
Abstract
Background:
In non-PCI capable hospitals, another important time to be noticed in patients who have been referred for PCI-capable centers; is the time of doo-in door-out (DIDO), defined as the duration of time from patient discharge from the transferrring hospital. In our country, there is no clear information about the duration of DIDO time and transfer time. Consequently, very little is known about how frequently these targets can be met nationally.
Objectives:
This study aimed to measure door-in door-out time for ST-elevation myocardial infarction diagnosed patients who admitted to emergency department of a hospital capable of non-percutaneous coronary intervention and to measure whether door-in door-out time meets the guidelines.
Methods:
This single-center, prospective study was conducted in emergency department (non-percutaneous coronary intervention capable) between 1 August 2015 and 1 August 2016 with patients who presented to the emergency department and were diagnosed with ST-segment elevation myocardial infarction. All the times including door-in time, door to electrocardiogram time, door to emergency medical services activation time, door to defined percutaneous coronary intervention hospital, and finally door-in door-out time were measured and recorded.
Results:
During the study period, 135 of patients met the inclusion criteria and diagnosed with ST-elevation myocardial infarction and referred to another hospital for percutaneous coronary intervention. When the median values (interquartile range of 25%–75%) of the time periods are examined, it is found door-in door-out time was 55 (43–74) min. It was found that the number of patients meeting the recommended duration of door-in door-out (30 min or less) was 12 (8.9%). Of the remaining 123 patients (91.1%), door-in door-out times were found to be over 30 min.
Conclusion:
In conclusion, our study showed that compliance with door-in door-out time is very poor and is far behind to met the criteria which is recommended by current guidelines.
Introduction
Coronary artery disease (CAD) is one of the most important causes of mortality and morbidity in both Turkey and the world. According to data from the Turkish Statistical Institute, in 2014, 40.4% of all deaths originated from circulatory system diseases and 39.6% of circulatory system diseases originated from ischemic heart disease. 1 Mortality due to acute coronary syndrome (ACS) causes approximately 95,000 deaths per year, which corresponds to an annual mortality rate of 32%, quite high when compared to the rates in Europe. 2 Therefore, particular emphasis should be given to the CAD diagnosis, and treatment should be initiated as soon as the first medical contact.
The primary treatment options for reperfusion strategy in patients with ST-elevation myocardial infarction (STEMI) are primary percutaneous coronary intervention (PCI) and fibrinolytic administration. In addition, early PCI treatment improves outcomes, including mortality. 3 Therefore, the current guidelines recommend PCI as a primary reperfusion strategy. Fibrinolytic administration is also recommended for the patient group who cannot perform PCI in a timely manner. In PCI-capable centers, it is recommended to perform PCI within first 90 min after diagnosis of STEMI.4,5 In centers which do not have PCI capability, it is recommended to transfer patients with STEMI to PCI-capable hospitals, and the primary PCI should be performed within at least 120 min.6,7 If this time prolonged, it is recommended to deliver fibrinolytic therapy—unless contraindicated—within the first 30 min.8,9
In non-PCI-capable hospitals, another important time for patients who have been referred for PCI-capable centers is door-in door-out (DIDO) time, defined as the duration from the patient’s arrival to patient discharge time from the transferring hospital. In the 2014 edition of the Myocardial Revascularization Guide, published by the European Society of Cardiology (ESC) and also in the 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation, it is specified that DIDO time should not exceed 30 min. In cases where this condition cannot be achieved, the guidelines recommend that fibrinolytic therapy should be initiated. 3 Furthermore, the current guidelines recommend intermittent measurements to improve duration of these times.10,11 In our country, there is no clear information about the duration of DIDO time and transfer time. Consequently, very little is known about how frequently these targets can be met nationally.
Therefore, with this study, we aimed to measure DIDO time for STEMI diagnosed patients who were admitted to the emergency department (ED) of a non-PCI-capable hospital and to measure whether DIDO time meet the guidelines. We also aimed to find the factors that influence this time.
Material and method
Study design and settings
This was a single-center, prospective, observational study conducted in the ED of a training and research hospital (non-PCI capable) between 1 August 2015 and 1 August 2016 with patients who presented to the ED and were diagnosed with STEMI. All participants provided written informed consent, and the study was approved by the local ethics committee.
Study population
Patients older than 18 years who were diagnosed with STEMI and were subsequently transferred into PCI facility for further treatment were included in the study. Patients who were younger than 18 years and who did not agree to participate in the study were excluded.
