
Abstract
Background:
New psychoactive substances are constantly evolving structural analogues of traditional drugs of abuse that have become a threat to public health worldwide and within our locality. An understanding of the local pattern of new psychoactive substance use will help guide frontline clinical management.
Objectives:
This study was conducted to review the new psychoactive substances detected in cases referred to the authors’ laboratory (a tertiary clinical toxicology centre), as well as the associated clinical features and toxicological findings.
Methods:
All cases referred to the laboratory for toxicology analysis between January 2009 and December 2017, and which were analytically confirmed to involve new psychoactive substance use, were retrospectively reviewed. Demographic data, clinical features and toxicology findings were studied.
Results:
A total of 111 cases involving 104 patients and 22 types of new psychoactive substances were identified, with an increasing trend in the number of cases and subclass of new psychoactive substances detected. Up to half of the cases (n = 64) were related to the use of 2-phenyl-2-(ethylamino)-cyclohexanone (2-oxo-PCE, a ketamine analogue); other new psychoactive substances detected included para-methoxymethamphetamine, 4-fluoroamphetamine, phenazepam, 3-trifluoromethylphenylpiperazine, 5-methoxy-diisopropyltryptamine, 2-diphenylmethylpyrrolidine, methoxyphenidine, the N-methoxybenzyl drugs, cathinones, synthetic cannabinoids and opioids. Among the acute poisoning cases attributable to new psychoactive substance use, the severity was fatal (n = 3), severe (n = 17), moderate (n = 67) and minor (n = 17). And 11 patients required intensive care unit admission. All three fatal cases were associated with para-methoxymethamphetamine use.
Conclusion:
A rising trend of new psychoactive substance use is observed locally, which is associated with considerable morbidity and mortality. Continued vigilance from frontline clinicians and medical professionals is imperative in the combat against new psychoactive substance use.
Introduction
New psychoactive substance (NPS) refers to ‘substances of abuse, either in a pure form or a preparation, that are not controlled by the United Nations drug conventions, but which may pose a public health threat’. 1 These emerging substances of abuse, marketed to the public as ‘legal highs’ or ‘designer drugs’, are often synthesized as structural analogues to the traditional drugs of abuse in an attempt to produce similar psychotropic effects while at the same time evading detection and other legal regulations. Despite international efforts to combat against NPS use, there has been a continuous surge in NPS detected globally over the last decade, as reflected by the increasing variety of NPS detected, as well as in the quantity of such drugs seized. 2
Although NPS resemble existing illicit substances structurally, their clinical effects and toxicological profiles have not been well characterized. Numerous cases of intoxication and fatalities associated with their use have been reported worldwide. 3 The problem is further complicated by difficulties in the analytical detection of NPS, which is often hindered by the rapid transformation of their chemical structures, the unavailability of reference standards and the limited coverage of these agents in routine toxicology laboratories. In Hong Kong, NPS is also a growing public health concern; nevertheless, only isolated case reports or case series related to their use have thus far been published.4–9 A review of the pattern of NPS use in Hong Kong will be useful to frontline medical professionals.
The first cluster of NPS poisoning in Hong Kong involving the piperazine derivatives was reported in 2009 by the authors’ laboratory, 7 which provides centralized tertiary toxicology service to all institutions within the Hospital Authority (HA). In particular, the laboratory receives referrals for NPS-related cases based upon suspicious drug history or toxicology findings, atypical clinical features associated with using drugs of abuse or conversely a typical clinical toxidrome but with negative findings in the initial toxicology screen. Analytical platforms have been developed within the laboratory that allow the simultaneous detection of conventional drugs of abuse as well as a constantly expanding panel of NPS in patient specimens.10,11 Specialized methodologies were employed where necessary to identify these protean and chemically diverse compounds.4,5,8 In this study, a retrospective review on the NPS detected in cases referred to our laboratory over the previous 9 years, as well as the associated clinical features and toxicological findings, was conducted.
