
Abstract
Background:
The problem that is central to trauma research is the prediction of survival rate after trauma. Trauma and Injury Severity Score is being used for predicting survival rate after trauma. Many countries have conducted a study on the classification, characteristics of variables, and the validity of the Trauma and Injury Severity Score model. However, few investigations have been made on the characteristics of coefficients or variables related to Trauma and Injury Severity Score in Korea.
Methods:
This study examined how the currently used Trauma and Injury Severity Score coefficients were developed and created for trauma patients visiting the emergency department in a hospital in Korea using the analytical method. A total of 34,340 trauma patients who were hospitalized into an emergency center from January 2012 to December 2014 for 3 years were analyzed with trauma registry established on August 2006.
Results:
Trauma and Injury Severity Score coefficients were transformed with the methods that were used to make the existing Trauma and Injury Severity Score coefficients using the trauma patients’ data. Regression coefficients (B) were drawn by building up a logistic regression analysis model that used variables such as Injury Severity Score, Revised Trauma Score, and age depending on survival with Trauma and Injury Severity Score.
Conclusion:
With regard to Trauma and Injury Severity Score established in the United States differing from Korea in injury types, it seems possible to realize significant survival rate by deriving coefficients with data in Korea and reanalyzing them.
Introduction
The evaluation of survival rates is a requisite for the qualitative evaluation of trauma treatments. 1 Trauma and Injury Severity Score (TRISS) is most widely used to compare the measurements of survival rates. 2 That is, TRISS is used to verify the predictions of survival or mortality rates and thus to compare trauma outcomes, while the trauma scoring system ultimately focuses on reducing some preventable deaths. 3 Used to predict the post-traumatic survival rates of adults based on the databases representing the trauma population in major countries, the TRISS model is questioned in view of its validity due to the distinct characteristics of variables and databases in logistic models. 4 The prediction of post-traumatic survival rates is the key point of research on trauma, where TRISS is widely used to predict the post-traumatic survival rates. 5 TRISS was first developed in 1987 based on the US Major Trauma Outcome Study (MTOS) database and revised in 1995. In the latest 2010 version, TRISS coefficients were modified based on the data collected from the National Trauma Data Bank (NTDB) and the National Sample Project (NSP).
When it comes to the validity of TRISS models and the classification of variables and relevant characteristics, each country’s trauma database is used to investigate the validity of TRISS, as the trauma databases differ between countries.
In Korea, researchers have analytically compared TRISS with other trauma indicators. Yet, the characteristics of coefficients and variables of TRISS have never been investigated. Based on the US trauma database, TRISS is incompatible with the injury mechanism and resultant mortality in Korea. Therefore, questions have been raised over applying the existing TRISS to Korean trauma patients. This study is intended to verify the method of extracting the existing TRISS coefficients and to develop a Korean TRISS coefficient model based on the data collected from Korean trauma patients.
Materials and methods
This study was conducted after getting approval by the research ethics committee of Yonsei University (YWMR-15-5-019). The Wonju Severance Christian Hospital Trauma Center, where our study was conducted, opened in 2015 after being designated as the fourth trauma center in South Korea by the Ministry of Health and Welfare. The trauma center is equipped with operating rooms dedicated to trauma surgery, an angiography suite, intensive care unit (ICU), and wards and provides specialized surgical care including emergency medicine, radiology, and anesthesiology.
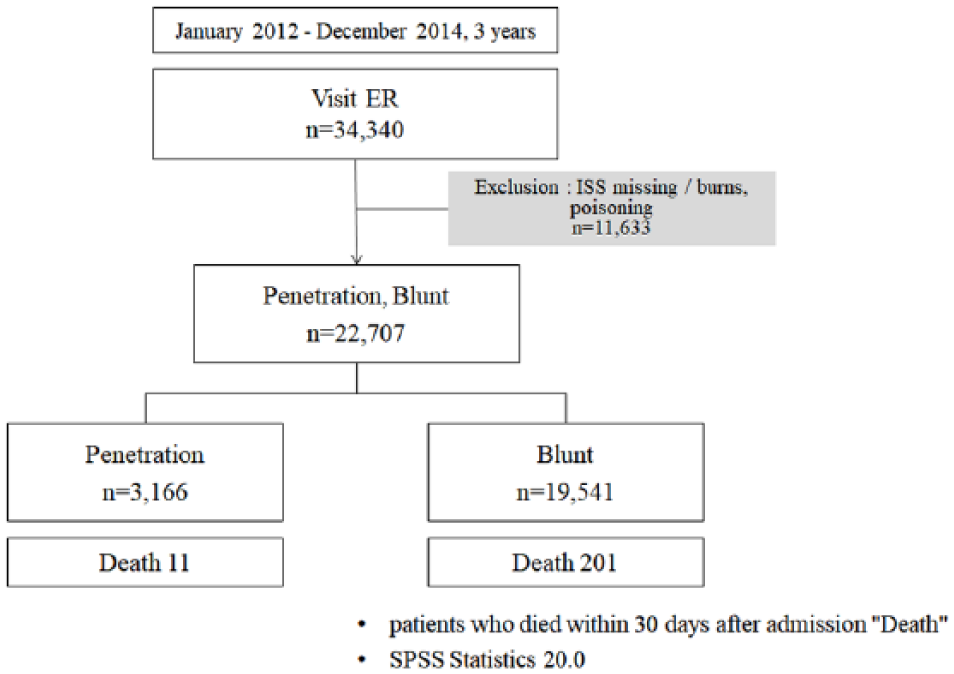
A total of 34,340 trauma patients presenting to the emergency room in an emergency center were analyzed. Transfer cases from another emergency center and patients whose deaths were not correct by Injury Severity Score (ISS) were excluded. Among them, 22,707 patients with blunt and penetrating injuries classified as the S_T under the ICD10 diagnosis code were included as subjects. A total of 11,633 trauma patients were excluded, as their injury mechanisms were associated with foreign substances, burns, and addictions.
