
Abstract
Background:
Assessment of geriatric patients presented with abdominal pain had been challenge for emergency physicians with the ageing population. A rapid, reproducible risk stratification model for the assessment of the need for admission for geriatric abdominal pain would be required to identify low-risk patients to be managed as out-patient basis.
Objective:
Assess the feasibility of risk stratification model to predict the need of hospital admission based on readily available bedside parameters in emergency departments.
Methods:
This is a multicenter retrospective cohort study in four emergency departments. Patients aged at least 65 who presented with chief complaint of abdominal pain within the previous 7 days of attendance as the chief complaint were included. Chart review was performed for the included patients. The primary outcome was defined as a composite of mortality, abdominal surgery or endoscopic treatment, and other inpatient treatments for abdominal diseases within 14 days, surrogating the need of hospital admission. Logistic regression was modeled to identify independent predictors. The diagnostic accuracy of the risk model was evaluated with the receiver operating characteristic curve and compared with the clinical gestalt of decision for hospital admission by the attending physician.
Results:
In total, 553 patients were included. Symptoms of upper gastrointestinal bleeding, non-ambulatory presenting status, pain duration, focal abdominal tenderness, hyperglycemia, leukocytosis, and elevated creatinine were independent predictors of the outcome. The area under the receiver operating characteristic curve of the predicted probabilities of the logistic model was 0.741. In keeping for a low-risk criterion to achieve more than 90% sensitivity, the predictive model would only achieve 18.2% specificity which was inferior to clinical gestalt for hospital admission (sensitivity 99.3%, specificity 44.3%).
Conclusion:
Risk stratification model by clinical assessment and laboratory markers alone were inadequate and inferior to clinical gestalt for identification of the group of patients requiring inpatient treatment.
Background
Acute abdominal pain (AAP) ranks one of the most frequent reasons for attendance to emergency departments (EDs) worldwide,1,2 including the geriatric populations. In the reported literature, up to 3%–13% of ED visits of older patients were attending for abdominal pain.3–7 Abdominal pain in elderly had special features of less specific symptoms,8,9 lower diagnostic accuracy, 10 high rate of surgery,11–14 and higher mortality rate.12–14 The problems were further complicated that elderly commonly had multiple comorbidities which would complicate the diagnosis and treatment. 15 Meanwhile, most emergency physicians, unless subspecialized in geriatric emergency medicine, reported being less comfortable when dealing with older patients. 16 Thus, AAP in geriatric patients creates a challenge to emergency physicians. With the aging population, it is anticipated that the number of geriatric patients presented with AAP would be increasing. Universal hospital admission for geriatric patients with abdominal pain would induce significant burden and may not be sustainable with the soaring healthcare needs of the aging population. A risk stratification model for assessment of the need for admission for geriatric abdominal pain would be required to identify low-risk patients to be managed as outpatient basis. The objective of the study was to identify the predictors of the need for admission in geriatric patients with chief complaint of abdominal pain and assess the feasibility of developing a clinical prediction rule based on the bedside readily available parameters in the ED.
Methods
Study design and setting
We performed a multicenter retrospective cohort study in the EDs of four hospitals including two regional hospitals and two tertiary referral centers. The study period was from 1 January 2014 to 31 December 2014. Patients aged at least 65 who presented with chief complaint of abdominal pain within the previous 7 days of attendance as the chief complaint were included. For patients with chronic abdominal pain, they would be included if there is documented acute change in the pattern of pain during the previous 7 days. Subjects would be excluded if there was recent abdominal trauma, surgery, or invasive abdominal procedures within the previous 30 days, or they were admitted with other medical reasons in addition to abdominal pain. The study was performed complying to the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) guidelines for good clinical practice and ethics approval was obtained from the local institutional review board of all study centers (NTWC/CREC/15012, HKEC-15-020, UW 15-157).
Data collection
The data collection procedure was divided into two parts. First in the screening part, all elderly patients who attended the EDs in the study period were retrieved from the hospital electronic databases. A random sample was drawn within the whole cohort of geriatric patients to meet the calculated sample size. Further detailed assessment for eligibility of the selected samples to be included was then performed. Written and electronic medical records were screened if they were presented with abdominal pain and fulfilled the inclusion criteria. The study method was designed to eliminate the potential seasonal effect. For those who fulfilled the inclusion criteria, detailed data on demographics, symptoms, presenting vital signs and examination findings, investigations and outcome were retrieved from written and electronic hospital records. Data collection was standardized with clear definitions of variables and a standard data entry template. Those not documented in the clinical notes were regarded as negative.