Methods
All cases referred to the authors’ laboratory for toxicology analysis between January 2009 and December 2017, and which were analytically confirmed to involve NPS use, were retrospectively reviewed. Clinical data were collected by reviewing the laboratory database and medical records of the patients. Demographic data, clinical features, medical and drug history as well as laboratory findings were reviewed. This study has been approved by the Hospital Authority Kowloon West Cluster Research Ethics Committee (KW/EX-17-110(114-11)). Written informed consent was not necessary because no patient data have been included in the manuscript.
Patient urine specimens were subjected to routine toxicology screening that includes common drugs, drugs of abuse and NPS. Where indicated by drug history or suspicious clinical or analytical findings, specialized methodologies for detecting NPS not originally covered in the routine toxicology screening were employed.4,5,8 Specimens were subjected to liquid–liquid extraction followed by trimethylsilyl (TMS) derivatization and general unknown screening by gas chromatography–mass spectrometry (GC-MS) and/or solid-phase extraction, followed by sample concentration and analysis by liquid chromatography–tandem mass spectrometry (LC-MS/MS). 11 For the latter, multiple-reaction monitoring (MRM) or enhanced product ion scanning was employed for the confirmation of NPS. The chromatographic retention time, GC-MS spectrum, MRM ratio and/or product ion spectrum of the patient samples were compared against the reference standard material for positive identification of drugs.8,11
