
Abstract
Objectives:
This prospective study was performed to evaluate the diagnostic accuracy of bedside point-of-care abdominal ultrasonography performed by emergency physician in patients with non-traumatic acute abdominal pain.
Methods:
The patients, who were admitted to emergency department due to abdominal pain, were included in this study. The emergency physician obtained a routine history, physical examination, blood draws, and ordered diagnostic imaging. After the initial clinical examinations, all the patients underwent ultrasonography for abdominal pathologies by emergency physician and radiologist, respectively. Point-of-care abdominal ultrasonography compared with abdominal ultrasonography performed by radiologist as the gold standard.
Results:
The study included 122 patients. Gallbladder and appendix pathologies were the most commonly detected in the abdominal ultrasonography. Compared with abdominal ultrasonography, point-of-care abdominal ultrasonography was found to have 89% sensitivity and 94% specificity in gallbladder pathologies; 91% sensitivity and 91% specificity in acute appendicitis; 79% sensitivity and 97% specificity in abdominal free fluid; 83% sensitivity and 96% specificity in ovarian pathologies. Compared to final diagnosis, preliminary diagnoses of emergency physicians were correct in 92 (75.4%) patients.
Conclusion:
This study showed that emergency physicians were successful in identifying abdominal organ pathologies with point-of-care abdominal ultrasonography after training.
Introduction
Acute abdominal pain (AAP) is a common complaint in the emergency department (ED). The origin of pain may be surgical or medical, and it may range from benign, self-limiting conditions to diseases of high mortality. Therefore, correct diagnosis and treatment are important. The emergency physician (EP) should have sufficient assessment skills to triage such patients. Patient history, physical examination, and laboratory tests are the primary steps, but they are not always reliable or specific enough to pinpoint an exact diagnosis.1,2
Computed tomography (CT) scan, which is considered as diagnostic gold standard in diagnosis of the most abdominal pathologies, is an expensive and time-consuming modality that uses ionizing radiation. 3 Ultrasonography (US), on the other hand, is noninvasive, cheap, requires neither the injection of a contrast medium nor radiation, and can be employed quickly as a bedside examination tool.1–3 In most countries, US examinations are performed in radiology departments by specialist radiologists. The resources of the radiology departments are often limited, leading to long waiting times in the ED. 4
Point-of-care ultrasonography (POCUS), which is performed by clinicians at the bedside, is increasingly being used to facilitate accurate diagnoses, to monitor the fluid status, and to guide procedures in emergency and critical care.5–7 The use of bedside US performed by the EP is quite common in continental Europe and the United States. Several studies confirmed the benefits of an early bedside US examination in trauma situations. In addition, bedside US has been shown to reduce the length of stay in the ED, as well as the time to diagnosis and definitive care. 4
Studies evaluating diagnostic accuracy and other benefits of EP-performed US for patients with abdominal pain are fewer, but do exist.2,3 These studies mostly investigate single organ pathologies such as acute appendicitis, acute cholecystitis, and hydronephroses.8–10 However, all the causes should be considered and assessed during physical examination in the differential diagnosis of patients with abdominal pain. For accurate diagnosis, all abdominal tissues should be systematically evaluated in the United States.
This prospective study was performed to evaluate the diagnostic accuracy of bedside point-of-care abdominal ultrasonography (POCAS) performed by EP in patients with non-traumatic AAP in comparison with abdominal ultrasonography (AUS) performed by radiologist as the gold standard.
Methods
Study design
This study was initiated in the ED of a tertiary hospital following ethics committee approval. Both theoretical and practical trainings on AUS were provided to EPs by radiology clinic instructors. These trainings were given on weekly training day of ED for a total of 8 h for three consecutive weeks.
The theoretical training taught about natural structures of the liver, spleen, bile ducts, pancreas, intestine, abdominal aorta, kidney, and pelvic organs (appendix, bladder, ovary, uterus, and adnexa). The training was covered to detect the abdominal free fluid and diagnosing acute appendicitis, abdominal aortic aneurysm, cholelithiasis, acute cholecystitis, renal stones, hydronephrosis, intestinal obstruction, intrauterine–extrauterine pregnancy, and ovarian cyst. Six EPs participated in the study as a researcher who had a 6-month experience of work and extended focused assessment with sonography for trauma (E-FAST). Practical training was done on healthy adults and patients. First, practical training was given on natural structures of abdominal organs and imaging techniques on healthy adults.). Second, the comparative US practice with the radiology reports was made by the EPs participating in the study to at least 10 patients within 1-month period.
