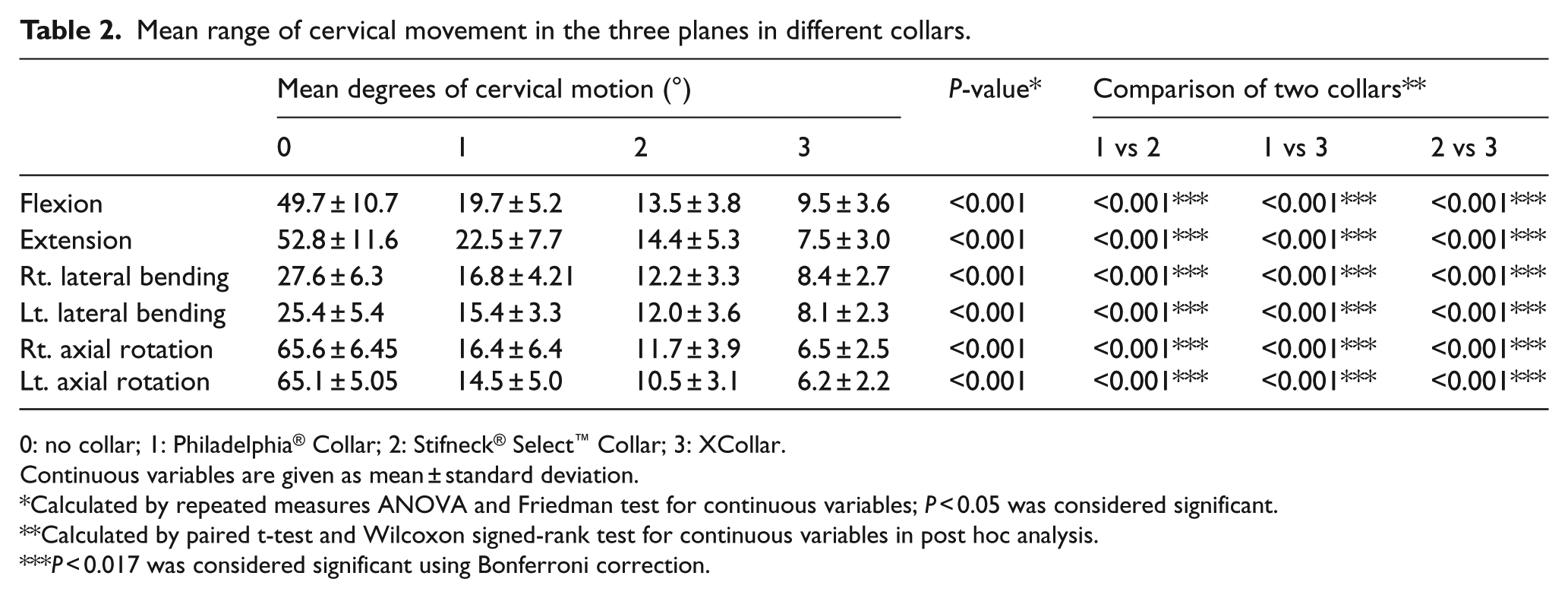
0: no collar; 1: Philadelphia® Collar; 2: Stifneck® Select™ Collar; 3: XCollar.
Continuous variables are given as mean ± standard deviation.
Calculated by repeated measures ANOVA and Friedman test for continuous variables; P < 0.05 was considered significant.
Calculated by paired t-test and Wilcoxon signed-rank test for continuous variables in post hoc analysis.
P < 0.017 was considered significant using Bonferroni correction.
On average, XCollar permitted less than a mean of 10° of movement during flexion, extension, bilateral bending and bilateral axial rotation. This was less than the movement permitted by the other two cervical collars (Table 2).
CROM was also collected as a mean percentage of cervical motion (Table 3), which was calculated as follows:
Mean percentage of cervical motion (%) = (°) braced ROM/(°) unbraced ROM × 100.
A comparison of percentage restriction to range of cervical movement by each collar in three planes.