Drug samples, where available, were subjected to general toxicology screening by high-performance liquid chromatography diode array detection (HPLC-DAD) followed by confirmation on a time-of-flight mass spectrometer (TOF/MS), as published previously. 5 The identity of drugs was confirmed by exact mass and comparison of the retention time and ultraviolet (UV) spectrum with the reference standard.
Results
During the 9-year study period, 111 cases involving 22 types of NPS were identified. All cases were referred from 14 different local hospitals belonging to the HA. The referral departments were as follows: Accident & Emergency (n = 51), Medicine (n = 46), Psychiatry (n = 9), Orthopaedics (n = 3), Paediatrics (n = 1) and Surgery (n = 1). Among the 104 involved patients, 77 (74%) were male. The median age was 33 years (range 16–54 years).
The types and subclasses of NPS detected over the 9-year period are summarized in Table 1 and Figure 1. The total number of NPS encounters was 117. The most frequently encountered NPS were 2-phenyl-2-(ethylamino)-cyclohexanone (2-oxo-PCE; n = 64), para-methoxymethamphetamine (PMMA; n = 11) and phenazepam (n = 10). The 64 encounters related to 2-oxo-PCE, a ketamine analogue, occurred as a poisoning outbreak in late 2017. 12 Figure 1(a) shows the number of NPS of different subclasses encountered each year between 2009 and 2017 (Figure 1(b) shows the same data excluding the 64 cases related to 2-oxo-PCE to avoid skewing of data).
The number of encounters of each NPS detected across the 9-year study period.
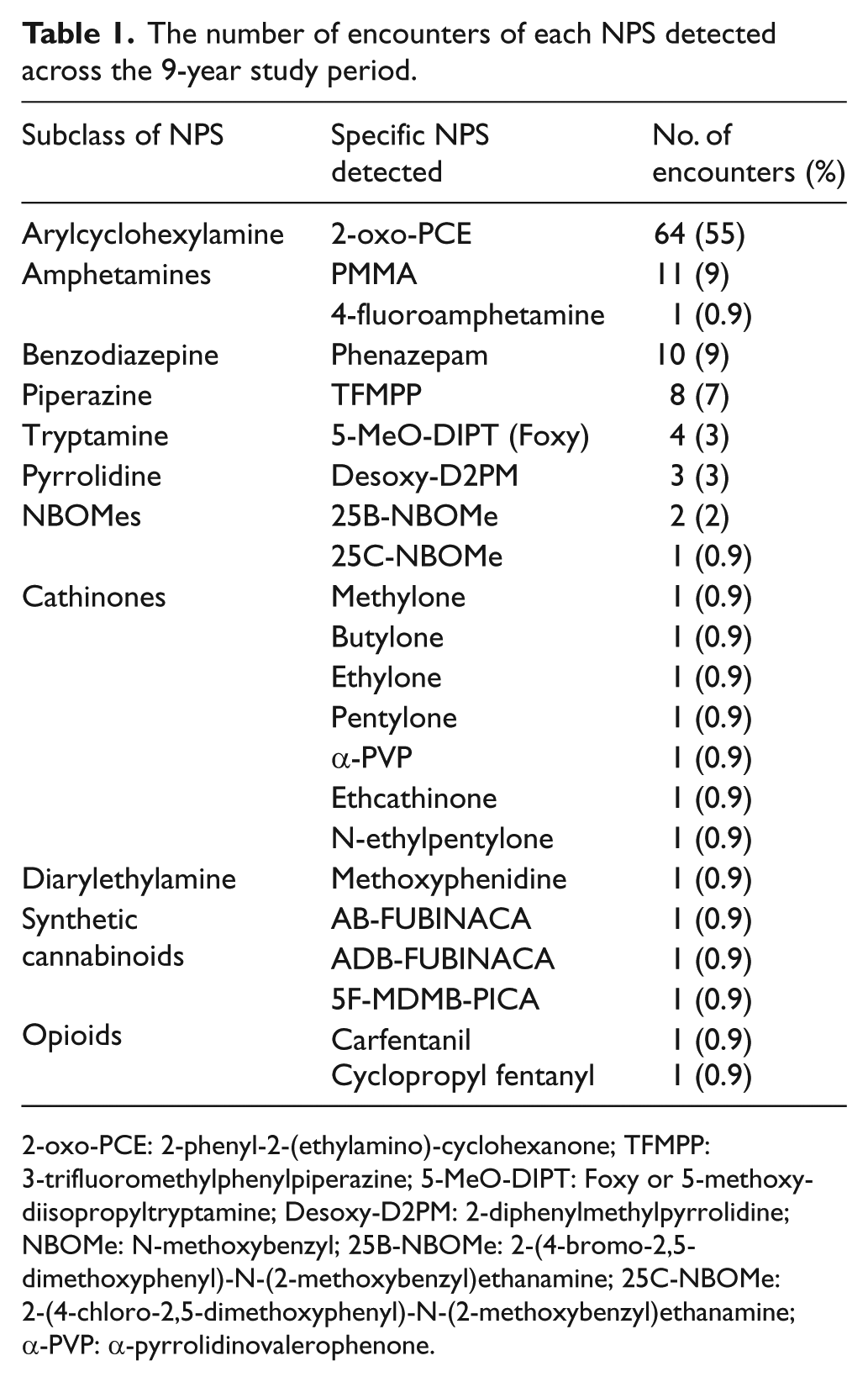
2-oxo-PCE: 2-phenyl-2-(ethylamino)-cyclohexanone; TFMPP: 3-trifluoromethylphenylpiperazine; 5-MeO-DIPT: Foxy or 5-methoxy-diisopropyltryptamine; Desoxy-D2PM: 2-diphenylmethylpyrrolidine; NBOMe: N-methoxybenzyl; 25B-NBOMe: 2-(4-bromo-2,5-dimethoxyphenyl)-N-(2-methoxybenzyl)ethanamine; 25C-NBOMe: 2-(4-chloro-2,5-dimethoxyphenyl)-N-(2-methoxybenzyl)ethanamine; α-PVP: α-pyrrolidinovalerophenone.