Data collection and definition
Demographic data, medical history, cardiac histories, the nature of the symptoms and the onset time, vital signs at arrival time and electrocardiogram (ECG) features, presence of cardiac insufficiency or cardiogenic shock findings at admission, and types of treatment applied to the patient were recorded in the patient’s form.
All the times to be measured in the study were recorded in the study form. The arrival time (door-in time) of the patients to emergency services was recorded, based on the time they registered. The ECG timing (door to ECG time) was recorded, based on the time of the ED doctor’s requesting the first ECG after the examination. In this case, the ED physician activates the emergency medical services (EMS: 112) to inform that a STEMI patient needs to transfer to another hospital for PCI. The reaching time (door to EMS activation time) to EMS for referral to PCI center was recorded. EMS system found the PCI-capable hospital to transfer patient and the determination time (door to defined PCI hospital) of the PCI center was recorded. Finally, the ground EMS ambulance took the patients from the first hospital and the departure time of the patient from ED (door-out time) was recorded in the patient’s form.
Several titles were defined using the time information and identified as the cause of delay. According to this, four reasons for delay in DIDO time were identified:
Late ECG timing—timing more than 10 min from admission to ECG recording time;
Late EMS activation—timing more than 10 min from diagnosed STEMI by ECG recording to reaching the EMS control center to give information about STEMI patients who need to transfer to another hospital for PCI;
Late determination time—timing more than 10 min from reaching EMS control centre to determination of PCI-capable hospital;
Delay of ambulance—timing more than 10 min from determination of PCI-capable hospital to EMS arrival to ED for taking and transferring patients.
Also, in some patients, the duration of the DIDO was prolonged because the first ECG was normal, or the posterior/right ECG was not taken, or the physician misinterpreted the ECG, and therefore, “delayed diagnosis” was identified as the fifth cause of delay.
Outcomes
The primary outcome was defined as measuring the duration of the DIDO time, measured at the patient level as the time from arrival in the ED to discharge from the same ED for patients who were transferred to another hospital for primary PCI. The secondary outcome was defined as investigating the factors associated with this time.
Statistical analysis
Statistical analyses were performed using SPSS version 16.0 (Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normal distribution of all parameters related to patients. Patients’ parametric data were expressed as mean values and standard deviation (SD). Non-parametric data were expressed as median values and interquartile range (IQR) (25%–75%). The Pearson Chi-Square test was used to analyze the groups’ categorical data. Continuous parametric group data were analyzed using the Student t-test, and non-parametric group data were analyzed using the Mann–Whitney U and Kruskal–Wallis tests. The 95% confidence intervals (95% CIs) were calculated whenever appropriate, and a two-tailed p-value < 0.05 was considered statistically significant.