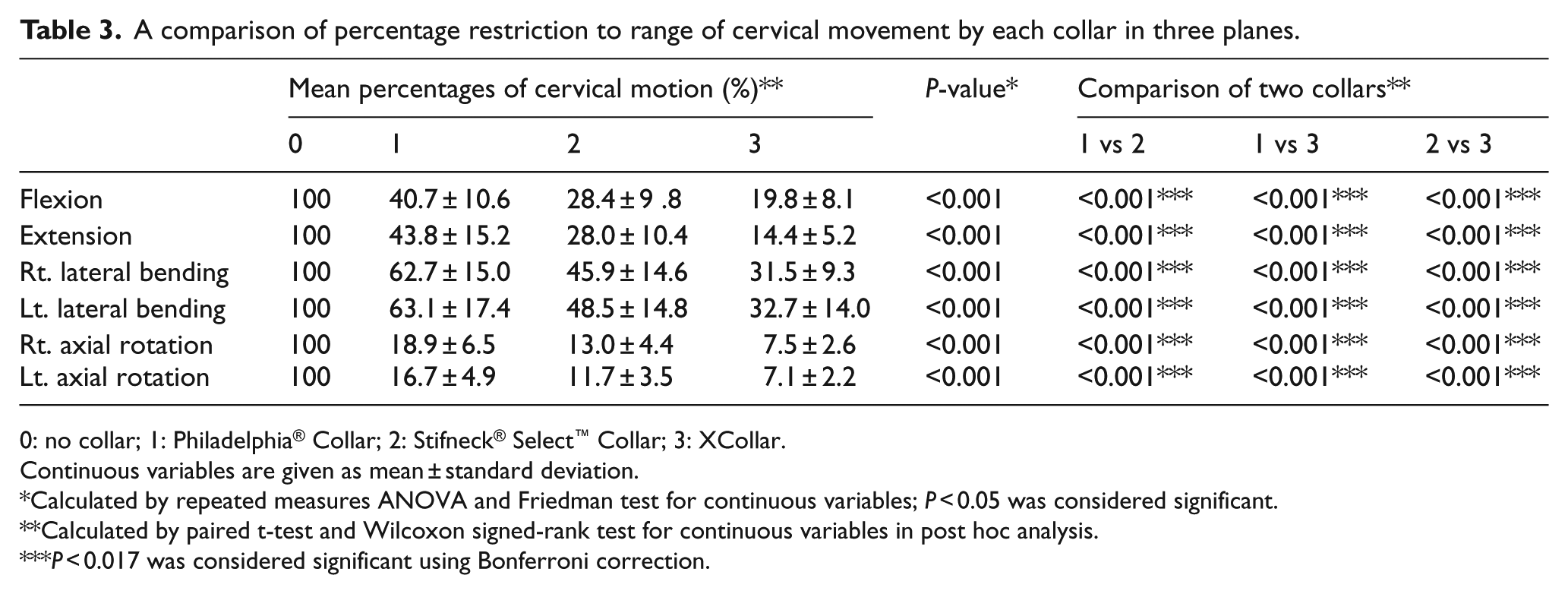
0: no collar; 1: Philadelphia® Collar; 2: Stifneck® Select™ Collar; 3: XCollar.
Continuous variables are given as mean ± standard deviation.
Calculated by repeated measures ANOVA and Friedman test for continuous variables; P < 0.05 was considered significant.
Calculated by paired t-test and Wilcoxon signed-rank test for continuous variables in post hoc analysis.
P < 0.017 was considered significant using Bonferroni correction.
All the neck collars showed the least restricted mean percentage of cervical motion in lateral bending (coronal plane), and the most restricted mean percentage of cervical motion in bilateral axial rotation (transverse plane).
Compared with the other two cervical collars, XCollar presented superior cervical restriction in the three planes and was particularly more effective in restricting axial rotation movements (Tables 2 and 3).
Discussion
The cervical collar has been used as a common device for the initial stabilization of the cervical spine. Although many cervical collars are commercially available, there is currently no consensus as to which offers the greatest protection, with studies showing considerable variations in their ability to restrict CROM.6–8,13 This study found that XCollar presented superior cervical restriction in the three planes and was particularly more effective in restricting axial rotation movements.
