
Abstract
Background:
Acute appendicitis is a very common surgical emergency. Early and correct diagnosis and early intervention are necessary to prevent complications. It is often diagnosed on clinical signs and a certain ratio of negative appendectomy is acceptable. For early and accurate diagnosis, various scoring systems such as Alvarado, Ohmann, Eskelinen and more recently Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) have been developed.
Objective:
In this study, we aimed to compare the effectiveness and accuracy of scoring systems.
Materials and methods:
The patients who attended emergency department and operated with acute appendicitis pre-diagnosis were evaluated retrospectively. Alvarado, Ohmann, Eskelinen, and RIPASA scores were calculated and compared with histopathologic results by reviewing the patient files.
Results:
A total of 76 patients (44 males and 32 females) were included in the study. The mean age was 33.8 ± 13.2 years. Of which, 59 patients (77.6%) were diagnosed to have acute appendicitis on histopathological examination. The mean leukocyte count was 13.9 ± 3.7 × 103 μL. Sensitivity and specificity of Alvarado, Ohmann, Eskelinen, and RIPASA were 36%–82%; 58%–71%; 36%–8%, and 68%–71%, respectively. Cut-off values were 8, 14, 55.63, and 10, respectively. RIPASA had the highest accuracy. The cut-off value of leukocyte counts was 13,900 × 103/μL. Sensitivity and specificity were 64% and 88%, respectively; positive predictive value was 95%. In the receiver operating curve analysis, the area under the curve was found to be 74%.
Conclusion:
The RIPASA scoring system is a more reliable scoring system than Ohmann, Eskelinen, and Alvarado scoring systems. In cases of suspected acute appendicitis, it may be useful to evaluate patients with RIPASA score in emergency departments by general practitioners, where there is no general surgeon. Thus, patients can be guided in a timely manner to reduce the complications that may arise from delays. The cut-off value of 13,900 × 103/μL is an important marker for the presence of acute appendicitis.
Introduction
Acute appendicitis is a common surgical emergency. Early intervention in cases with acute appendicitis prevents complications such as perforation, abscess, and peritonitis. For this reason, cases of acute appendicitis should be operated before the development of the complications. 1
Various scoring systems have been developed and put into practice for the diagnosis of acute appendicitis. Alvarado, Ohmann, Eskelinen, and Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) are the most widely known scoring systems.2–6 These scoring systems are formed by a combination of examination findings and laboratory results. Each scoring system has been presented with the thought that it may be useful in diagnosing acute appendicitis. The main goal is to minimize negative appendectomy, to facilitate diagnosis, and to accelerate the process. In this process, standardizing different complaints in male and female patients in different societies will increase the success of the scoring system. There is no consensus on which one of the scoring systems has a higher rate of true diagnosis.
In this study, it has been aimed to determine which one of Alvarado, Ohmann, Eskelinen, and RIPASA scoring systems is more effective in diagnosing acute appendicitis.
Materials and methods
The patients who were included in the study were the ones who attended emergency department with abdominal pain and a surgery was performed because the surgeons considered them suffering from acute appendicitis. Informed consent of all patients and retrospective study approval from the hospital were taken. Scoring results were obtained by retrospectively evaluating the patient’s data. Female patients were gynecologically consulted for gynecological pathology. Patients with hematuria were consulted with urology. Pregnant patients were not included in the study. The forms of Alvarado, Ohmann, Eskelinen, and RIPASA scoring systems were filled and scores were determined and evaluated with the results of postoperative histopathologic examination.
Descriptive statistics were calculated for continuous variables (mean, standard deviation, minimum, maximum, and median). The diagnostic performance of parameters was assessed by receiver operating curve (ROC) analysis. The reliability between two categorical variables was performed by Kappa test. Statistical analysis was performed using the MedCalc Statistical Software version 12.7.7 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org, 2013).
Results
A total of 76 patients with pre-diagnosis of acute appendicitis were included in the study. Of which, 44 of the patients were males and 32 were females. The mean age was 33.8 ± 13.2 (range = 15–72) years. Out of the 76 patients, 59 patients (77.6%) were diagnosed with acute appendicitis histopathologically, and 17 patients had negative appendectomy (22.36%). The mean leukocyte values were 13911.5 ± 3721.5 × 103/μL. Patient scores and histopathology results were evaluated by comparison (Table 1).
Comparison of scores of scoring systems with histopathological results.