The analysis lasted for 3 years from January 2012 to December 2014 (Figure 1).
Inclusion and exclusion criteria.
A trauma registry developed in August 2006 was used to analyze the accumulated trauma database. The trauma registry includes the demographics, epidemiology, physiological parameters of anatomical severities, and clinical conditions of trauma patients presenting to the emergency room. The trauma database built on the trauma registry of each patient is registered and accumulated on the server in the center. Patient information is entered from the arrival at the emergency room to the discharge from the hospital. The physiological parameters used in TRISS calculations reflected those measured at the time of patient outbreak.
To compare mortality, death and survival were categorized. Patients who died within 30 days of hospitalization or died at the emergency room were classified as death and 30 day survival cases were classified into survival groups.
For this study, a trauma registry expert performed a range of tests to verify the completeness, accuracy, and consistency of data. TRISS was developed to evaluate the severity of trauma patients, whose provability survival (Ps) is determined based on the Revised trauma Score (RTS), ISS, and age, where the Ps ranges from 0 (positive death) to 1 (positive survival). The ISS is calculated with the Abbreviated Injury Scale (AIS). AIS coding was entered by well-trained emergency medical residents over the second year and identified by a trauma information coordinator over 3 years’ experience managing the DB (Database). The RTS involves the Glasgow Coma Scale (GCS), systolic blood pressure (SBP), and respiratory rate (RR) variables
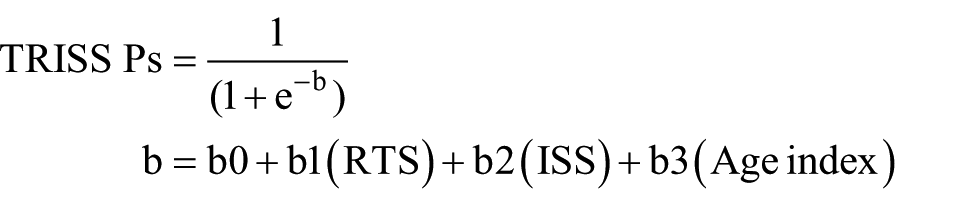
The existing coefficients b0–b3 are the results of the multiple regression analysis of the US MTOS database (Table 1).
Coefficients for outcome norms (trauma.org, TRISS: Trauma Injury Severity Score).

SPSS Statistics 20.0 was used for the statistical analysis. To verify the analytic approach to the development of the US TRISS coefficients, the binary logistic regression analysis was performed, where the survival or death from penetrating and blunt injuries was used as a dependent variable, while the RTS, ISS, and age index were inserted in the ordinal scale (covariance) for analysis to derive the coefficients. Following the foregoing analysis method, this study derived the coefficients from the Korean trauma patient data.
Results
Classification according to injury mechanism
A total of 19,541 blunt trauma patients and 3166 penetrating trauma patients were found among the trauma patients presenting to the emergency room in a regional emergency center. A total of 201 blunt trauma patients died (1.03%), and 11 of the penetrating trauma patients died (0.35%). Between blunt trauma patients and penetrating trauma patients, there are no significant differences in general characteristics and demographic data (Table 2).
General characteristics and demographic data.