Setting and population
The patients of this study were collected in a one-year period between May 2017 and May 2018. The patients, who were admitted to ED due to AAP, had abdominal pathology identified in physical examination, had stable vital signs, and underwent AUS, were included in this study. The exclusion criteria were as follows: patients who were performed AUS and abdominal CT (ACT) scans in other centers and referred to ED of our hospital, patients who did not undergo AUS due to clinical instability and patients who were under 18 years of age. Written consent was obtained from all patients and their relatives who participated in the study.
Study protocol
The EP obtained a routine history, physical exam, laboratory tests, and ordered diagnostic imaging. After the initial clinical examinations, all the patients underwent US for abdominal pathologies by EP and radiologist, respectively.
POCAS was performed by an EP. A standard ultrasound (Mindray DC-T6, Germany) with two probes, including a 7.5-MHz linear probe and a 3.5-MHz convex probe, was used for POCAS. Afterward, AUS was performed by a radiologist. For AUS, 7.5-MHz linear and 3.5-MHz convex probe of the standard ultrasound device (TOSHIBA/Xario-Japanese) was used. AUS findings were recorded on the hospital automation system as the official US report.
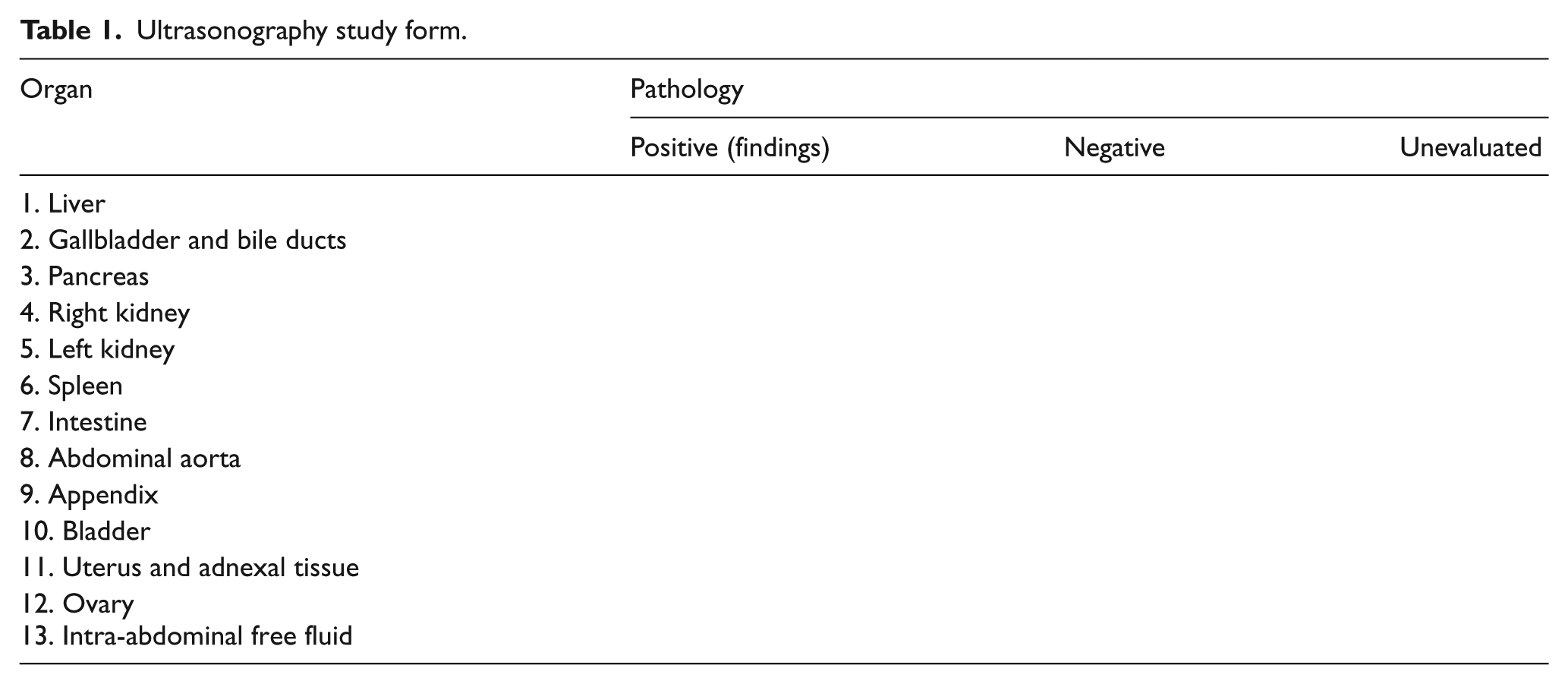
A standard form was created for the study. The vital signs and physical examination findings of the patients were recorded in this form. Pathologic findings, which were visualized by ultrasound, were recorded in this form (Table 1). The abdominal organs were noted as “unevaluated” when cannot be visualized. All organs were evaluated in order.