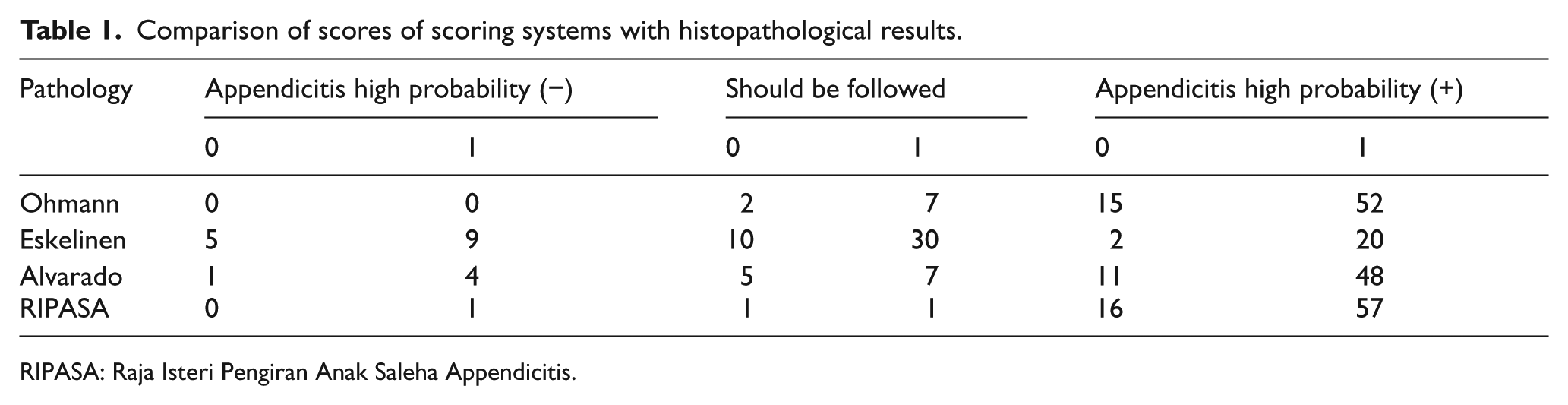
RIPASA: Raja Isteri Pengiran Anak Saleha Appendicitis.
Upon evaluation, the sensitivity of Alvarado, Ohmann, Eskelinen, and RIPASA was 36%, 58%, 36%, and 68%, respectively, and the specificity of Alvarado, Ohmann, Eskelinen, and RIPASA was 82%, 71%, 88%, and 71%, respectively. Cut-off values were found to be 8, 14, 55.63, and 10 for Alvarado, Ohmann, Eskelinen, and RIPASA, respectively. The highest scoring system was found to be RIPASA with 75% diagnostic accuracy (Table 2). The ROC curves of the scoring systems are shown in Figure 1.
ROC analysis for scoring systems.
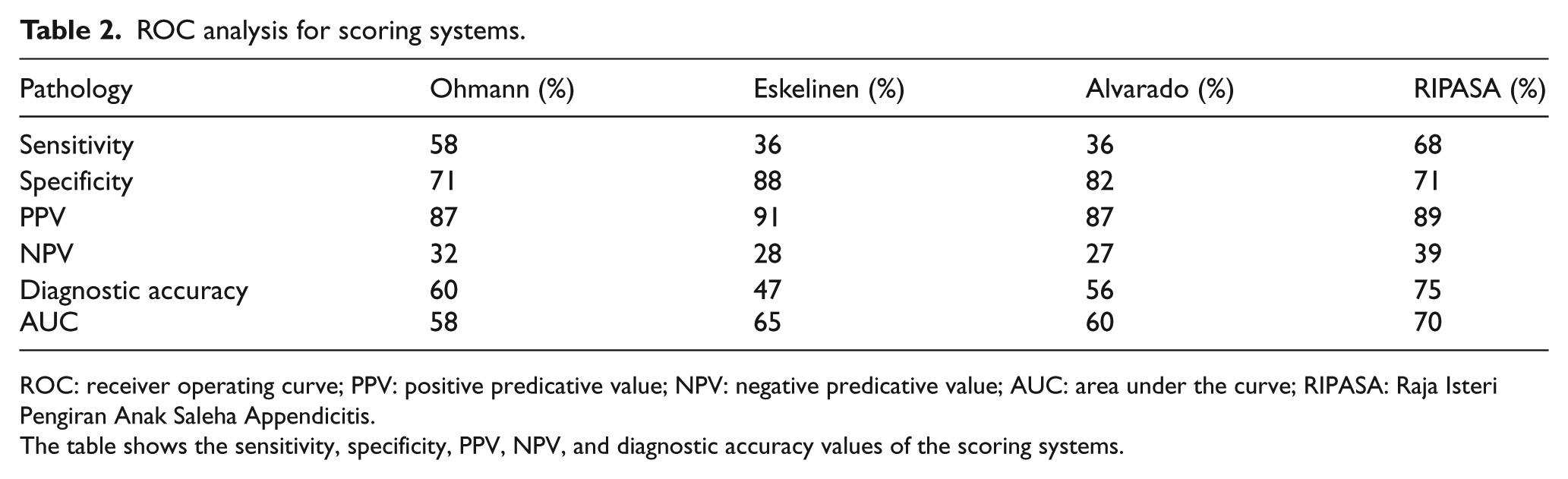
ROC: receiver operating curve; PPV: positive predicative value; NPV: negative predicative value; AUC: area under the curve; RIPASA: Raja Isteri Pengiran Anak Saleha Appendicitis.