Definitions
Abdominal pain was defined anatomically as pain below costal margins to the above inguinal ligaments, including both loin area but excluding pain at the vertebral column. Patients presented with hematemesis, melena, coffee ground vomiting, and coffee ground aspiration from gastric tube were regarded as having symptoms of upper gastrointestinal bleeding (UGIB). Abnormal per rectal examination was defined as pelvic excitation tenderness, rectal mass, melena, or hematochezia. Fever was reported as self-checked temperature of 38°C or above. Plain abdominal X-ray findings were considered as positive if the observed radiological sign is correlating to the abdominal pain.
Outcome
The primary outcome is defined as a composite outcome of mortality, abdominal surgery or endoscopic treatment, and other inpatient treatments for abdominal diseases within 14 days. Other treatments for abdominal diseases included treatments requiring inpatient setting such as infusion of parenteral medications and interventional radiological procedures. The primary outcome was defined as a surrogate to the need for hospital admission and inpatient treatment. The secondary outcomes include mortality within 14 days, hospital admission, and re-attendance for abdominal pain within 14 days.
Statistics
Descriptive statistics were calculated for predictive and outcome parameters. Continuous variables would be expressed as mean and standard deviation and compared using the independent-samples t-test for normally distributed variables. Those with skewed distribution would be expressed as median and interquartile range and compared using Mann–Whitney U test. Categorical variables would be expressed as proportions and percentages and compared using chi-square or Fisher’s exact test where appropriate. p < 0.05 would be regarded as significant for all statistics.
Binominal logistic regression was modeled for the primary composite outcome and mortality, with forward stepwise method based on likelihood ratios. Wald statistics, adjusted odds ratio (OR), 95% confidence interval (CI), and p values were reported. Hosmer–Lemeshow test was adopted to evaluate the model calibration. The model discrimination was evaluated with the area under the receiver operating characteristic (ROC) curve of the predicted probabilities. Cut-off values were adopted and diagnostic characteristics were calculated and compared to the clinical gestalt of the decision by the attending emergency physician to admit the patient to ward. Feasibility of establishing a sensitive and specific predictive model to predict the need for in-hospital treatment was assessed. IBM SPSS version 22 for Windows was employed for statistical analysis (IBM Corp., Armonk, NY, USA).
Sample size was calculated with NCSS PASS 2011 software (PASS 11; NCSS, LLC, Kaysville, UT, USA; www.ncss.com). Sample size was calculated with logistic regression assuming 80% power, 5% level of significance, and two-tailed hypothesis. Effect size was taken to be an OR of 2 for predictors. According to a preliminary survey in one of the centers, the prevalence of primary composite outcome was 20% among geriatric patients with abdominal pain. To identify a binominal predictor with an OR of 2 or more and 20% incidence, a sample of 511 patients would be required.
Results
Patient enrollment
During the study period of 1 January–30 December 2014, the total number of ED attendance in the four study centers was 374,678 (range 78,610–133,048). Geriatric patients aged 65 or above consisted of 23.3% (87,254 attendance, range 12,959–27,229). A random sample of 5166 patients was screened for eligibility to be included. After screening, 553 cases fulfilled the inclusion criteria and they were enrolled for further detailed analysis. The prevalence of abdominal pain among geriatric patients with ED attendance was 10.7%.
Clinical characteristics and outcome
The clinical characteristics and etiology of the study cohort are demonstrated in Table 1 and compared between the positive composite outcome and the contrary group. The positive predictors of the composite outcome in univariate analysis were age, cognitively impaired, and non-ambulatory status in ED. For presenting vital signs, hypotension with systolic blood pressure < 90 mmHg was associated with the composite outcome, while other parameters (including heart rate, body temperature, or the presence of fever) did not demonstrate any association. For the presenting symptoms, duration of pain and symptoms of UGIB were positively associated with the composite outcome. Diarrhea was negatively associated with the composite outcome. For the physical examination findings, focal abdominal tenderness was associated, while generalized tenderness cannot demonstrate any association, with the composite outcome. For ED investigations, leukocytosis, hyperglycemia, creatinine, urea, and hemoglobin were associated with the outcome, while abdominal X-ray cannot demonstrate any association with the composite outcome of need of hospital admission.
