
Abstract
Splenic and renal infarctions are embolic conditions which usually occur secondary to cardiac problems, thromboembolic systemic diseases, and infectious conditions such as sepsis. Trauma is a relatively rare cause of visceral infarctions. Traumatic segmental renal infarction associated with total splenic infarction is extremely rare. For detecting these visceral infarctions, contrast-enhanced computed tomography is essential, and a very careful examination is required for detecting very small infarctions and excluding total visceral infarctions. In isolated splenic or renal infarctions secondary to trauma, the common contrast-enhanced computed tomography findings are wedge-shaped or segmental hypodense areas in kidneys or spleen and rarely total visceral infarctions. Usually, intraperitoneal or retroperitoneal fluid collection which corresponds to bleeding from kidney or spleen is not seen in such cases. Also, the lack of evidence of active extravasation from renal/splenic arteries and pseudoaneurysm or dissection is an important finding of isolated traumatic splenic or renal infarctions. Because total infarctions can be misinterpreted in some cases, differences in density between intra-abdominal organs allowed by computed tomography must be carefully examined. Intestinal infarctions, the other abdominal injuries, pulmonary injuries, and pelvic or thoracic bone fractures usually accompany traumatic renal or splenic infarctions. In this report, we present contrast-enhanced computed tomography findings of a multitrauma pediatric case of traumatic total splenic and bilateral segmental renal infarction by reviewing the literature.
A child was admitted to emergency department with a trauma due to fall from height. The patient was comatose at admission and had respiratory distress. A contrast-enhanced thoracic and abdominal computed tomography (CT) imaging was performed. On laboratory examination, there was mild transaminase elevation (aspartate transaminase (AST) was 120 mg/dL and alanine transaminase (ALT) was 108 mg/dL). Hemoglobin level was 11 g/dL. Also, microscopic hematuria was detected on urinalysis. A chest tube was inserted and the patient was transferred to intensive care unit.
Questions
What are the pathological findings of contrast-enhanced CT imaging of the patient?
What is the diagnosis?
Which findings must be kept in mind for making a differential diagnosis?
Answers
Non-enhancing spleen (long arrows in Figures 1–3) and bilateral wedge-shaped hypodense areas in upper poles of the both kidneys (short arrows in Figures 1–4) are seen. Also, pulmonary contusions, right-sided pneumothorax (Figure 5), and liver contusion (Figure 1) are detected.
Traumatic total splenic and bilateral segmental renal infarctions.
The presence of intraperitoneal or perirenal fluid collections corresponding to bleeding from spleen or kidneys and also active contrast extravasation around splenic and renal arteries must be carefully examined, which are seen in the patients with splenic and renal contusions or hematomas that exhibit similar imaging findings. Also, pseudoaneurysm or dissection of splenic or renal arteries must be kept in mind in the case of traumatic renal/splenic infarctions.
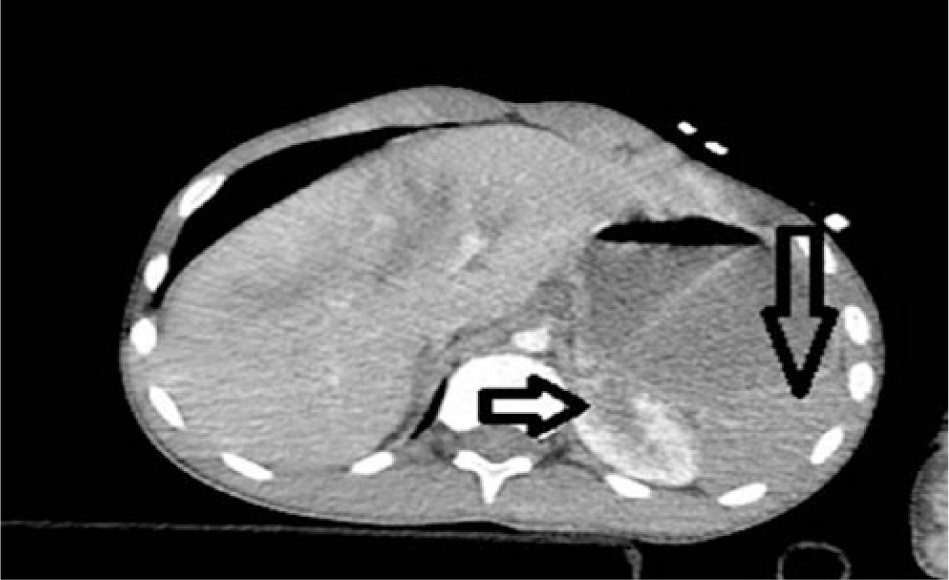
Contrast-enhanced axial CT image.