The table shows the sensitivity, specificity, PPV, NPV, and diagnostic accuracy values of the scoring systems.
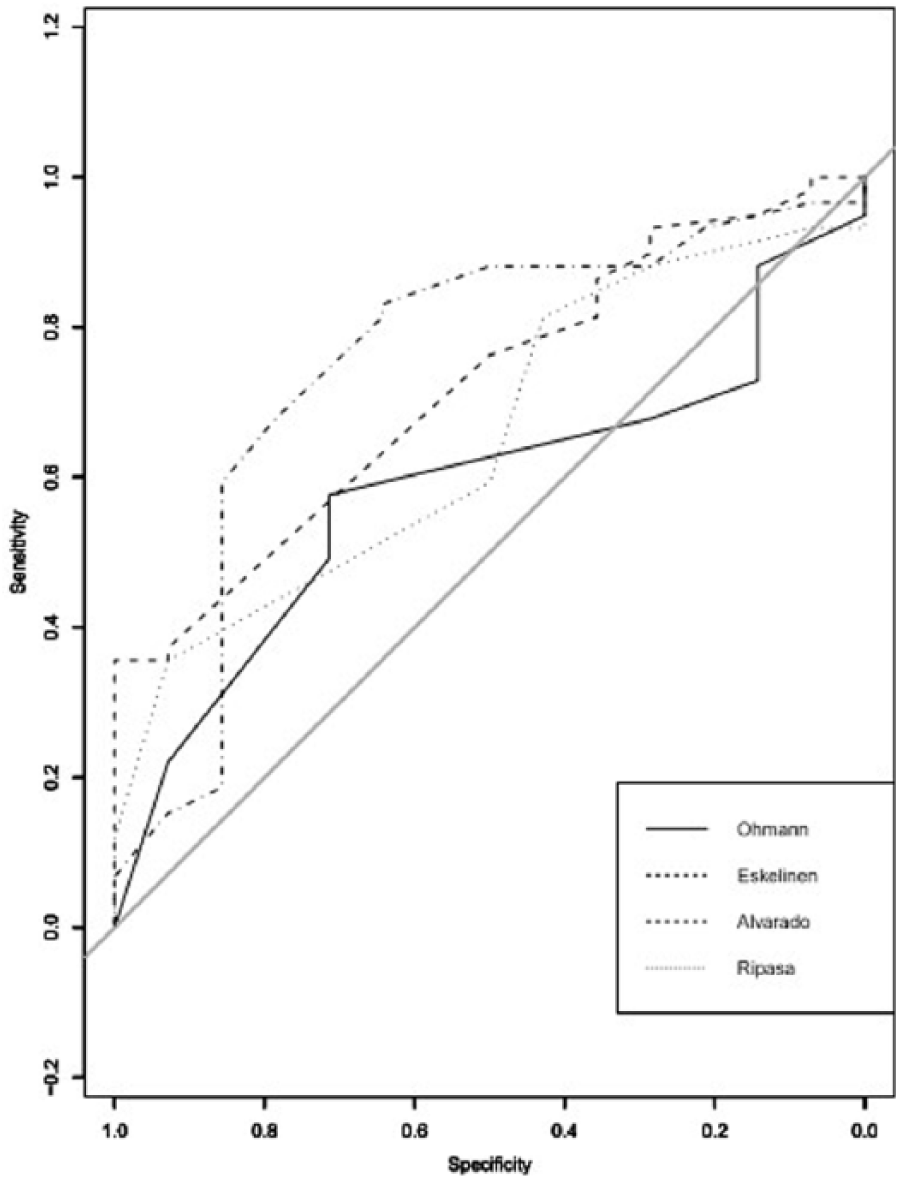
ROC curves of scoring systems.