Characteristics and etiology of the cohort of geriatric patients presenting with abdominal pain.
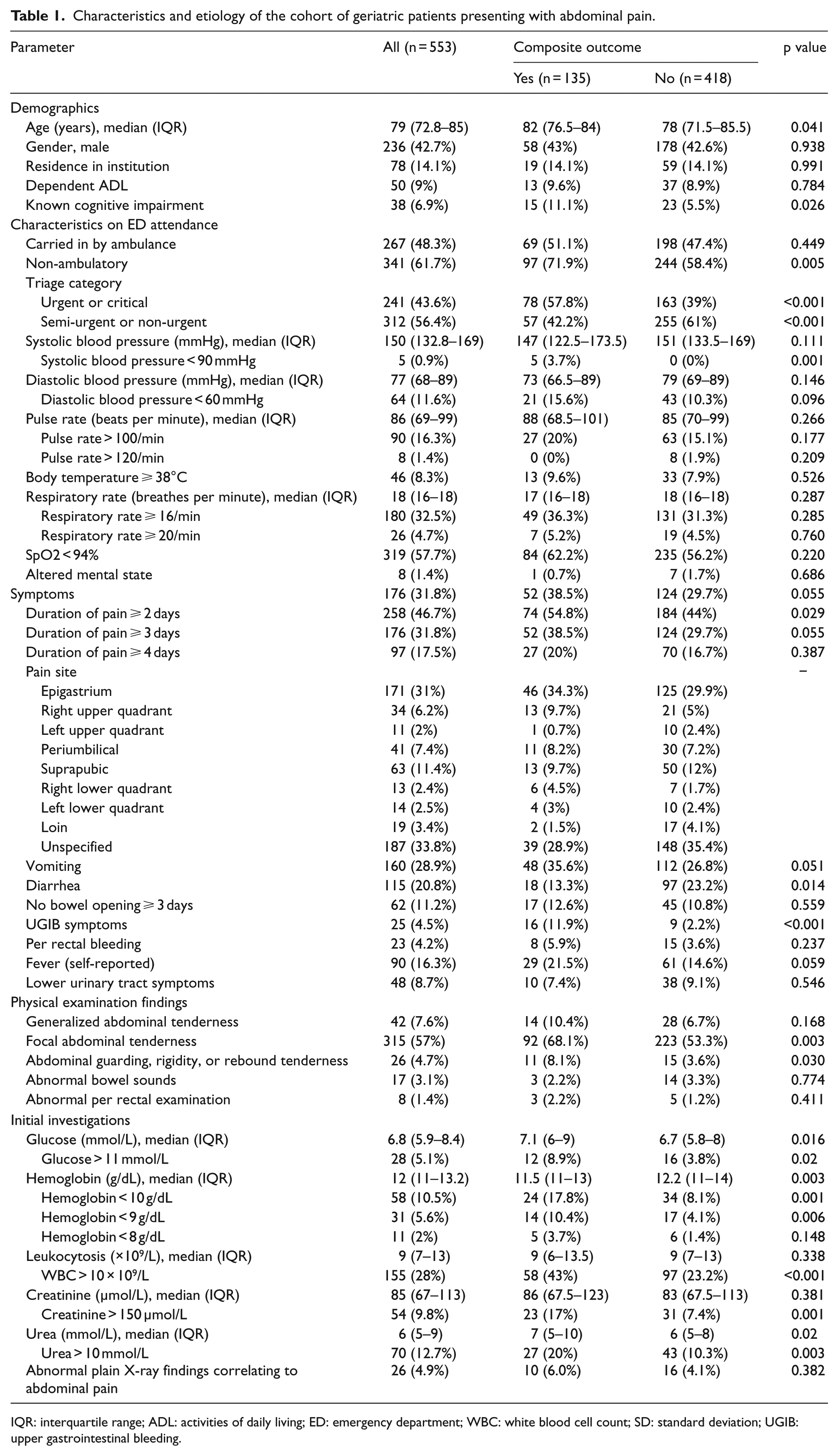
IQR: interquartile range; ADL: activities of daily living; ED: emergency department; WBC: white blood cell count; SD: standard deviation; UGIB: upper gastrointestinal bleeding.