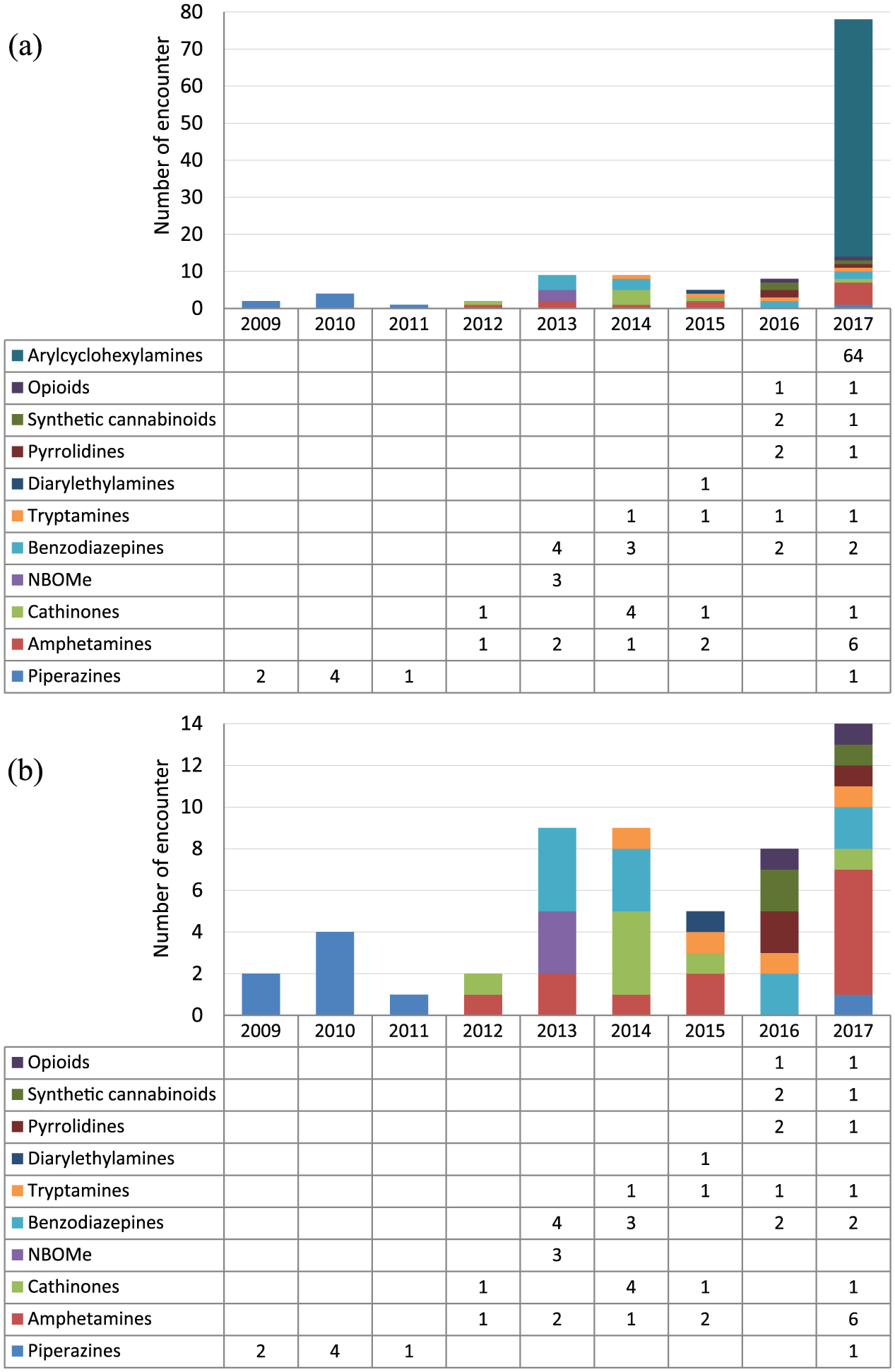
Number of NPS of different subclasses encountered each year (a) including and (b) excluding the 64 cases related to 2-oxo-PCE in 2017.
Overall, 76 cases (68%) required hospital admission, while 11 cases (10%) required intensive care unit (ICU) admission. Most of the patients presented with neuropsychiatric manifestation (n = 97; 87%) including confusion/impaired consciousness (n = 49), agitation (n = 16), convulsion (n = 10) and hallucination (n = 7), followed by cardiovascular involvement (n = 69; 62%) including hypertension (n = 46) and tachycardia (n = 37), as well as musculoskeletal involvement (n = 28; 25%) including 17 cases of rhabdomyolysis. 13 Among the 111 cases, NPS was an incidental finding in 7 cases (patient admitted for non-NPS-related conditions). For the remaining 104 poisoning episodes attributable to NPS use, the severity was assessed according to the poisoning severity score (PSS) 13 and the results were as follows: fatal (n = 3), severe (n = 17), moderate (n = 67) and minor (n = 17). There were 10 cases with NPS-related fatal or severe poisoning requiring ICU admission; among these, three 2-oxo-PCE cases have been detailed in another report. 12 A summary of the remaining seven cases is given in Table 2.