Although the three neck collars reduced CROM in this study, the amount by which the Philadelphia Collar and Stifneck Select Collar immobilized the cervical spine was clinically less substantial because although many routine daily tasks require only 30%–50% of full cervical spine movement, 14 these two cervical collars did not immobilize the neck sufficiently to prevent the movements. In contrast, XCollar presented superior immobilization of CROM compared to the other two cervical collars.
This may be due to the difference of support structure between the three neck collars. Philadelphia Collar uses a four-point support structure at the bottom of the collar: namely, at the two trapezius muscles posteriorly and at the two clavicles anteriorly; and Stifneck Select Collar uses the sternum as a fifth support structure. 15 Unlike these neck collars, XCollar has an additional stabilization structure which extends its superior edge to the zygomatic arches and external occipital protuberance, and its inferior margin sufficiently below the manubrium and upper thoracic spine. 16
As a result, we could speculate that the better immobilization of XCollar could be because it has a more supportive structure than the other two neck collars.
According to the Allen et al.’s 17 classification, distractive-flexion injuries are the most frequent cervical injuries. Therefore, it is very important to reduce external flexion forces that can cause additional injury to the cervical spine. In this study, XCollar presented the most restricted cervical range of neck movement during flexion than the other two neck collars (Tables 2 and 3). Hence, XCollar could be more effective in the prevention of cervical spine injury compared to the two other neck collars.
The rationale behind the superiority of XCollar over the other two cervical collars in restricting flexion is unclear. However, we speculate that it may be related to the chin support structure and adjustable chest support structure that secures the XCollar around the neck. 18
There were several limitations to this study.
First, we employed only healthy asymptomatic volunteers in the subject selection. Hence, the measured CROM could differ from that of patients with cervical spine injuries or neck pain symptoms. Second, the average age of the participants in this study was 21.9 ± 1.6 years; therefore, it could be a limitation if the results are to be applied to a younger or older population. Third, in most other studies involving cervical collars, radiographic techniques were used to measure the degrees of cervical motion, but our study used a digital camera and image-analysis software. Although we excluded the risk of radiation exposure for the participants using non-radiographic techniques, the true range of motion in the cervical spine was not identified. Finally, other factors besides CROM that make up the superiority of the cervical collar is not considered in this study. The superiority of the cervical collar could be different if other factors such as price, ease of wearing, patient’s comfort and durability of cervical collar are evaluated in this study.
In conclusion, these results suggest that when the use of a neck collar is considered for the prevention of additional cervical injury, XCollar might be one of the considerate options as a cervical immobilization device.
Supplemental Material
hkj809499 – Supplemental material for Comparison of the efficacy of three cervical collars in restricting cervical range of motion: A randomized study
Supplemental material, hkj809499 for Comparison of the efficacy of three cervical collars in restricting cervical range of motion: A randomized study by Jae Guk Kim, Sung Hwan Bang, Gu Hyun Kang, Yong Soo Jang, Wonhee Kim, Hyun Young Choi and Gyoung Mo Kim in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors would like to thank Daejeon Health Institute of Technology for offering place to perform this study and Editage (![]() ) for writing assistance. J.G.K. and S.H.B. contributed equally to this work. All authors contributed to the development of the study protocol. J.G.K. and S.H.B. were responsible for obtaining ethical approval for the study and cleaned all data in preparation for data analysis. G.M.K. collected all data. J.G.K., G.H.K., Y.S.J., W.K. and H.Y.C. undertook the data analysis. All authors contributed to preparation of the manuscript and all take responsibility for its contents.
) for writing assistance. J.G.K. and S.H.B. contributed equally to this work. All authors contributed to the development of the study protocol. J.G.K. and S.H.B. were responsible for obtaining ethical approval for the study and cleaned all data in preparation for data analysis. G.M.K. collected all data. J.G.K., G.H.K., Y.S.J., W.K. and H.Y.C. undertook the data analysis. All authors contributed to preparation of the manuscript and all take responsibility for its contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Primary data used in this research article were submitted with article submission.
Ethical approval
This study was approved by the local ethics committee for human participants in February 2018 (Kangnam Sacred Heart Hospital Institutional Review Board; IRB No. 2017-12-023-001).
Human rights
Written informed consent was obtained from the participant for photographs that may identify the patient.
Informed consent
Written informed consent was obtained from the all patients for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.