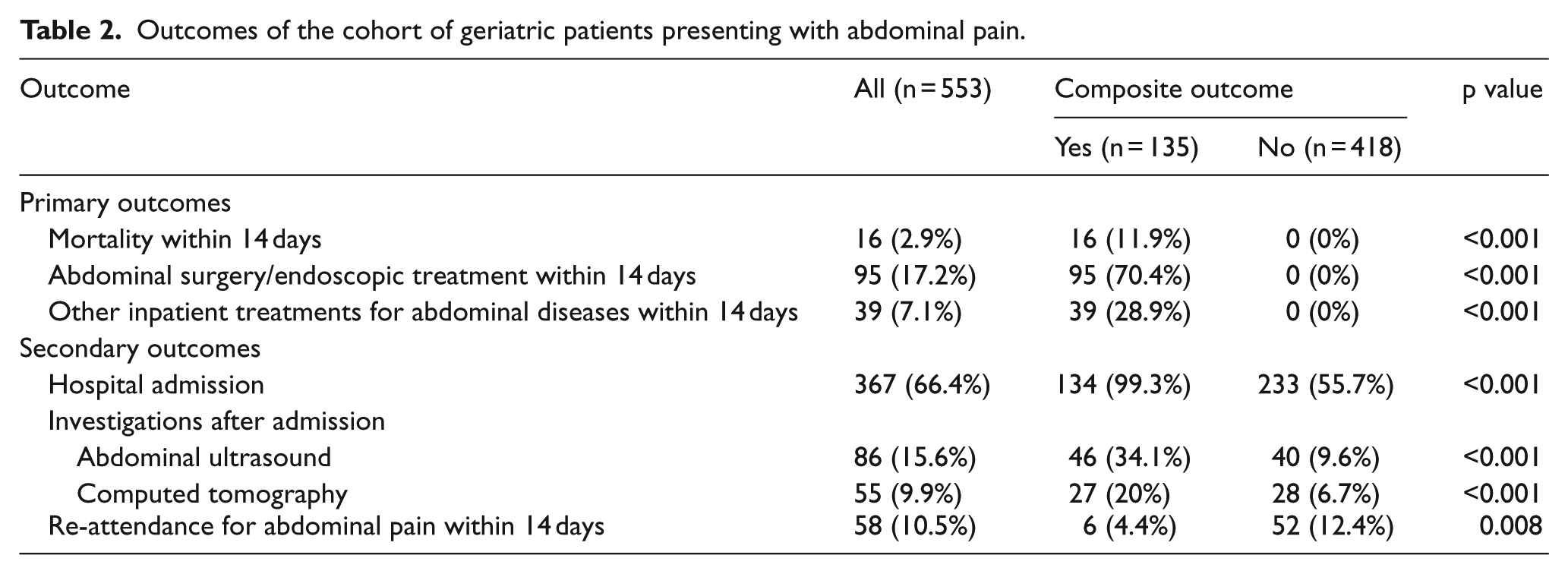
Concerning the outcome (Table 2), the overall hospital admission rate was 66.4%. All except one patient who fulfilled the composite outcome were admitted. Out of the 553 patients, 135 (24%) fulfilled the composite outcome surrogating the need for hospital admission. The re-attendance rate within 14 days was in average 10.5% in the cohort.
Outcomes of the cohort of geriatric patients presenting with abdominal pain.
Predictors of primary composite outcome surrogating the need for hospital admission
Table 3 illustrates the logistic regression model predicting the composite outcome of need for hospital admission. Symptoms of UGIB were highly predictive of the outcome (adjusted OR 6.14). Other independent predictors of the outcome include non-ambulatory status in ED (OR 1.69), pain duration (OR 1.15), focal tenderness on examination (OR 2.02), blood glucose > 11 mmol/L (OR 2.73), leukocytosis (OR 2.11), and creatinine > 150 µmol/L (OR 2.2). Hosmer–Lemeshow test demonstrated satisfactory model calibration with p = 0.220. Area under the ROC curve of the predicted probabilities was 0.741 (95% CI: 0.694–0.789; Figure 1).