Results
During the study period, 135 patients met the inclusion criteria, were diagnosed with STEMI, and referred to another hospital for PCI. The general characteristics of the patients are summarized in Table 1.
General characteristics of patients.
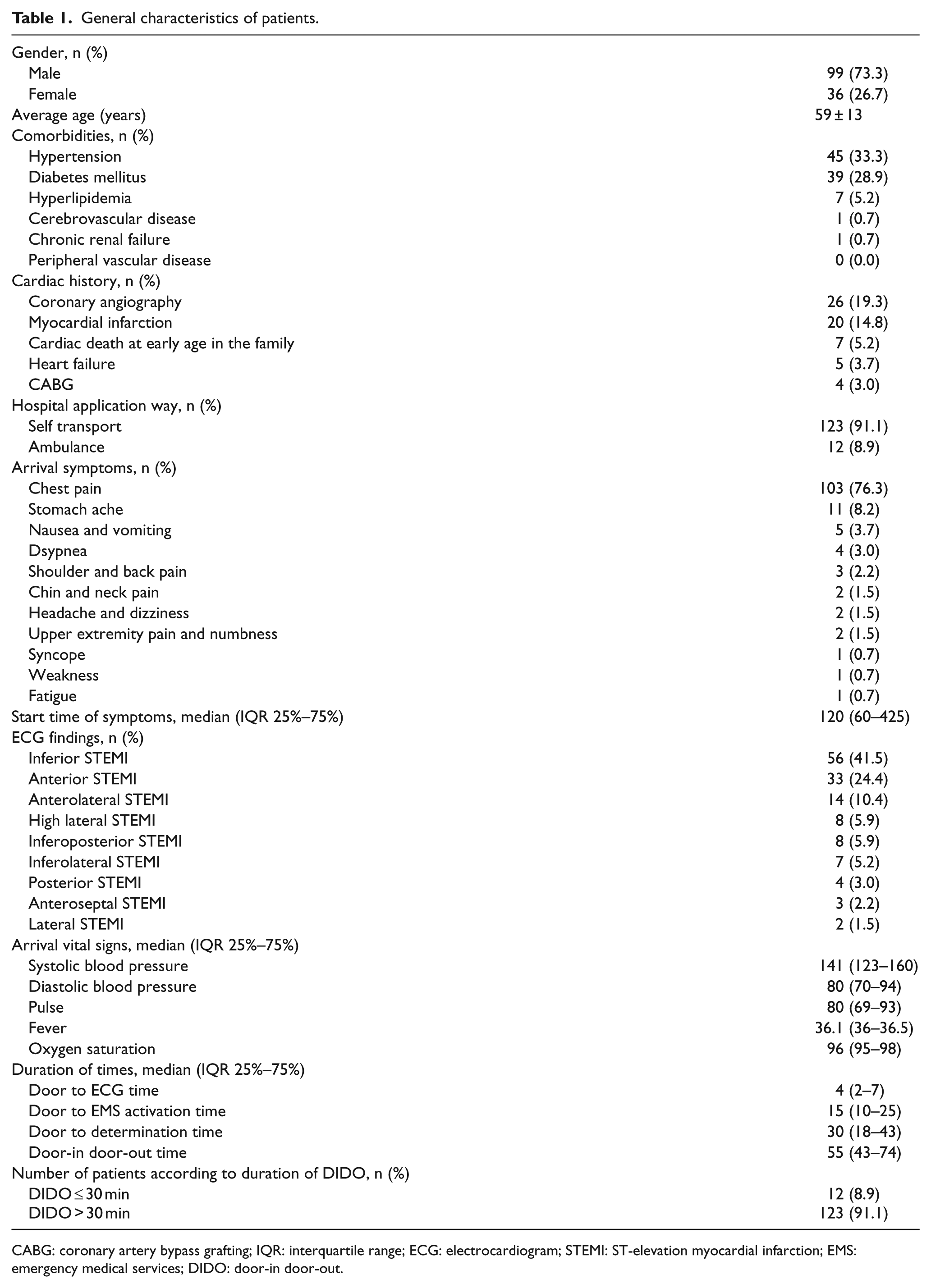
CABG: coronary artery bypass grafting; IQR: interquartile range; ECG: electrocardiogram; STEMI: ST-elevation myocardial infarction; EMS: emergency medical services; DIDO: door-in door-out.
When the median values (IQR 25%–75%) of the time periods are examined, the results are as follows: the duration of door to ECG time was 4 (2–7) min, door to EMS activation time was 15 (10–25) min, door to defined PCI hospital time was 30 (18–43) min, and finally, DIDO time was 55 (43–74) min. It was found that the number of patients meeting the recommended duration of DIDO (30 min or less) was 12 (8.9%). Of the remaining 123 patients (91.1%), DIDO times were found to be over 30 min (Figure 1).
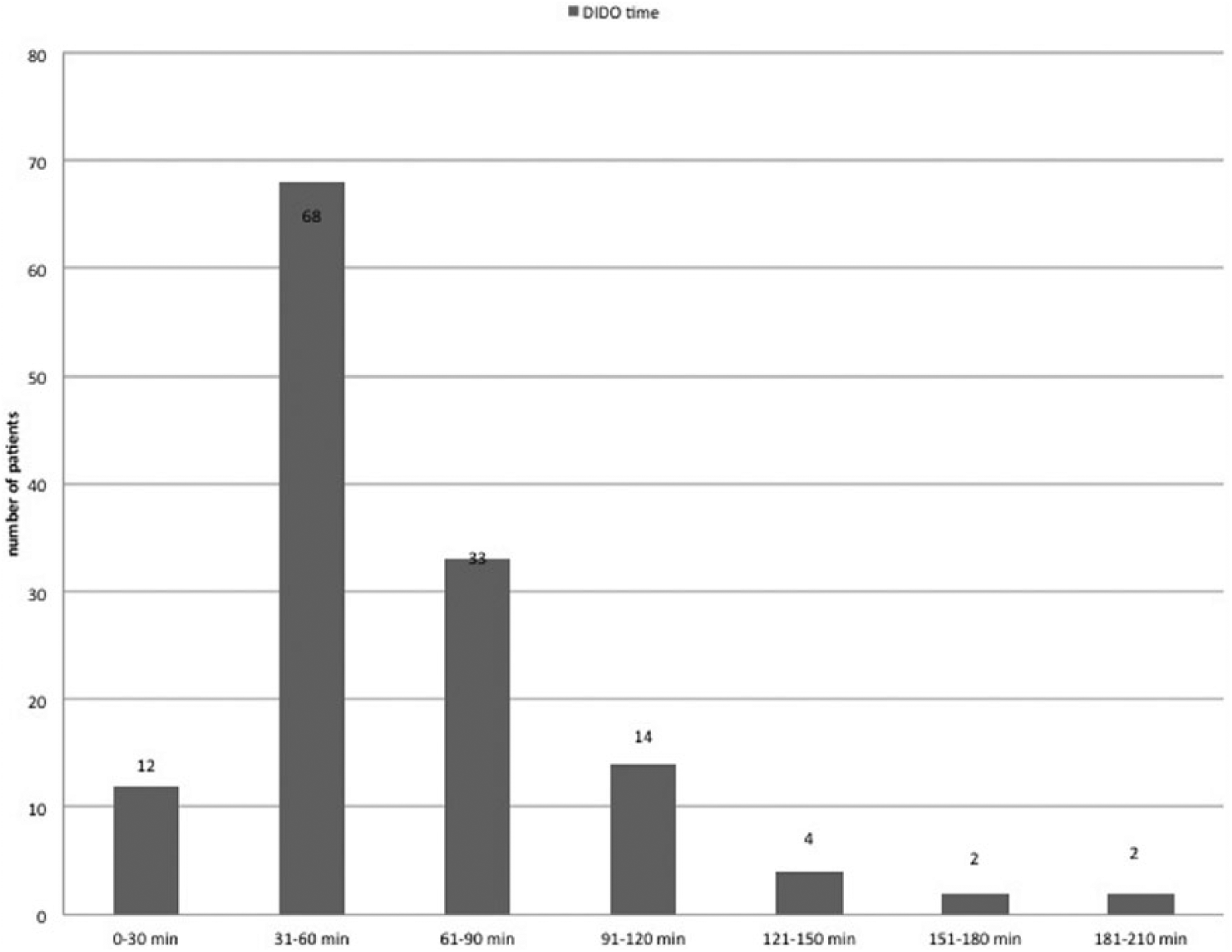
Number of patients according to DIDO time.
Five titles, previously defined according to the protocol, have been established as the cause of the delay in patients who have longer durations of DIDO time than the guidelines recommended (Figure 2). The most common cause of prolongation in DIDO time was ambulance delay (46%).
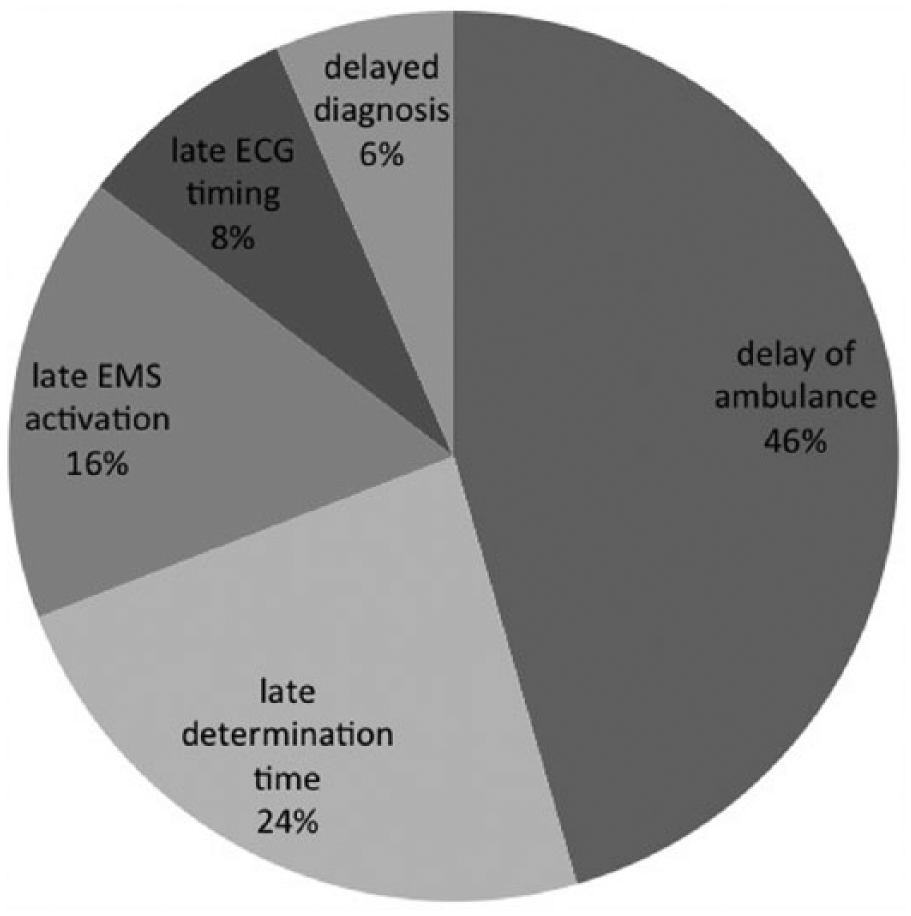
Number of patients and percentages according to reasons for delay.