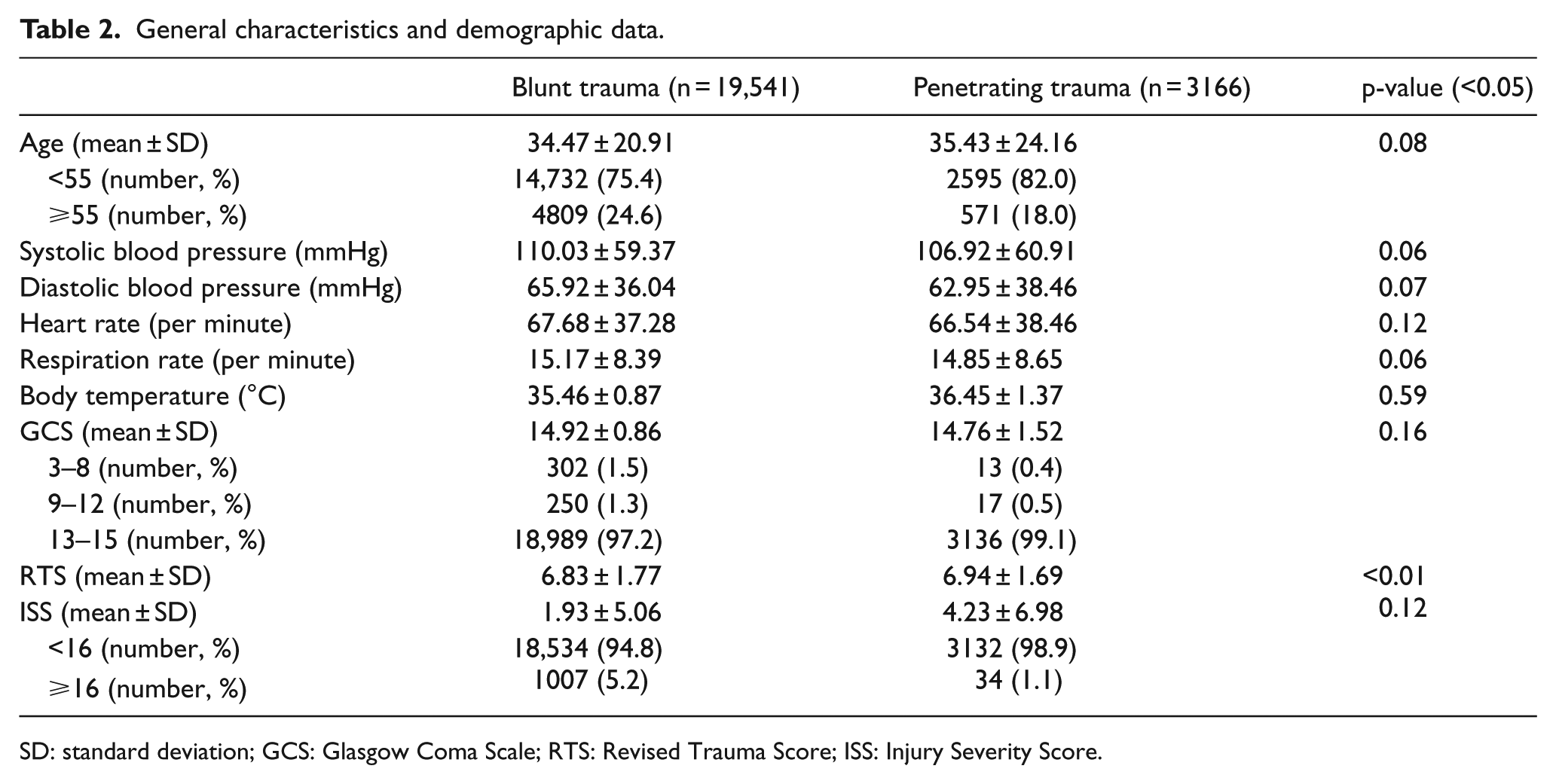
SD: standard deviation; GCS: Glasgow Coma Scale; RTS: Revised Trauma Score; ISS: Injury Severity Score.
Age and mortality distribution according to RTS
One penetrating trauma patient, who scored highest in the RTS (7.8, 0.03 %), and 36 blunt trauma patients (0.18%), who scored 7.8 in the RTS, died (Table 3).
Age and mortality by RTS.
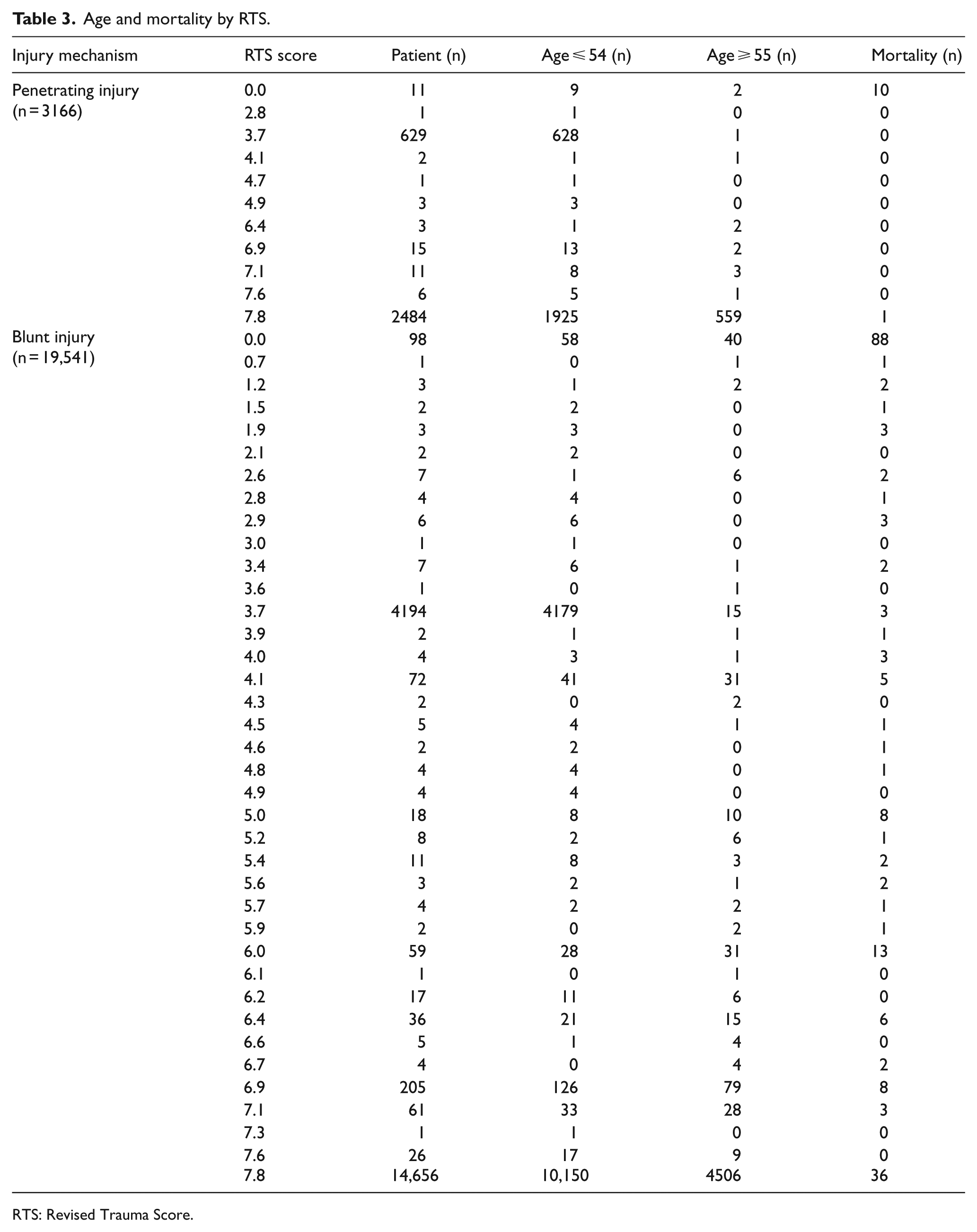
RTS: Revised Trauma Score.