Ultrasonography study form.
POCAS scanning was performed in 10 steps:
Step 1. Liver; convex probe was used. The probe was placed in a sagittal orientation in the right anterior axillary line and swept horizontally from right to left until the far edge of the left lobe is visualized. Enlargement, mass, and abscess were assessed.
Step 2. Gallbladder and bile ducts; convex probe was used. Probe was placed under right costal margin in mid-clavicular line. Acute cholecystitis was diagnosed when US displayed cholelithiasis, gallbladder wall thickening, pericholecystic fluid, and a sonographic Murphy’s sign.
Step 3. Pancreas; convex probe was used. Acute pancreatitis was diagnosed when abdominal US revealed a swollen pancreas, fluid collection, and inflammation of adjacent organs.
Step 4.: Right and left kidney; convex probe was used; probe was placed in the left and right midaxillary region along the lower costal margin. Hydronephrosis was diagnosed, if there was enlargement of the black area at the center of the normally echogenic kidney; thinning of the renal parenchyma and dilatation of the calyces.
Step 5. Spleen; convex probe was used. Enlargement was assessed. The probe was placed in a sagittal orientation in the left anterior axillary line. Splenomegaly was accepted if the cranio-caudal length is more than 11 cm.
Step 6. Abdominal aorta; convex probe was used. Aorta was displayed in the midline, from the subxiphoid area to the umbilicus. Abdominal aortic aneurysm was accepted if the diameter of abdominal aorta more than 3 cm in transverse section.
Step 7. Intestine; convex probe was used. Fluid-filled bowel loops with thickened bowel walls, intestinal dilatation, and minimal peristalsis were accepted as ileus.
Step 8. Appendix; linear probe was used. The probe was placed in the Mc Burney’s point. A blind-ended tubular structure from the base of the cecum was identified as the appendix. This structure was accepted to be acute appendicitis when structure was non-compressible and aperistaltic with a diameter greater than 6 mm.
Step 9. Bladder, ovary, uterus, and adnexa; convex probe was used. Probe was placed in the suprapubic area. Ovarian cyst, intrauterine–extrauterine pregnancy, hydrosalpinx, and urinary retention were assessed. Free fluid in the pelvis with or without an ovarian cyst was accepted as ruptured ovarian cyst.
Step 10. Abdominal free fluid; convex probe was used. Free fluid was assessed similar to FAST exam. The anechoic area with sharp edges was accepted as free fluid.
ACT scans with intravenous contrast were performed patients who have not diagnosed after AUS. The CT scans were performed using HITACHI-ECLOS multi-slice 16-slice tomography device that was located in the Emergency Tomography Unit of ED. The diagnosis of patients was determined according to ACT and AUS results. Patients who were not hospitalized were discharged from the ED after an average of 8-h follow-up.
Statistical analysis
SPSS 21 software was used for the statistical analysis. Demographic data were reported as frequencies and medians with interquartile ranges for ordered non-normally distributed data and means with standard deviations for continuous normal data. Organs that were noted “unevaluated” in the AUS/POCAS examination were excluded from the statistical analysis. POCAS results were compared with AUS results and the specificity, sensitivity, and area values of POCAS were determined. Data were reported as percentages with a 95% confidence interval (CI).
Results
The study included 122 patients. The mean age of the patients was found to be 42 ± 17 years. Of all patients, 79 (65%) were female and 43 (%35) were male. The abdominal pain location in patients was as follows: entire abdomen in 19 (15.6%) patients, right upper quadrant in 23 (18.9%) patients, right lower quadrant 57 (46.7%) patients, epigastric area in 11 (9%) patients, left upper quadrant in 4 (3.3%) patients, left lower quadrant in 1 (0.8%) patients, and suprapubic region in 7 (5.7%) patients.
In the AUS, abdominal aorta and pancreatic pathologies were not detected. Gallbladder and appendix pathologies were the most commonly detected in the AUS. Gallbladder pathologies were detected in 27 (22%) patients. Cholelithiasis was imaged in 11 (9%) patients. Three patients who have a calculous cholecystitis were not diagnosed with POCAS. Six patients who have gallbladder polyps were interpreted as gallstones in the POCAS examination. Compared with AUS, POCAS was found to have 89% sensitivity and 94% specificity, (AUC: 0.913, 95% CI: 0.838–0.987) in gallbladder pathologies (Table 3, Figure 1).