Contrast-enhanced axial CT image.
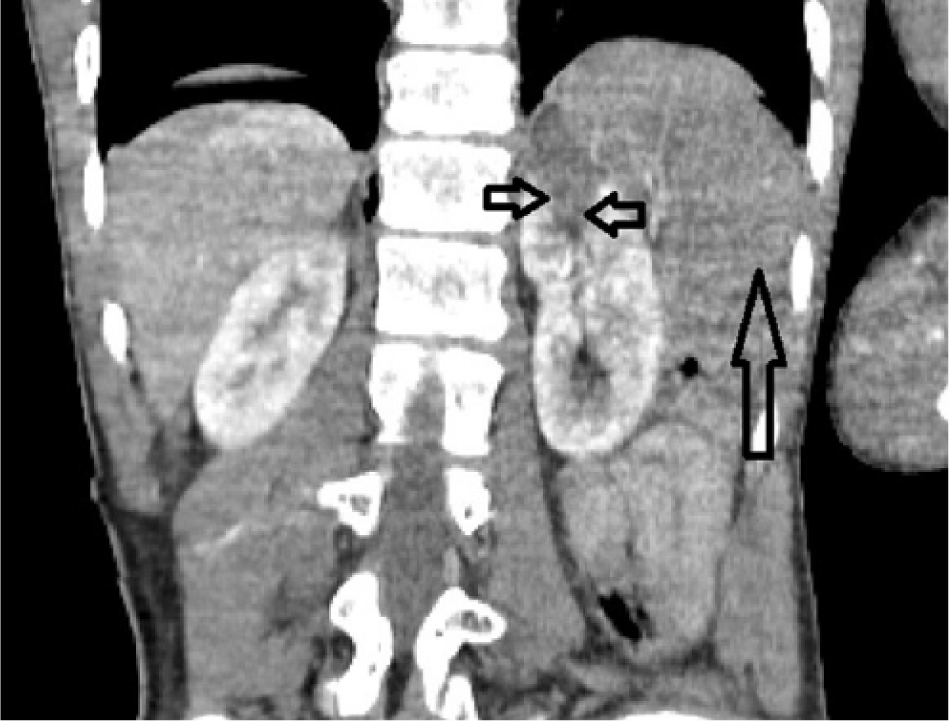
Contrast-enhanced coronal CT image.

Contrast-enhanced coronal CT image.