Summary of fatal and severe poisoning cases that required ICU admission and were attributable to NPS use.
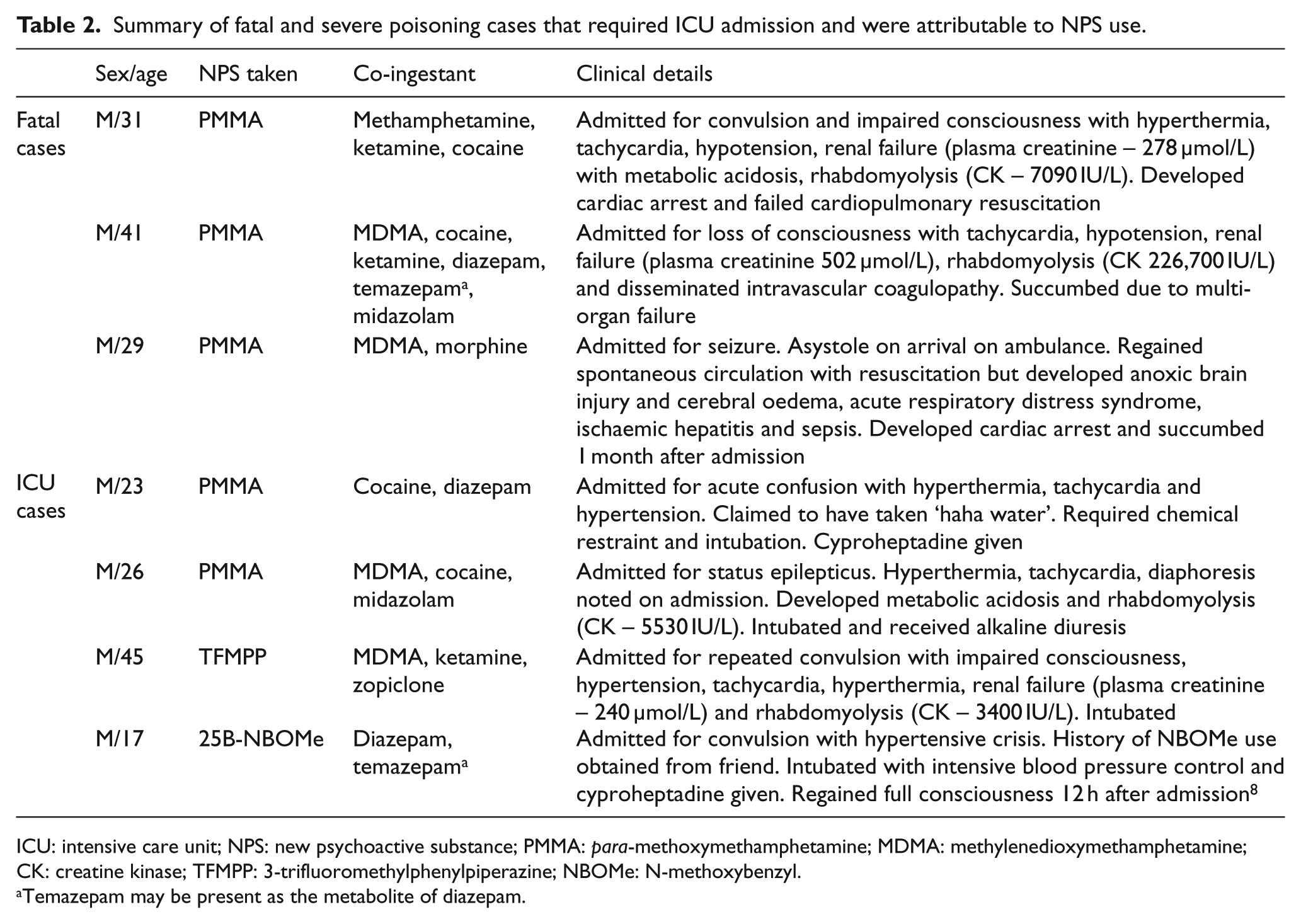
ICU: intensive care unit; NPS: new psychoactive substance; PMMA: para-methoxymethamphetamine; MDMA: methylenedioxymethamphetamine; CK: creatine kinase; TFMPP: 3-trifluoromethylphenylpiperazine; NBOMe: N-methoxybenzyl.