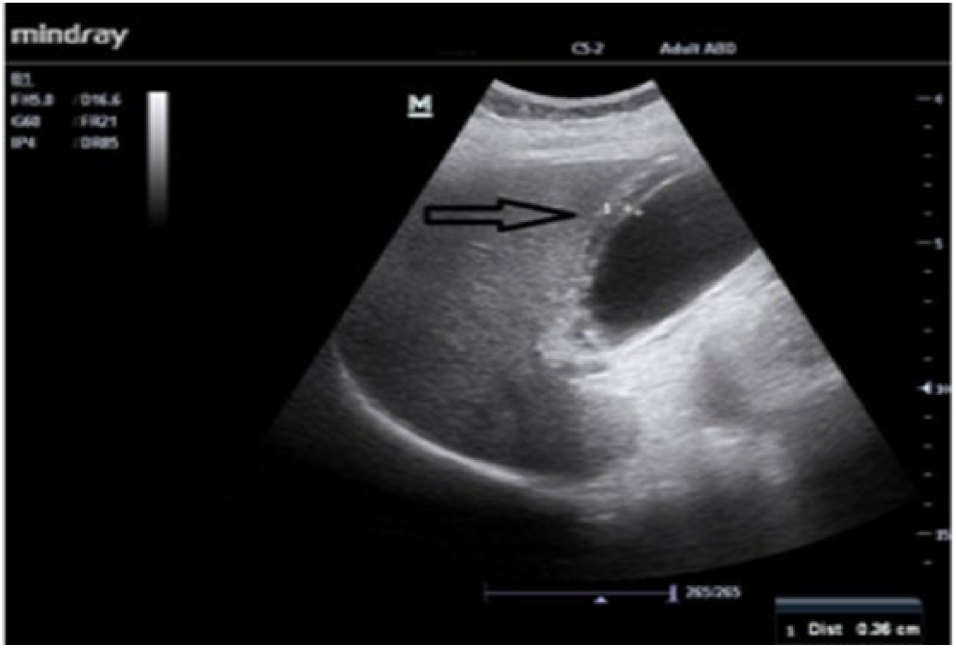
A 79-year-old female patient was admitted to the emergency department with a complaint of abdominal pain. Physical examination of the patient had right upper quadrant abdominal tenderness. The gallbladder was visualized with POCAS. The patient was hospitalized to the general surgery department with the diagnosis of acute cholecystitis.
A total of 27 patients were diagnosed acute appendicitis in the AUS. Three patients who were unevaluated with AUS were diagnosed acute appendicitis after ACT scans. Compared with AUS, POCAS was found to have 91% sensitivity and 91% specificity (AUC: 0.914, 95% CI: 0.839–0.988) in acute appendicitis (Table 3, Figure 2).
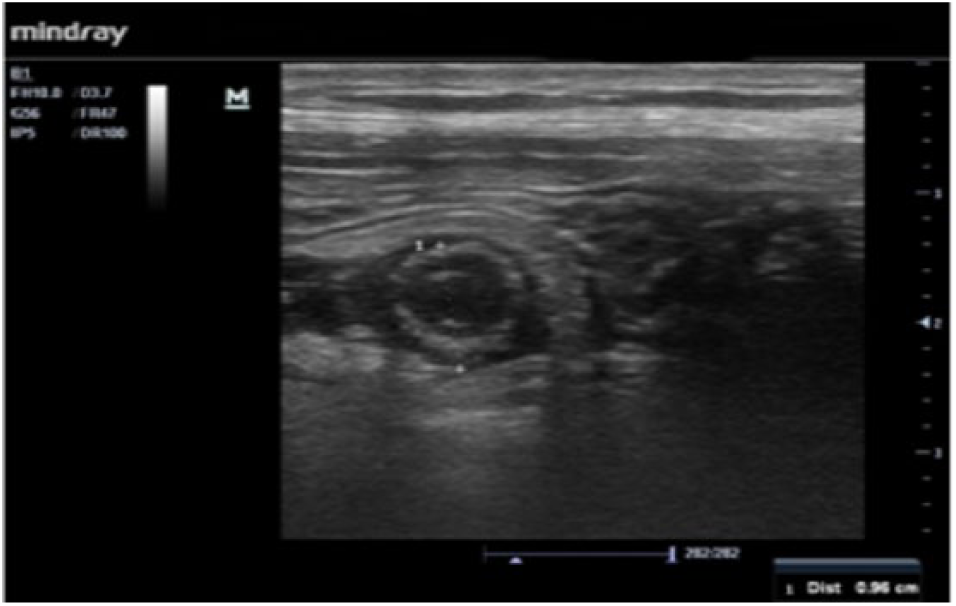
A 22-year-old male patient was admitted to the emergency department with abdominal pain complaint. Physical examination of the patient revealed evident tenderness in the right lower quadrant of abdomen. The appendix was visualized with POCAS. The patient was hospitalized to the general surgery department with the diagnosis of acute appendicitis.