RTS, ISS, and age of penetrating and blunt trauma
With regard to the patients who died from penetrating trauma, the mean RTS, ISS, and age were 0.71 ± 2.35, 49.64 ± 29.99, and 45.55 ± 16.31 years, respectively. With regard to the patients who died from blunt trauma, the mean RTS, ISS, and Age were 3.32 ± 3.26, 40.41 ± 26.60, and 57.00 ± 20.95 years, respectively (Table 4).
Penetrating and blunt trauma of the RTS, ISS and age.
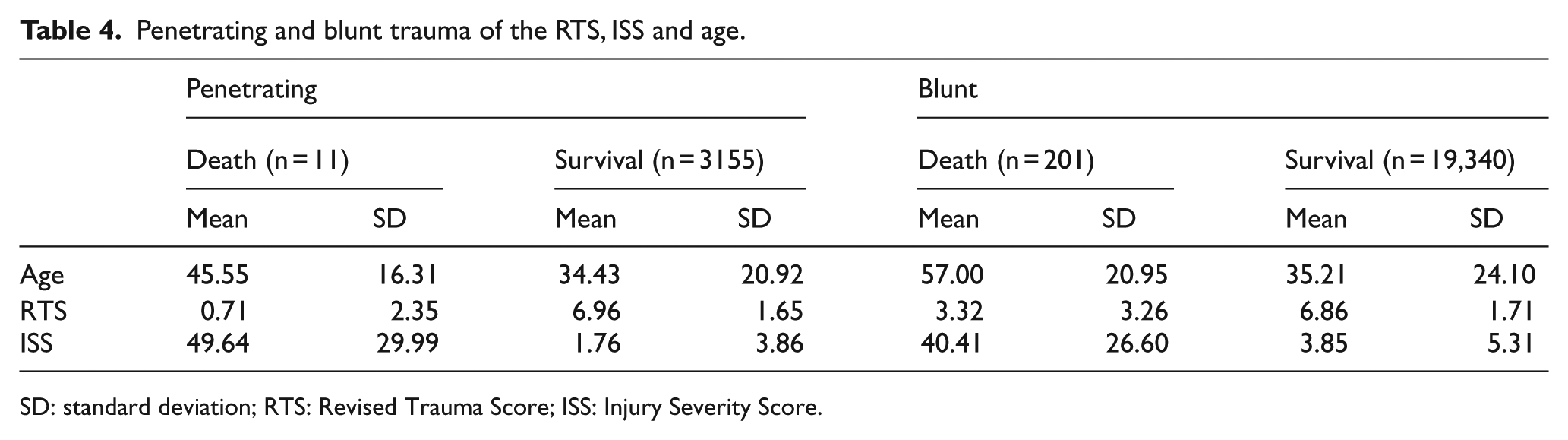
SD: standard deviation; RTS: Revised Trauma Score; ISS: Injury Severity Score.