Logistic regression predicting outcome in geriatric patients with abdominal pain.
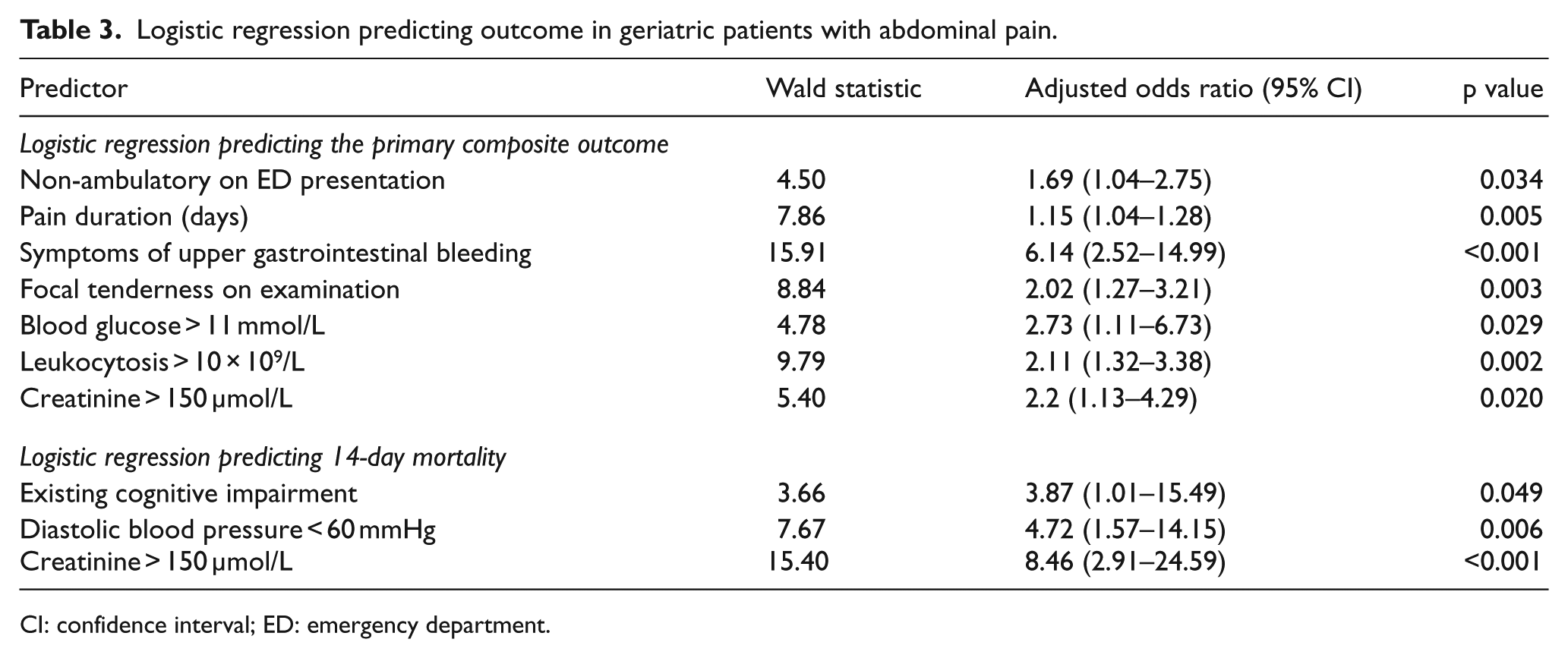
CI: confidence interval; ED: emergency department.