Abdominal free fluid was detected in 19 (15.5%) patients with AUS (Table 2). Abdominal free fluid was diffused in six (5%) patients. Diffuse free fluid was displayed with POCAS. The patients who have diffuse free fluid were diagnosed as ovarian cyst rupture, acute appendicitis, bladder rupture, acute cholecystitis, acute mesenteric artery embolism (Figure 3), and gastric cancer. Compared with AUS, POCAS was found to have 79% sensitivity and 97% specificity (AUC: 0.880, 95% CI: 0.769–0.991) in free fluid (Table 3).
Ultrasonography results of emergency physician and radiologist.
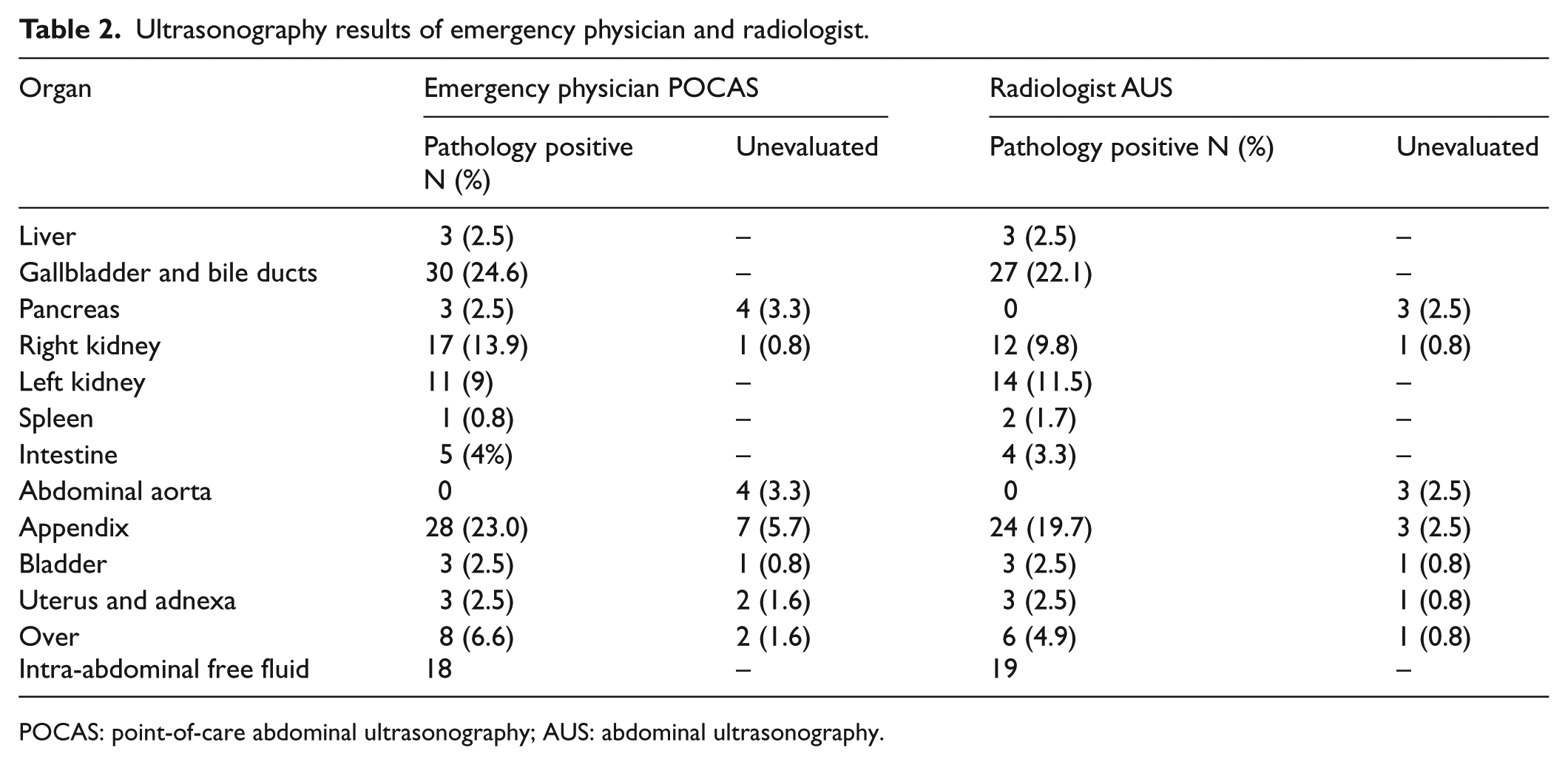
POCAS: point-of-care abdominal ultrasonography; AUS: abdominal ultrasonography.