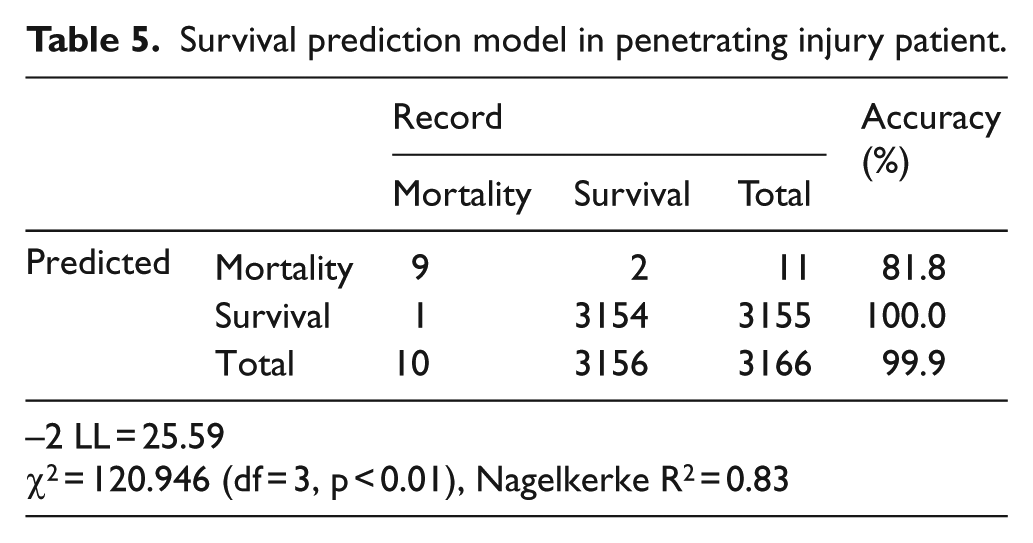
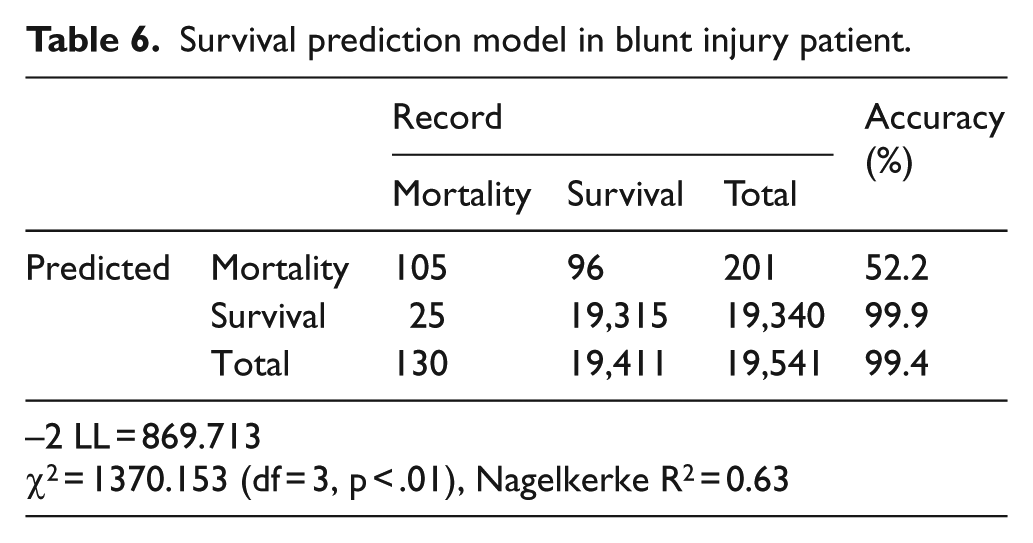
The goodness-of-fit of the model with RTS, ISS, and age predictors was verified with the chi-square scores of 120.95 (p < 0.001) and 1370.15 (p < 0.001) in penetrating and blunt injuries, respectively, which indicates the goodness-of-fit of the model for predicting the survival rates based on the RTS, ISS, and age is statistically significant. The accuracy rates of classification in the penetrating trauma were 81.8% and 100.0% for the death and survival groups, respectively, which indicates that the classification is highly accurate. The total accuracy of classification in the penetrating trauma was 99.9%. The accuracy rates of classification in the blunt trauma were 52.2% and 99.9% for the death and survival groups, respectively, while the total accuracy was 99.4% (Tables 5 and 6).
Survival prediction model in penetrating injury patient.
Survival prediction model in blunt injury patient.
Derivation of TRISS coefficients
In both penetrating and blunt injuries, higher RTS, lower ISS, and younger ages are associated with higher survival rates. The effects of these predictors on the survival or death rates are significant in the order of RTS, age, and ISS. As for the significance probability of each predictor toward the regression coefficients at a significance level of 0.05, the RTS, ISS, and age exert statistically significant effects on survival rates, excluding the age predictor in the penetrating trauma (Tables 7 and 8).
Result of logistic regression analysis for the survival after penetrating injury.
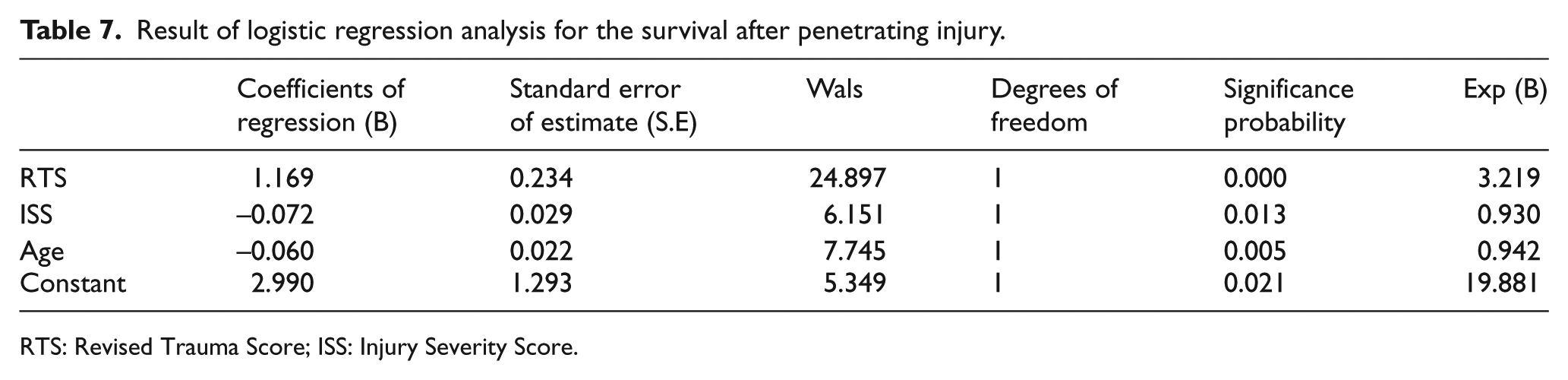
RTS: Revised Trauma Score; ISS: Injury Severity Score.