Temazepam may be present as the metabolite of diazepam.
Among the 111 cases, 25% of patients (n = 28) volunteered a history of psychoactive drug use at presentation, with four patients being aware that they have been taking some form of NPS. The NPS taken by the patients were claimed to be obtained over the Internet or overseas, at parties or from friends. Three patients reported a history of slimming agent use, which had been analytically confirmed to be the source of NPS (2-diphenylmethylpyrrolidine (desoxy-D2PM)). Such slimming agents were available in local convenience stores.
Regarding the pattern of drug use, co-ingestion of other substances of abuse was frequently noted (n = 62; 56%), with a maximum of seven drugs of abuse detected in one case, and an overall average of two substances per case. The three most common co-ingestants include ketamine (n = 30; 27%), cocaine (n = 30; 27%) and methamphetamine (n = 26; 23%).
Discussion
The aim of this study was to review the pattern of NPS use in Hong Kong from a clinical laboratory’s perspective. The nature of the authors’ laboratory as a tertiary toxicology centre specializing in NPS allows the centralization of NPS-related clinical poisoning cases in our unit. To the best of the authors’ knowledge, this is the largest cohort reported in our locality at the time of writing.
The current data show the emergence of a variety of NPS in Hong Kong in the recent years, including different subclasses such as the amphetamines, synthetic cannabinoids, cathinones, tryptamines, piperazines, N-methoxybenzyl (NBOMe) derivatives and opioids. This is consistent with the global data demonstrating diversity both across and within subclasses of NPS.2,14–16 It is interesting to note that prior to 2013 the number and variety of NPS detected were relatively limited compared to those in the subsequent years (Figure 1). This may be explained by increased awareness of clinicians as well as the dramatic increase in the analytical coverage of NPS within the authors’ laboratory in the latter years of the study, both in terms of the availability of reference standards and technical expertise.
One of the striking findings of this study was the surge in NPS use in 2017, which was mostly accounted for by the outbreak of 2-oxo-PCE, also known as deschloro-N-ethyl-ketamine late that year.4,12 Putting aside these cases of 2-oxo-PCE, a steady rise in the overall number and variety of NPS detected is still appreciable over the years, which is alarming given the likely underestimation of NPS use (discussed below).
Compared with traditional drugs of abuse, by nature NPS display a more dynamic pattern of use, changing as new substances emerge. As shown in Figure 1(b), the abuse of 3-trifluoromethylphenylpiperazine (TFMPP; a serotonin receptor agonist of the piperazine class) was mainly clustered around 2009–2011, while the NBOMe drugs – highly potent and toxic hallucinogens8,17 – were only detected in 2013. The synthetic opioids started appearing only in the recent 2 years, which is consistent with the trend reported by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). 2 On the other hand, certain NPS such as the amphetamines, cathinones, phenazepam and 5-methoxy-diisopropyltryptamine (5-MeO-DIPT) were detected relatively constantly over the years.
The use of NPS in our cohort is associated with significant morbidity and mortality. In 87 (78%) cases, patients developed moderate toxicity with PSS grade 2 or above (although the effect of other co-ingested drugs of abuse should not be discounted). Out of the 10 severe cases (including three fatalities), 5 were related to the use of para-methoxymethamphetamine (PMMA), a methoxy derivative of methamphetamine. PMMA has a slower onset of action but higher toxicity, rendering them much more dangerous with numerous deaths reported worldwide.18,19 2-oxo-PCE was also associated with three severe poisoning cases. 12 Although synthetic opioids were not involved in any severe cases in this study, they are known to be highly potent and toxic. 20 With multiple fatalities reported and their rapid emergence in the recent years, 21 this group of NPS warrants our attention.