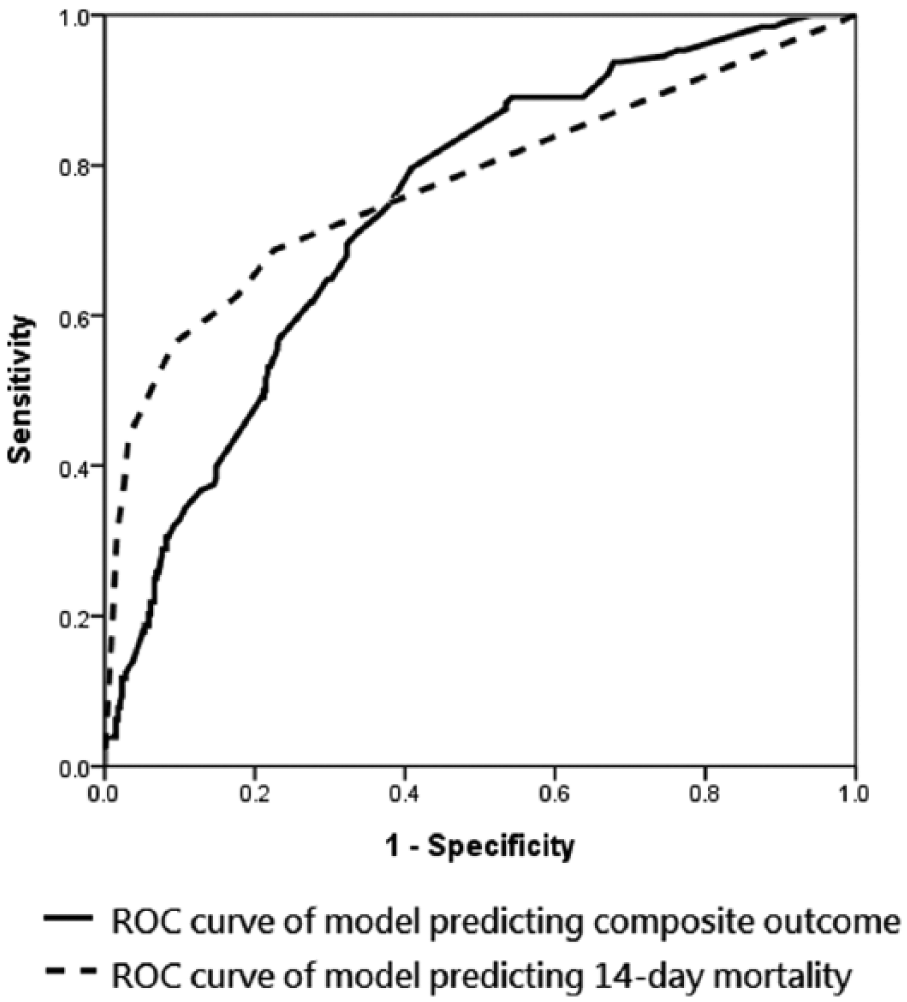
ROC curve predicting outcomes in geriatric patients with abdominal pain.
Predictors of 14-day mortality
Table 3 also illustrates the logistic regression model predicting the mortality at 14 days. Existing cognitive impairment (OR 3.87), diastolic blood pressure < 60 mmHg (OR 4.72), and creatinine > 150 µmol/L (OR 8.46) were significant independent predictors of mortality. Hosmer–Lemeshow test demonstrated satisfactory model calibration with p = 0.395. Area under the ROC curve of predicted probabilities was 0.774 (95% CI: 0.629–0.919; Figure 1).
Feasibility of development of clinical prediction model
Table 4 illustrates the diagnostic characteristics of the predictive model at various cut-offs of predicted probabilities. The best cutoff by Youden’s J statistics was 0.199 (J = 0.373). However, compared to the clinical gestalt by the attending emergency physician for the decision of hospital admission (J = 0.435), the predictive model is inferior. The clinical gestalt for admission had excellent sensitivity and negative likelihood ratio, in keeping specificity of 43.5%. However, for the predictive model achieving more than 90% sensitivity, specificity dropped to 18.2%.
Diagnostic characteristics of the logistic regression model in predicting the composite outcome surrogating the need for hospital admission.