Result of logistic regression analysis for the survival after blunt injury.
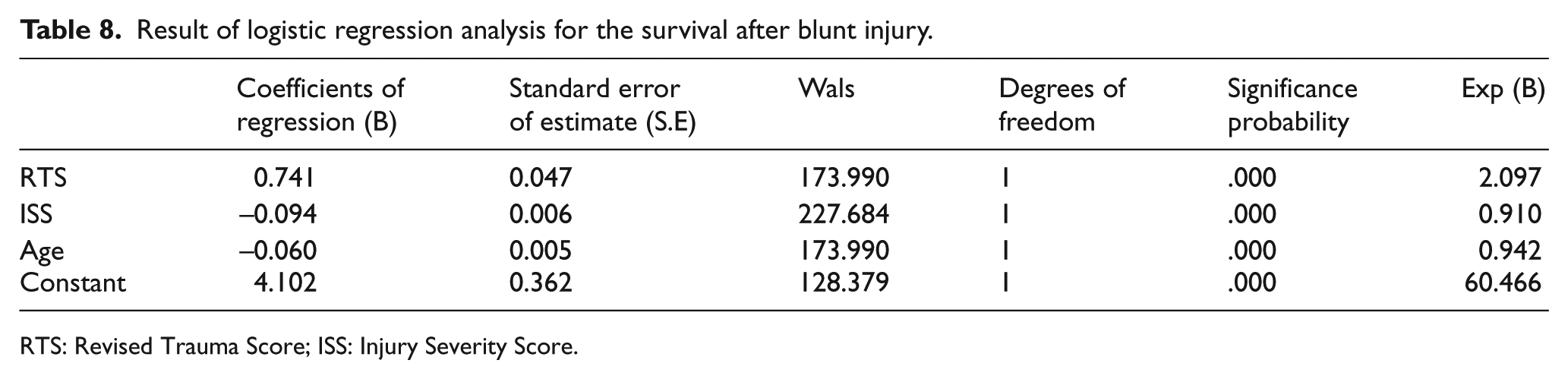
RTS: Revised Trauma Score; ISS: Injury Severity Score.
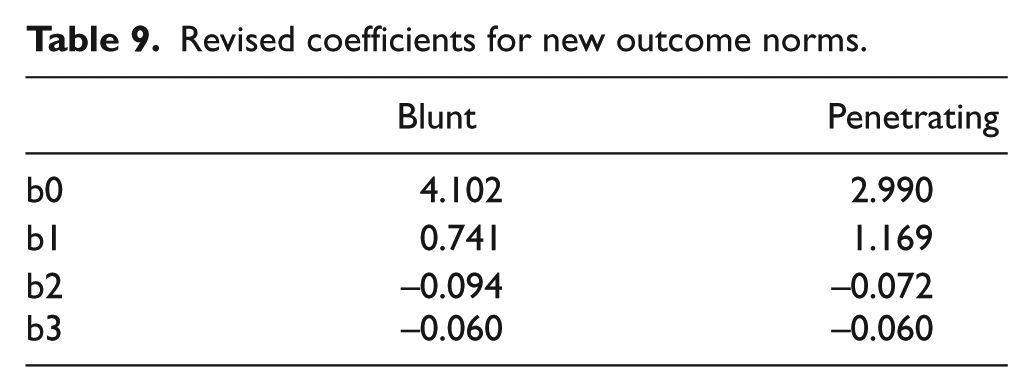
Table 9 shows the regression coefficients (B) in the logistic regression analysis model, where the ISS, RTS, and age are used as predictors for the survival or mortality rates associated with penetrating or blunt injuries among trauma patients presenting to a regional center (Table 9).
Revised coefficients for new outcome norms.