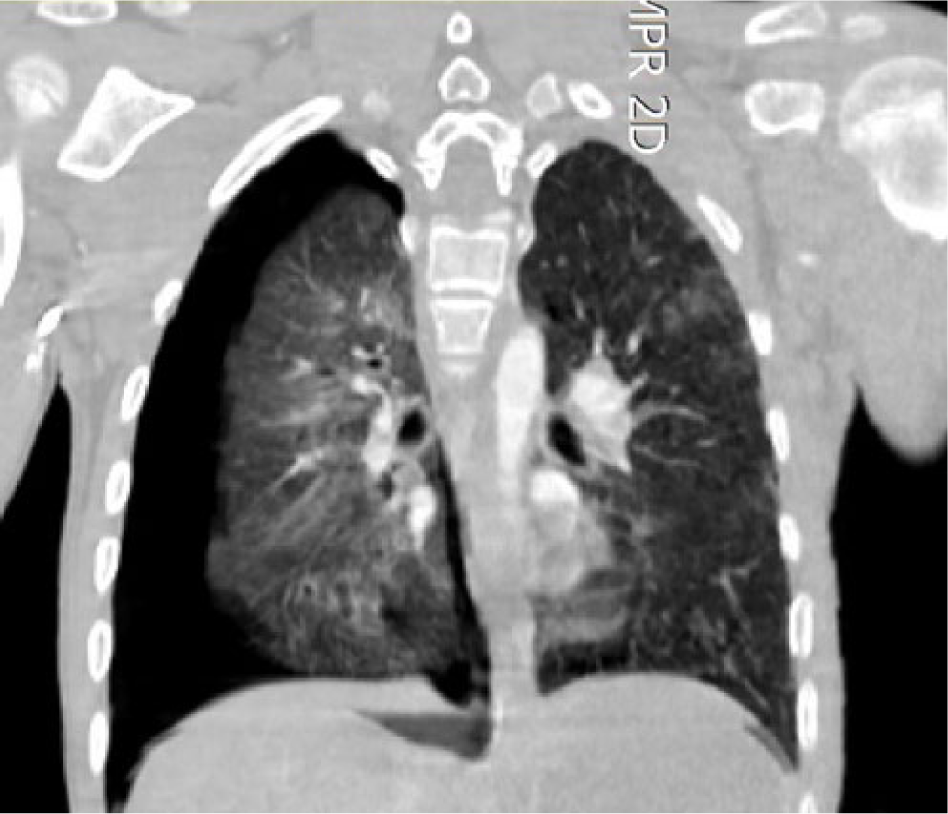
Contrast-enhanced coronal CT image.
Discussion
Cardiac problems, vascular diseases, and thromboembolic conditions are the most common causes of splenic and renal infarctions. But traumatic visceral infarction is rarely reported. 1
Splenic injury secondary to trauma is common. The most common CT findings of splenic injury include contusion, laceration, subcapsular hematoma, post-traumatic pseudoaneurysm, and active hemorrhage (contrast extravasation).1,2 Miller et al. identified 913 patients admitted to their trauma center with splenic injury secondary to blunt trauma. Of these 913 patients, 13 had splenic infarction which was detected on contrast-enhanced abdominal CT. Among their 13 patients, 2 patients had also small (<25%) renal infarctions (one was ipsilateral and the other one was contralateral to spleen). 2
Similar to splenic infarction, renal infarction most commonly occurs secondary to cardiac conditions and hematologic and thromboembolic diseases. Although traumatic renal infarctions are relatively frequent, segmental renal infarction due to trauma is rare. Alevizoupoulos et al. presented a case with a segmental right renal infarction secondary to a traffic accident. They detected a demarcated wedge-shaped hypodense area in kidney on contrast-enhanced tomography. Also, there was no perirenal or intraperitoneal fluid or active extravasation. They observed microscopic hematuria on urinalysis like our case. 3
Romano et al. reviewed imaging findings of 84 patients who were admitted to their department and in whom there was evidence of splenic and/or renal infarction on CT examination. In 10 of these 84 patients, there were both splenic and renal infarctions. They found a traumatic origin in 19 of these 84 patients. Among these 19 patients, they detected both renal and splenic infarctions in two patients. 1
Similar to previous reports, our patient had no intraperitoneal or perirenal hematoma, active extravasation, pseudoaneurysm, or dissection. Also, in our patient, visceral infarctions were also associated with multiple pelvic and thoracic injuries. But our patient had bilateral renal segmental infarctions and total splenic infarction. Because total splenic infarction without intraperitoneal hemorrhage or active extravasation is rare, a total splenic infarction can be misinterpreted as an intact spleen without contusion or hematoma. For detecting very small renal or splenic infarctions and for excluding total visceral infarctions, a very careful examination of contrast-enhanced CT is essential.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.