The analytical detection of NPS is often a challenge due to their protean nature, diverse chemical structures and lack of published analytical information as well as of reference standards. The identification of synthetic cannabinoids, a diverse group of cannabinoid receptor agonists, is of particular analytical difficulty for several reasons: (1) small dose taken and consequently minute biological concentrations, often in the low ppb levels;22,23 (2) this group of NPS is known to undergo extensive metabolism, frequently to overlapping metabolites; 23 and (3) the synthetic cannabinoids are consistently the largest group of NPS reported to EMCDDA each year. 2 The result is a vast, constantly expanding pool of parent drug and metabolites of close structural homology and low biological levels, and little is known about their pharmacology, toxicology and analysis. Specialized methodologies and highly sensitive analyzers are often required for their analytical detection. This considerable analytical challenge may be reflected in the relatively low frequency of detecting synthetic cannabinoids in this study (only two isolated cases involving three drugs) despite the large number of such compounds emerging each year. 2 An alternative explanation is that the prototype itself, cannabis, is in general not commonly abused locally. 24
Early identification of an emerging NPS is vital for effective prevention and harm reduction. It allows the timely alert of (1) frontline physicians to facilitate better clinical management, (2) legislative units to make necessary changes to the control of new drugs and (3) social units to educate the general public. To facilitate their early identification, monitoring of NPS should first be a proactive and continuous process. 10 Second, NPS methods need to be ‘non-targeted’ with the coverage being easily expandable. One of the key NPS detection systems in this study employed a ‘targeted’ approach, where only signals of a predefined list of compounds were captured. 11 On the other hand, non-targeted methods, for example, utilizing time-of-flight or other full-scan mass spectrometers, allow the capture of all the signals within a sample. Such methods are more useful for NPS detection where the candidate drug is often unknown at the beginning, and are becoming the method of choice worldwide.16,25,26
This study has several limitations. First, there is likely to be underestimation of the prevalence of NPS use in the general population. Mild cases that might not have presented to hospitals or fatal cases that proceeded directly to coroner investigation would not have been captured presently. Moreover, only cases that were referred to the authors’ laboratory due to specific toxicological concerns or suspicious laboratory findings were included. A surveillance rather than such ‘case finding’ approach will provide a better reflection of the true prevalence of NPS use. Second, the number and types of NPS present locally are also likely to be underestimated due to the non-exhaustive analytical coverage of NPS within the laboratory, in contrast to the constantly expanding pool of such compounds. Third, the interpretation of the toxicity associated with NPS in this study was often confounded by the co-ingestion of other drugs of abuse.
The global NPS epidemic is partly fuelled by the easy accessibility of the drugs nowadays. Alarmingly, this study found that desoxy-D2PM (which is a methamphetamine analogue with alleged appetite suppressing properties) was easily obtainable in local convenience stores marketed as a weight reduction product. 6 More importantly, the ease of obtaining NPS through the Internet nowadays means that we will continue seeing the penetration of these ever-emerging and potentially dangerous substances into the drug scene. 27
In conclusion, this study found a rising trend of NPS use in Hong Kong, which is associated with considerable morbidity and mortality, highlighting its potential threat to public health. Harm reduction depends upon the vigilance of frontline clinicians and medical professionals in the lookout for suspicious drug history, clinical or laboratory findings, as well as the proactive and continual surveillance of NPS in the susceptible population.
Footnotes
Acknowledgements
All persons who made genuine contribution to the manuscript, including conception and design of study, data acquisition and analysis, drafting and critical reviewing of the contents, have been included in the author list. We have all approved the contents of the manuscript. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The authors approve the publication of all data and materials associated with the manuscript in the online version of the journal.
Ethical approval
This study has been approved by the Hospital Authority Kowloon West Cluster Research Ethics Committee on 20 September 2017 (KW/EX-17-110(114-11)).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Informed consent
Written informed consent was waived by the Ethics Committee because minimal patient data have been included in the manuscript and the risk of patient identification is very low.