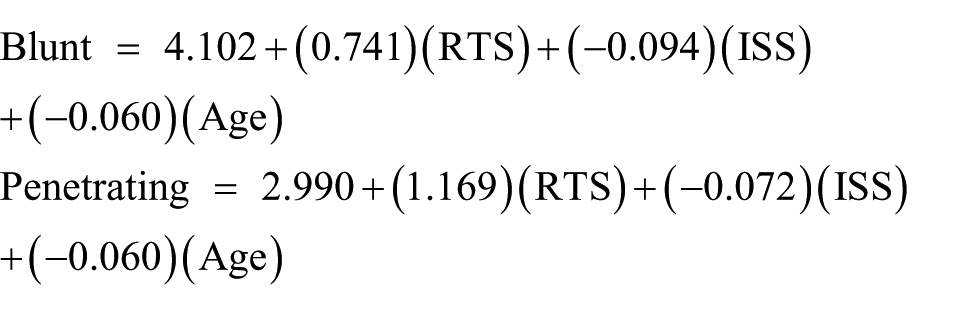
The calculated logistic regressions are as follows:
When we performed the analysis on TRISS of United States and Korea using receiver operating characteristic curve (ROC) curves, the area under the curve (AUC) of Korea TRISS was 0.933 which was higher than that of United States at 0.916 (Figure 2).
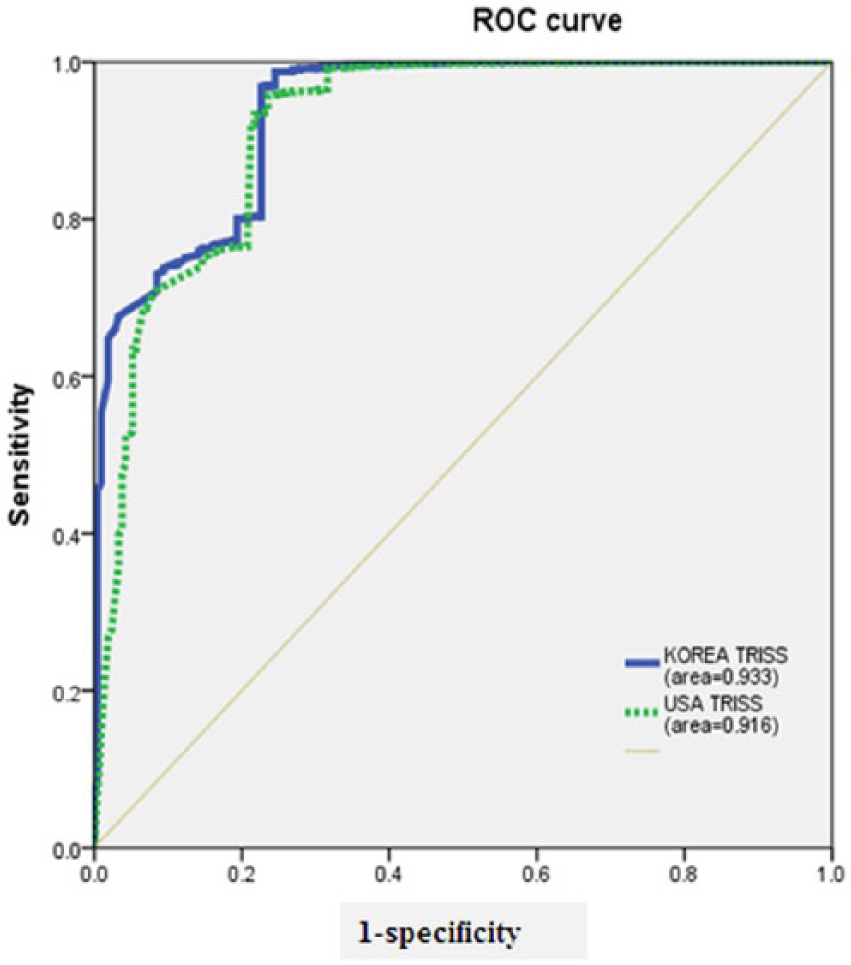
TRISS of United States and Korea using ROC curves.
Discussion
As trauma is acknowledged as one of the world’s leading causes of death across all age groups, diverse trauma indicators have been developed and used in many countries to objectively quantify the severity of traumatic injuries. 6 As the most frequently used instrument, TRISS has been extensively investigated in terms of revalidation of coefficients and alteration of variables, which is attributable to the cross-national differences in the aspects of trauma deaths.7,8
Ever since its introduction, TRISS has continuously changed over the last two decades. Treatment for trauma patients has been improving with advanced statistical methods evolving, while other outcome measures have been devised. Despite the perceived limitations regardless of its advancement, TRISS has been most widely used in hospitals to determine the quality of trauma care and to monitor the trauma mortality. 9 In that TRISS requires such data as AIS and GCS, which are hard to collect, research has been conducted to develop a simple model for predicting the survival rates on the basis of easily available patient information. 10 Yet, few studies on TRISS have been conducted in Korea.
Previous studies have reported that TRISS is more accurate in predicting the prognosis of trauma patients in Korea than RTS or ISS. 11 However, previous studies mostly focused on either comparative analyses of TRISS and relevant indicators or prediction of prognoses in patients with trauma relevant to certain injury sites.12–15
Recently, a study on the analysis of TRISS coefficients for blunt trauma patients has been published, and the trial is encouraging. However, further studies are needed to make more accurate predictions of prognosis for trauma patients. 16
TRISS was first developed in the United States based on the country’s trauma patient data. As Korea differs from the United States in terms of socio-cultural environment and thus trauma characteristics, it is challenging to predict the survival rates of Korean trauma patients with the established TRISS. TRISS is a conventional retrospective methodology of estimating the expected survival rates of trauma patients. That is, in TRISS, the injury mechanism is sub-divided into blunt and penetrating injuries to predict the survival rates of trauma patients with the logit regression analysis modeling drawing on the ISS, RTS, and age variables in each patient group. Following the method of constructing coefficients of TRISS, the regression coefficients (B) of ISS, RTS, and age were derived from the trauma patient data in a regional center, depending on their survival.