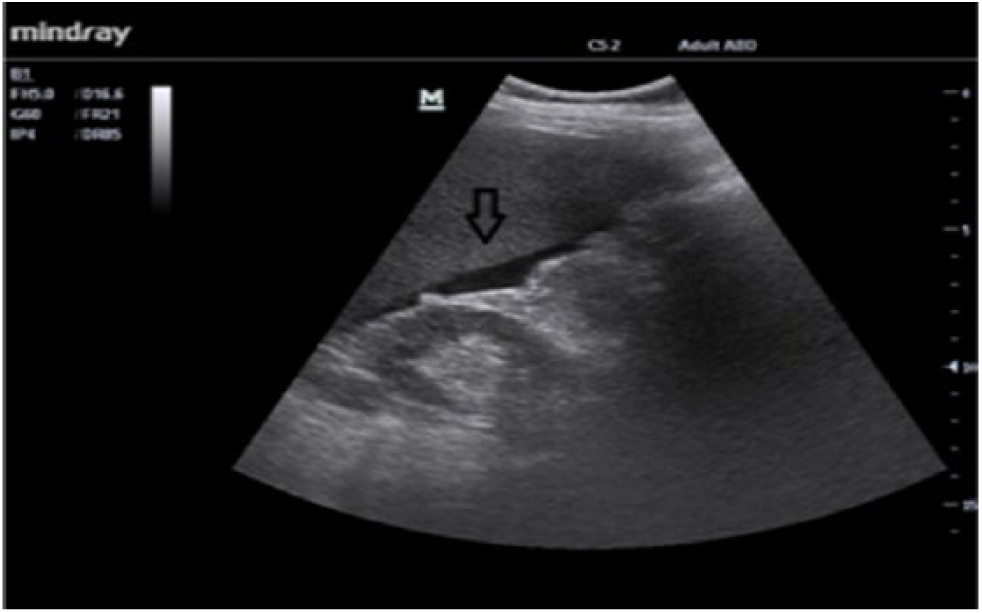
A 62-year-old female patient was admitted to the emergency department with a complaint of abdominal pain. Physical examination of the patient had general abdominal tenderness. Intra-abdominal free fluid was visualized with POCAS. The patient underwent computed tomography angiography imaging. The patient was hospitalized to the general surgery department with a massive mesenteric artery embolism diagnosis.
Emergency physician’s ability to identify organ pathologies with POCAS.
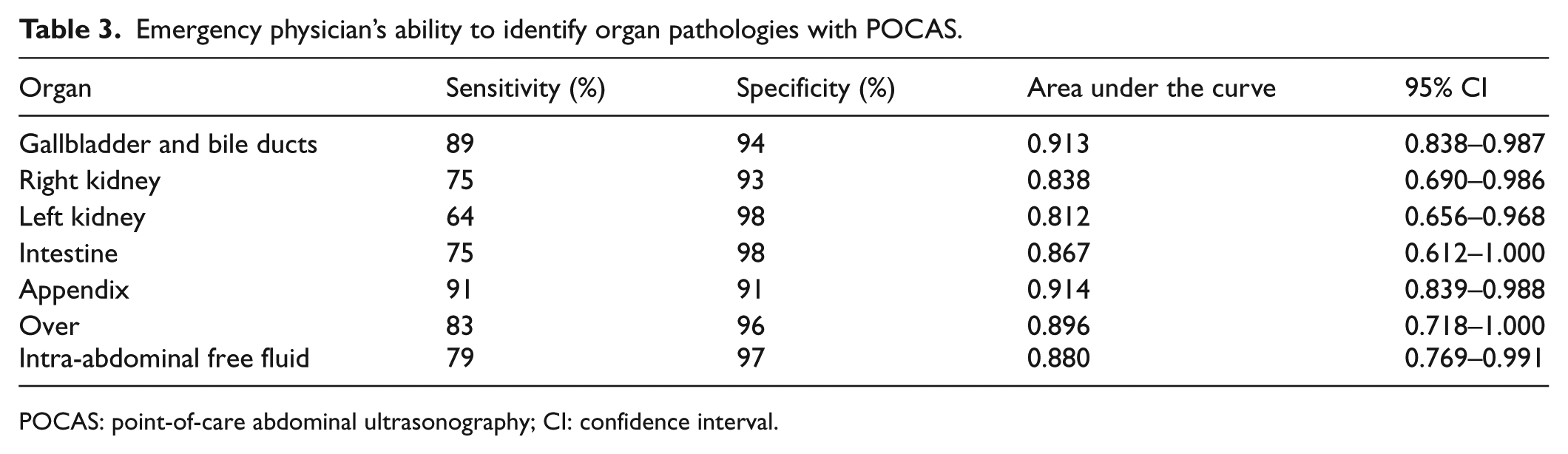
POCAS: point-of-care abdominal ultrasonography; CI: confidence interval.