When the leukocyte values of the patients were examined, it was determined that the mean value was 13,911.5 ± 3721.5 × 103/μL and the cut-off value was 13,900 × 103/μL. Sensitivity, specificity, and positive predictive value (PPV) were 64%, 88%, and 95%, respectively. In ROC analysis, the AUC was found to be 74% (Figure 2).
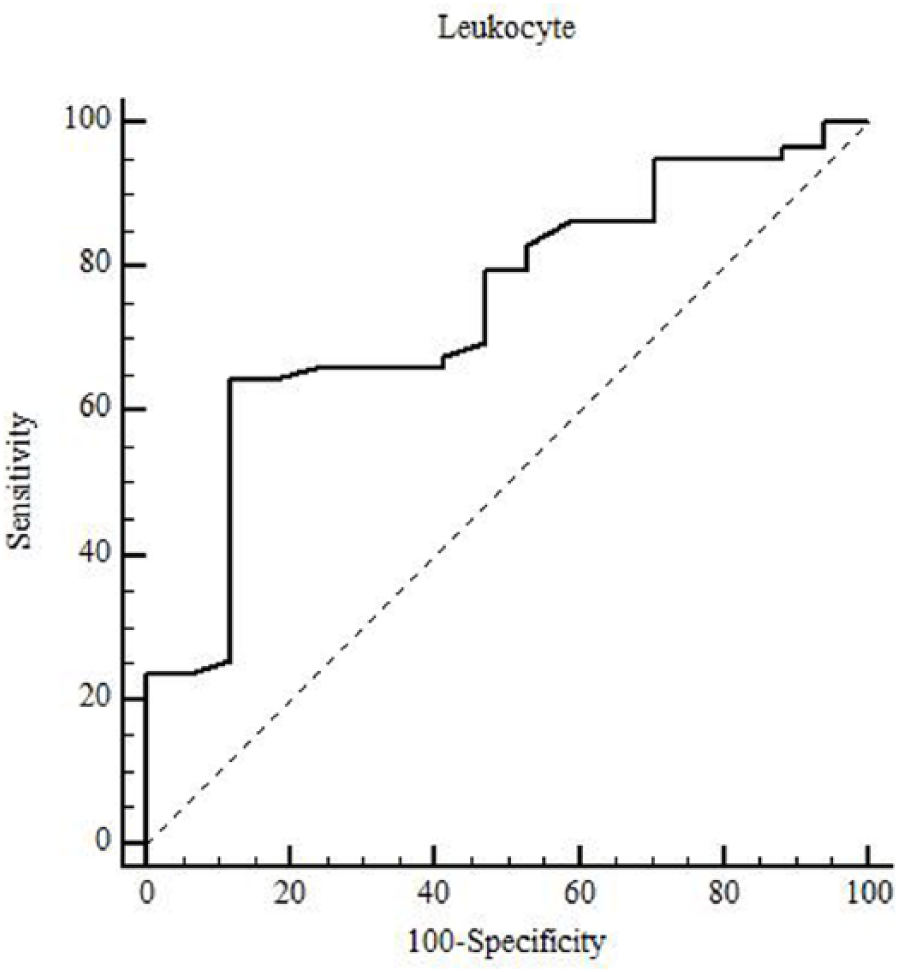
ROC curve of leukocyte count.
Discussion
Acute appendicitis is a clinical condition that has led researchers to search for facilitating methods for diagnosis due to its frequency and the difficulties in differential diagnosis. Delay in diagnosis is an undesired situation which might cause complications such as perforation, peritonitis, and sepsis, resulting seriously in increased mortality and morbidity.1,2 In the beginning, the scoring system was considered as adjuvant in diagnosis and the Alvarado scoring system first appeared in 1986. 3 It has been stated that this scoring system was not sufficient for diagnosis but determined the group of patients to be moved away from the diagnosis better. 4 After the Alvarado scoring system, different scoring systems that are thought to be helpful in the diagnosis of appendicitis came up but they were not enough to lead to a complete diagnosis.