Penetrating injuries of the United States capture 21% of the total injuries, reflecting such a large range of injuries. 17
In Korea, however, it is difficult to discover the significance of comparative analysis for the penetrating injuries, as most of the injuries are caused by blunt trauma.
Since there is a difference in the rates of damage mechanism and also a difference in the resulting rate of mortality, it is expected that the difference between the actual rate of survival and the expected rate of survival will be even less when the TRISS coefficient made of the Korean data rather than the US TRISS coefficient is applied.
In Korea, most trauma patients were associated with blunt injuries, which led to a higher mortality. In light of the predictive validity regarding mortality, most penetrating injuries were intentional (e.g. self-injury, suicide, and violence), resulting in the small difference between the expected and actual survival rates.
Recent research on TRISS has confirmed a few limitations and questioned the validity of methodology specific to certain types of trauma. 3 Researchers in many countries have exerted efforts to improve TRISS by analytically benchmarking local data against the US database. In Hong Kong, researchers have attempted to improve the existing TRISS model based on data involving Asian trauma patients. 1 For the betterment of outcome prediction, a study altered the variables in this model for analysis, for example, gender and age and found that the revised model predicted the outcomes more significantly than the existing TRISS model. 18 Also, in altering other variables, the ISS could reduce the severity in case of concentrated severe injuries on a certain site, as it used the three highest AIS scores per body part. 19 Research was conducted to verify the NISS (New Injury Severity Score) proposed to address the foregoing issue. In a comparative analysis to predict the mortality of trauma patients, the NISS had more effects on mortality than the ISS. 14 As such, researchers in different countries have conducted comparative analyses of the existing TRISS by altering relevant variables.
The existing TRISS involves coefficients derived from the MTOS data, whereas the proposed coefficients extracted from the trauma patient data in a regional center hardly represent the entire trauma patient population in the country. Thus, government-supported subsequent efforts should be made to ensure that the proposed coefficients represent the entire trauma patients nationwide, particularly by managing the quality of collected trauma patient data and rectifying any missing data. Despite current emphasis on trauma, there is a paucity of data concerning the regional distribution of severe trauma patients, etiology, severity, and mortality. 20 The data collection and quality management underlie the development of trauma management indicators, estimation and monitoring for evaluating the relevant effects of the system, and thus need be given priority. Above all, a system for collecting trauma patient data need be set up. However, it is difficult to include a number of healthcare institutions nationwide in the system due to lots of efforts and costs. 19 In addition, although research has demonstrated that TRISS has been substantially improved, further studies should delve into appropriate reclassification, TRISS modeling, and designation of coefficients. 2 The current survival prediction system need be adjusted based on the development of major trauma registries in all regions and data analysis and applied to a comparable population. 21 The injury severity indicators should be developed based on the understanding of trauma-related dynamics and the quality management of objective pre- and post-treatment data. 22 Once the foundation is laid, TRISS-related coefficients should be derived and verified continuously, while variables need be altered and analyzed, given the characteristics of trauma patients differ between countries. The TRISS coefficients derived from Korean trauma patients are conducive to increasing the predictive accuracy of mortality among Korean trauma patients.
Coefficients derived from patients visiting a single center are far from representing a national model. The accuracy of actual and predicted mortalities will increase when the predicted mortality is evaluated with the coefficients derived from the data collected in hospitals across the nation.
As this study is limited in that all injuries include penetrating wounds and blunt traumas, we plan to analyze a nationally representative sample of patients with a high severity injury with ISS >15 in the follow-up study.
Using the Korean trauma patient data, the Korean logit regression analysis model is characterized by the following: Blunt = 4.102 + (0.741)(RTS) + (–0.094)(ISS) + (–0.060)(Age) and Penetrating = 2.990 + (1.169)(RTS) + (–0.072)(ISS) + (–0.060)(Age).
It seems possible to determine some significant survival rates with the Korean-specific coefficient formula by applying Korea trauma patient data to the proposed coefficients and the current TRISS coefficients based on the US database and by comparatively analyzing the results.
Footnotes
Acknowledgements
This thesis has become a reality with the undying support and love of my beloved professors. The authors wish to thank Choi Eun-hee, Research support team of University of Yonsei, Korea, for his helpful comments. The authors show gratitude to those who have helped to finish the long journey of writing this thesis. I.H.K. contributed to the study design, data collection, data analysis and interpretation, literature search, and writing. K.H.L. contributed to the the study design, data collection, data analysis and interpretation, literature search, and writing. H.Y. contributed to the data collection, data analysis and interpretation, and critical revision. J.I.L. contributed to data collection and data analysis. H.Y.L. contributed to the data collection and data analysis. K.S.B. contributed to the critical revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Trauma patients presenting to the emergency room in a Wonju severance Christian hospital region emergency center were analyzed. The analysis lasted for 3 years from January 2012 to December 2014.
IRB approval
YWMR-15-5-019
Human rights
As a retrospective study based on medical records, there is no conflict with the human rights of patients and consent is not required, as we have said before.