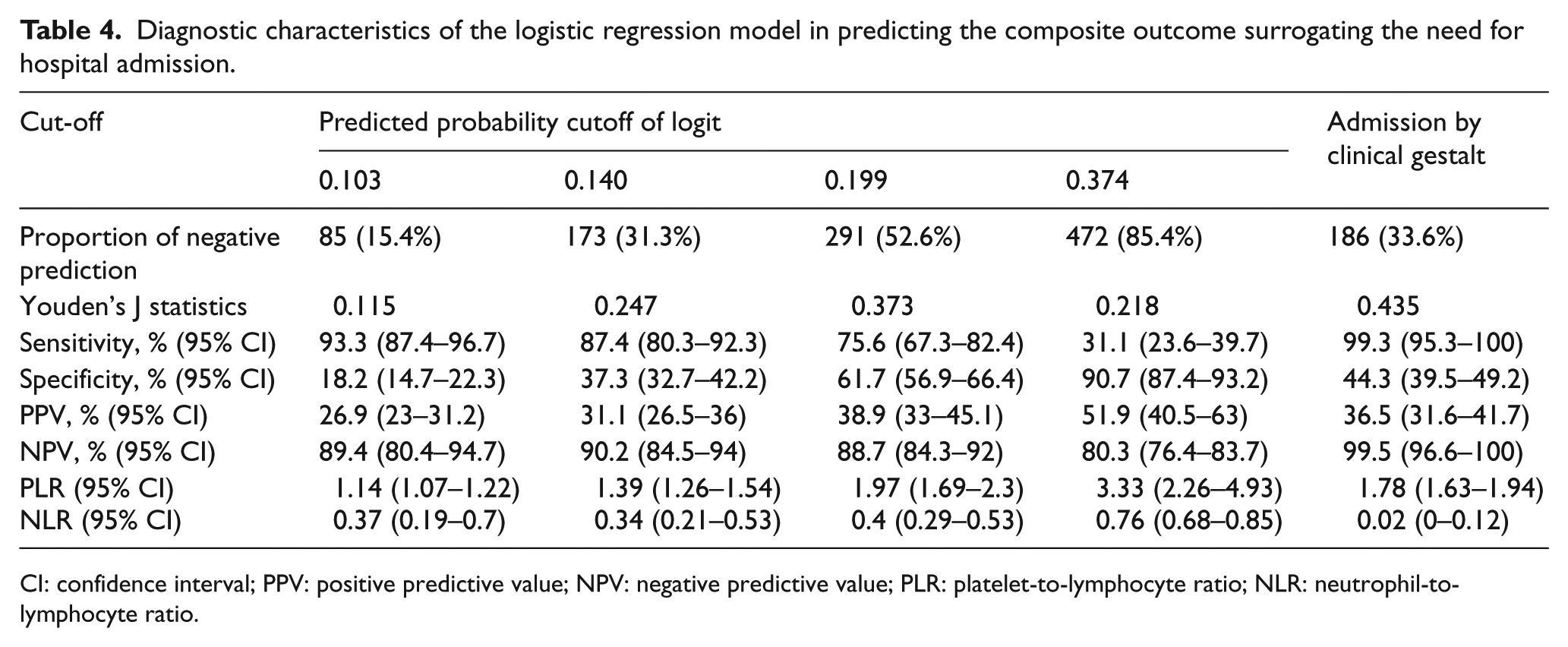
CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value; PLR: platelet-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
Discussion
With the global issue of aging population in developed countries and cities, EDs had been under the pressure of overcrowding and access block.17,18 The concept of geriatric ED had soared in recent decades to accommodate the growing need. 19 AAP accounted for up to 3%–13% of ED visits of older patients.3–6 In the study centers included in this study, the elderly consisted of 23% of all ED attendance during the study period, and attendance for abdominal pain accounted for one-tenth of the geriatric ED attendance. Geriatric abdominal pain had been a consistent challenge to emergency physicians as it was well known that abdominal pain in elderly had special features of less specific symptoms8,9 but higher mortality rate.12–14 Strategies on evaluation had been reviewed but standardization of care is difficult. 20 Therefore, a rapid reproducible risk stratification tool in ED is essential to identify low-risk patients and reduce unnecessary hospital admissions. There had been efforts to identify specific intra-abdominal pathologies for patients with abdominal pain, 21 but risk stratification model in ED for geriatric patients with abdominal pain with bedside readily available parameters is lacking.
Predictors of adverse outcome in geriatric patients with AAP had been explored and investigated in previous studies. Hypotension, abnormal abdominal radiography, leukocytosis, abnormal bowel sounds, and advanced age had been identified as independent predictors of adverse outcome. 22 It is also acknowledged that most physical examination findings were not helpful in identifying patients with adverse outcome. Furthermore, body temperature and laboratory parameters were demonstrated to be not helpful in identifying patients with need for surgery. 23 Most of the previous studied adopted the adverse outcome of mortality. In this study, a composite outcome surrogating the need for inpatient treatment is adopted. The predictors of the composite outcome versus mortality had been rather different (Table 3). Acute kidney injury with raised creatinine had been a predictor of both mortality and composite outcome of in-hospital treatment, while hyperglycemia and leukocytosis would predict the need of in-hospital treatment. Focal abdominal tenderness was the sole physical sign that would predict the need of in-hospital treatment. Symptoms of UGIB had the highest predictive value of in-hospital treatment (adjusted OR 6.1) as most patients would require endoscopic or surgical treatment.