Developed by Ohmann et al., 5 Ohmann scoring system has been presented as easy to use and useful in diagnosis. There are publications in the literature which show that this scoring system is useful in diagnosing acute appendicitis.5–7 In this study, we found that the sensitivity of Ohmann scoring system was 58% and specificity was 71%. Similarly, there are publications that suggest another useful method of diagnosing acute appendicitis in Eskelinen scoring system.2,8 In this study, the sensitivity of Eskelinen and Alvarado scoring systems was found to be 36%, which is lower than in the literature.2,8,9
Being presented later than the other scoring systems, RIPASA scoring system is reported in the literature having a high sensitivity and specificity. 10 It was the scoring system with the highest sensitivity of 68% in our study as well. And its specificity was found to be 71%.
In our study, the cut-off values of Ohmann, Eskelinen, Alvarado, and RIPASA scoring systems were found to be 14, 55.63, 8, and 10, respectively. The scoring system with the highest diagnostic accuracy rate was RIPASA (75%), and the lowest was Eskelinen scoring system (47%).
It is desirable for the scoring systems to have high sensitivity and specificity values. The sensitivity of RIPASA scoring system was found to be the highest (68%) in this study. The specificity of Eskelinen and Alvarado scoring systems was found to be 88% and 82%, respectively.
According to the scores obtained from the scoring systems, three groups were formed according to the literature. 9 They are groups that are less likely to have acute appendicitis, need to be followed, and are more likely to have acute appendicitis (Table 1). In the Ohmann scoring system, values lower than 6 predict low probability, 6–11.5 values predict follow-up, and 12 and above are highly probable for acute appendicitis. This ranking is <48, 48–57, and >57 in Eskelinen scoring system; <4, 5–6, and >7 in Alvarado scoring system; and <5, 5–7, and >7.5 in RIPASA scoring system. These groups were classified 1 for patients with acute appendicitis and 0 for patients with negative appendectomy according to the histopathological examination results (Table 1).
When the data in Table 1 are examined, it is seen that the scoring system that gives the most accurate results in estimating the occurrence of acute appendicitis is RIPASA followed by the Ohmann scoring system. It is also seen that the Eskelinen scoring system is the least effective one to predict acute appendicitis. When the literature is examined, there are publications that indicate that RIPASA scoring system is more accurate and more reliable than other scoring systems.11–13 In our study, RIPASA scoring system was found to give better results, which supports the literature.
The 13,900 × 103/μL cut-off value reached in the ROC analysis of leukocytes in the study is consistent with the literature and is an important indicator of acute appendicitis.1,14 The ROC analysis curve for the leukocyte value is shown in Figure 2. The leukocyte count is an indispensable parameter in scoring systems, which is a laboratory data that surgeons pay attention to in addition to physical examination findings.
Finally, in this research, it was concluded that the RIPASA scoring system is a more reliable scoring system than Ohmann, Eskelinen, and Alvarado scoring systems in diagnosing acute appendicitis.
In cases of suspected acute appendicitis, use of RIPASA in emergency departments where general surgeon is not available or in evaluation of acute appendicitis presence by general practitioners. Thus, we think that the patients will be guided immediately, contributing to the reduction in complications that may arise from delay.
This study was presented as oral presentation at Malatya 1st Gastrointestinal Research Congress, 10 March 2018.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data collection
Zehra Unal Ozdemir, Hakan Ozdemir, Oguzhan Sunamak, Cebrail Akyuz, and Mehmet Torun contributed to data collection.
Data interpretation
Hakan Ozdemir, Oguzhan Sunamak, and Cebrail Akyuz contributed to data interpretation.
Data and materials
All raw data and materials are available on request.
Informed consent
Informed consent of the patients was taken.
Ethical approval
Ethical approval was taken for this study.
Final approval
Final approval was given by Zehra Unal Ozdemir, Hakan Ozdemir, Oguzhan Sunamak, and Cebrail Akyuz.
Human rights
There is no objection to human rights in this study.
Study design
Zehra Unal Ozdemir and Hakan Ozdemir contributed to study design.
Writing
Zehra Unal Ozdemir, Hakan Ozdemir, Oguzhan Sunamak, Cebrail Akyuz, and Mehmet Torun contributed to writing of the manuscript.