Intestinal pathology was defined as ileus in two patients and as terminal ileitis in two patients in the AUS. In POCAS, intestinal pathology was correctly interpreted in three patients and was misinterpreted in two patients.
Ovarian pathology was detected in six patients in the AUS. Compared to AUS, POCAS was found to have 83% sensitivity and 96% specificity (AUC: 0.896, 95% CI: 0.718–1.000) in ovarian pathologies. Intrauterine pregnancy was imaged in two patients, and hydrosalpinx was detected in one patient.
ACT scan was performed in 34 (27.9%) patients. The patients were diagnosed finally according to results of AUS and/or ACT records.
A total of 69 (58%) patients were discharged from the ED. Diagnosis of the discharged patients was as follows: normal in 42 (61%) patients, mass in the liver in 2 (3%) patient, gallstones and/or sludge in 13 (19%) patients, renal colic in 7 (10%) patient, gastric cancer in 2 (3%) patient, and ovarian cyst in 3 (6%) patients.
A total of 53 (42%) patients were hospitalized. Diagnosis of the hospitalized patients was as follows: acute cholecystitis in 11 (21%) patients, acute pancreatitis in 1 (2%) patient, nephrolithiasis in 3 (6%) patients, acute mesenteric artery embolism in 1 (2%) patient, terminal ileitis in 2 (4%) patients, acute appendicitis in 30 (59%) patients, pelvic inflammatory disease in 1 (2%) patient (Figure 4), bladder perforation in 1 (2%) patient, and ruptured ovarian cyst in 2 (4%) patients.

A 31-year-old female patient was admitted to the emergency department with a complaint of abdominal pain. Physical examination of the patient had extensive tenderness in the pelvic region. The fallopian tubes and uterine pathology were visualized with POCAS. The patient was hospitalized to the gynecology department with the diagnosis of pelvic inflammatory disease.
Compared to final diagnosis, preliminary diagnoses of EPs were correct in 92 (75.4%) patients and were not correct in 17 (13.9%) patients. EPs did not determine the preliminary diagnosis in 13 (10.7%) patients.
Discussion
In crowded EDs, resources and time are limited. Therefore, the management of the patients should be planned correctly. US imaging has been used in areas where diagnostic imaging is limited, such as ED and critical care. In the last decade, EPs have used point-of-care ultrasound in many different medical situations. Many studies have shown that bedside ultrasound imaging is successful abdominal organs pathologies within adults and children.11–14 A study that investigated the role of US performed by EPs in detecting the various causes of AAP found a 76% rate of accurate diagnosis. 3 In another study in patients with nonspecific abdominal pain, the accurate diagnosis of EPs was found a 45%. 12 In our study, EPs who performed POCAS were calculated 75.4% rate of diagnostic accuracy. This result is consistent with literature.
Positive Murphy’s sign (point of maximal tenderness to transducer pressure when localized to the sonographically visualized gallbladder fundus) in combination with the presence of gallstones makes the diagnosis of acute cholecystitis. 15 The high success rate in the diagnosis of gallbladder pathologies was most likely due to easily identifiable sonographic Murphy’s sign in imaging. In a study, in patients suspected to cholecystitis, the sensitivity and specificity of bedside US that performed by EPs in determining acute cholecystitis were 87% and 82%, respectively. 16 In another study, the sensitivity and specificity of bedside US were 89.58% and 96.59%, respectively. 10 In our study, the most common cause of acute abdomen was due to gallbladder pathology. The sensitivity and specificity of POCAS for detecting gallbladder pathology were calculated as 89% and 94%, respectively. The success rate of our study was consistent with the literature.
Acute appendicitis was easily diagnosed in patients presenting with classic symptoms. However, diagnosis may be delayed in patients with nonspecific symptoms, especially in children, elderly, and female patients.11,17 In a study, bedside ultrasound performed by EPs had a sensitivity of 44.18%, specificity of 85.18% and overall accuracy of 67.01% in diagnosing appendicitis in patients clinically suspicious to have acute appendicitis. 18 In another study, in patients suspected to acute appendicitis, bedside US was found to have 72.97% sensitivity, 83.10% specificity, in determining acute appendicitis. 18 In our study, compared to AUS, POCAS was found to have 91% sensitivity and 91% specificity in acute appendicitis. In our study, the sensitivity and specificity rates were higher than the other studies. This success of EPs may depend on their ability to manage the patients by themselves and interpretation of ultrasound images with physical examination findings. In addition, in this study, the long-term and detail training of researchers might have increased the correct diagnosis rate.