In our cohort, abnormal findings in abdominal radiograph were not predictive of both 14-day mortality and the composite outcome of inpatient treatment. Plain abdominal radiograph had been illustrated in the literature of limited effect in affecting the clinical decision and treatment in ED.24,25 The diagnostic accuracy of plain radiographs in AAP had been limited with particularly limited sensitivity. 26 In recent expert guideline, it was stated that there is no place for conventional radiography due to lack of added value based on clinical assessment. 27 In our study, it was demonstrated that the combination of predictors from clinical assessment and bedside readily available laboratory markers was inferior to the clinical gestalt of the attending physician. The area under the ROC curve would only achieve 0.741. This provided concrete evidence that the clinical assessment and laboratory markers alone are inadequate for ED risk stratification of geriatric patients with abdominal pain. Although in this study the role of inflammatory markers such as C-reactive protein was not evaluated, it was demonstrated in a previous study that the predictive value was limited. 27 An accurate model was proven infeasible for risk stratification of geriatric abdominal pain based on clinical assessment and laboratory markers alone. Addition of more predictive investigations such as sonography and computed tomography (CT) would be required for satisfactory diagnostic accuracy.
In recent years, a stepwise model for imaging advocated with ultrasound serving as the first-line imaging modality. 28 For those with persistent symptoms with negative ultrasound, a contrast CT would be proceeded. 27 Ultrasound has the advantage of being non-invasive and avoiding radiation exposure and the potential hazards, and it is particularly helpful in the evaluation of gallbladder disease and patients with loin pain or renal colic. In the recent years, point-of-care ultrasound has been advocated in both ED and critical care settings. 29 Point-of-care ultrasound for risk stratification of patients of abdominal pain warrants further evaluation, particularly the agreement with sonography by radiologist or other imaging. With more widespread expertise of point-of-care ultrasound among emergency physicians, it may be possible to establish a two-step approach for risk stratification of geriatric patients with abdominal pain, with the first step of risk stratification based on history and physical examination findings, laboratory parameters, and point-of-care ultrasound and CT as the second-level risk stratification tool. 27 A stepwise approach would be helpful to reduce the radiation hazard by CT. 30 A setting of geriatric short-stay observation unit for rapid risk stratification analogous to chest pain units may be explored in geriatric observation medicine. 31 Another approach that is actively under investigation is low-dose CT.32,33 It had been advocated by some experts to replace abdominal radiograph as the first-line imaging modality. Abdominal diseases such as appendicitis and urolithiasis had been demonstrated with good diagnostic accuracies with low-dose CT. 34
Limitations
There are several limitations to this study. First, it was designed retrospectively and subjected to the problem of missing data and retrieval bias. One major residual confounder that we cannot obtain with retrospective design is the severity of pain. Second, the primary composite outcome was only a surrogate of the need for hospital admission. Third, the abdominal radiographic findings were reported by the attending physicians but not reviewed independently by assessors. And some of the other potential laboratory markers such as C-reactive protein and lactate were not evaluated.
Conclusion
Risk stratification model by clinical assessment and laboratory markers alone were inadequate and inferior to clinical gestalt for identification of the group of patients requiring inpatient treatment. Addition of imaging such as ultrasound and CT for the care model would be required for risk stratification of geriatric patient with abdominal pain.
Supplemental Material
Supplementary_material_1 – Supplemental material for Feasibility of predictive model by clinical and laboratory parameters for risk stratification of geriatric abdominal pain
Supplemental material, Supplementary_material_1 for Feasibility of predictive model by clinical and laboratory parameters for risk stratification of geriatric abdominal pain by Chun Tat Lui, Wei Ming Ching, Kwok Leung Tsui, Ho Cheung Chu, Alex To Shing Tsui, Tak Shun Au, Tai Wai Wong, Kit Ling Fan and Ling Pong Leung in Hong Kong Journal of Emergency Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.