Differential diagnosis of right lower quadrant pain includes acute appendicitis, gastroenteritis, ileitis, ovarian cyst or cyst rupture, mass, or ovarian torsion, pelvic inflammatory disease, and ectopic pregnancy.11,17 Usually clinical history and physical examination are insufficient in the diagnosis of pelvic or lower quadrant pain in female patients. These patients usually have high morbidity and mortality rates, especially due to ectopic pregnancy. Transvaginal US is considered to be more superior to AUS in the evaluation of uterine and adnexal structures. However, in practice, the use of transvaginal US may be limited in the ED environment. For this reason, the use of AUS in evaluating uterus and adnexal has become more common.15,19 In meta-analysis, bedside pelvic US performed by EPs was found 99.3% sensitivity and 99.96% negative predictive value in the diagnosis ectopic pregnancy. 20 In our study, ovarian pathology was detected in six patients in the AUS. Compared to AUS, POCAS was found to have 83% sensitivity and 96% specificity in ovarian pathologies. In addition, intrauterine pregnancy was imaged in two patients, and hydrosalpinx was detected in one patient in the POCAS and AUS.
Renal US is helpful in the management of acute kidney injury, nephrolithiasis, and urinary tract infection. 7 A recent study evaluated bedside renal ultrasound performed by EPs reported a 76.3% sensitivity to detect hydronephrosis and a 90% sensitivity for large stones (>5 mm). 21 In another study, the sensitivity and specificity of EP in the diagnosis of hydronephrosis were found 90.8% and 78.3%, respectively. 9 In a study on patients with nephrolithiasis, there is no difference in complications, pain, return visits, admissions, or diagnostic accuracy between patients with suspected nephrolithiasis when evaluated with POCUS, radiology US, or CT. 22 In our study, the sensitivity and specificity of POCAS for detecting right and left kidney pathology were calculated as 75%–93% and 64%–98%, respectively. In addition, in one patient, rupture of the bladder and extensive intra-abdominal free fluid were detected in the POCAS and AUS.
FAST is a modality to rapidly detect free fluid (usually blood) in the peritoneal, pericardial, or pleural spaces in trauma patients. Studies were indicated that trained ED residents like their fellow radiology residents have the ability to perform FAST scan with high diagnostic value in patients with trauma.23,24 In these studies, the sensitivity and specificity of EPs in the diagnosis of abdominal free fluid were reported as 80%–90% and 95%–98.5%, respectively.23 –25 Spontaneous hemoperitoneum frequently presents with AAP with or without hemodynamic collapse. The etiology of spontaneous hemoperitoneum may be varied, and its causes may be classified as gynecologic, hepatic, splenic, vascular, or coagulopathic diseases. In some patients, the collapse becomes obvious after the initial evaluation; therefore, spontaneous hemoperitoneum should be detected rapidly during the evaluation. 7 In addition, the presence of free fluid may be a sign of pathology in a nearby organ such as acute appendicitis, ovarian cyst rupture, and acute cholecystitis. In our study, abdominal free fluid was detected in 15.5% patients with AUS. Compared with AUS, POCAS was found to have 79% sensitivity and 97% specificity in abdominal free fluid. The success rate of our study was consistent with the literature. In addition, free fluid was diffused in six patients. The patients who have diffuse abdominal free fluid were diagnosed ovarian cyst rupture, acute appendicitis, bladder rupture, acute cholecystitis, acute mesenteric artery embolism, and gastric cancer.
Limitations
In our study, hepatic, splenic, and intestinal pathologies were rarely detected. In addition, aortic pathology was no imaged in our study. In our study, theoretical and practical training does not include Doppler US. Furthermore, abdominal organs were not evaluated for acute infarction and ischemia.
Conclusion
US is an important bedside tool in ED. However, the accuracy of the US assessment is mostly operator-dependent. This study showed that EPs were successful in identifying abdominal organ pathologies with POCAS after training. Success rates can be increased with long-term US training programs.
Footnotes
Acknowledgements
N.K., B.E., C.K., and O.F.K. contributed to study concept and design. O.F.K., G.T., C.K., and B.E. contributed to acquisition of the data. N.K., M.A., O.F.K., and C.K. contributed to analysis and interpretation of the data. N.K., M.A., E.A., and G.T. contributed to drafting of the manuscript. N.K., M.A., and E.A. contributed to critical revision of the manuscript for important intellectual content. N.K. and B.E. contributed to statistical expertise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All materials taken from other sources (including our own published writing) were clearly cited.
Ethical approval
This study was initiated in the ED of a tertiary hospital following ethics committee approval.
Informed consent
Written consent was obtained from all patients who participated in the study and their relatives.
Human rights
Our work does not infringe on any rights of others, including privacy rights, and intellectual property rights. There is no human rights violation in our manuscript.