Four-hour intervals were set up to determine whether the durations of time changed at certain times of the day, and the duration of the patients admitted at these times was compared by considering the arrival times of the patients (Table 2). According to this, the shortest duration of times was determined between 4:00 a.m. and 8:00 a.m. However, it was seen that only one of the titles which was “door to EMS activation time” was statistically significant.
Duration of times according to time zones (min).
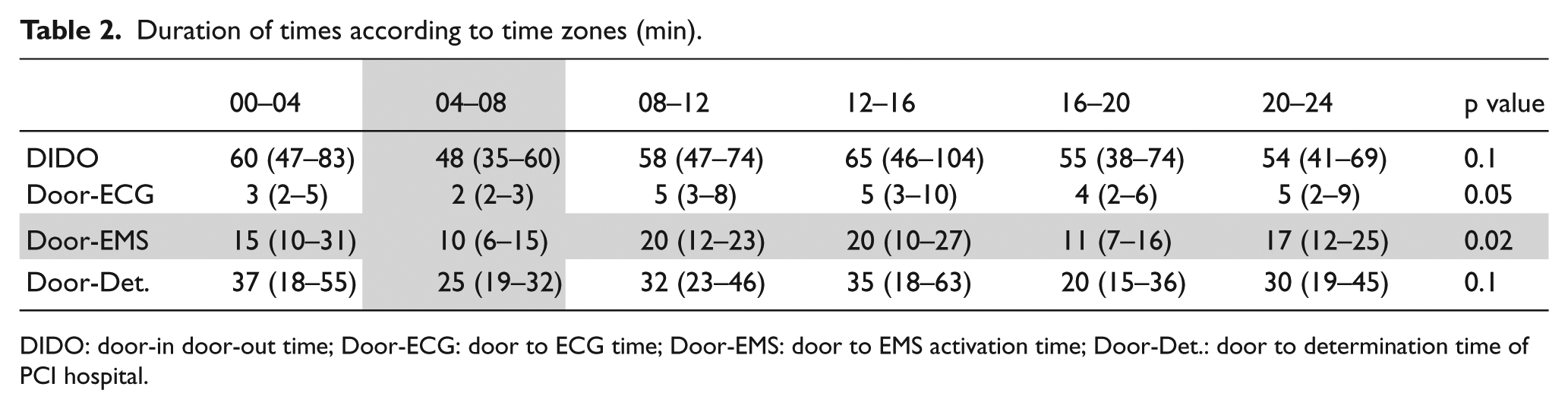
DIDO: door-in door-out time; Door-ECG: door to ECG time; Door-EMS: door to EMS activation time; Door-Det.: door to determination time of PCI hospital.
Possible causal parameters affecting the time of DIDO were evaluated to see if there was a relationship between them. According to this, 9 (75%) of the patients with 30 min or less duration of DIDO time applied to the hospital with their own resources and 3 (25%) of the patients with 30 min or less duration of DIDO time applied to the hospital by ambulance, while 114 (92.7%) of patients with over 30 min duration of DIDO time applied to the hospital with own resources and 9 (7.3%) of patients with over 30 min duration of DIDO time applied to the hospital by ambulance. A statistically significant difference was found between the two groups in terms of manner of admission to the hospital (p = 0.04). However, in the univariate regression analysis performed, it was found that the duration of DIDO time was not significant in determining whether to be over 30 min or less (p = 0.055, odds ratio: 4.2, 95% CI: 0.9–18). In addition, when the other parameters were examined, no statistical difference was found (Table 3).
Characteristics of patients according to durations of DIDO time.
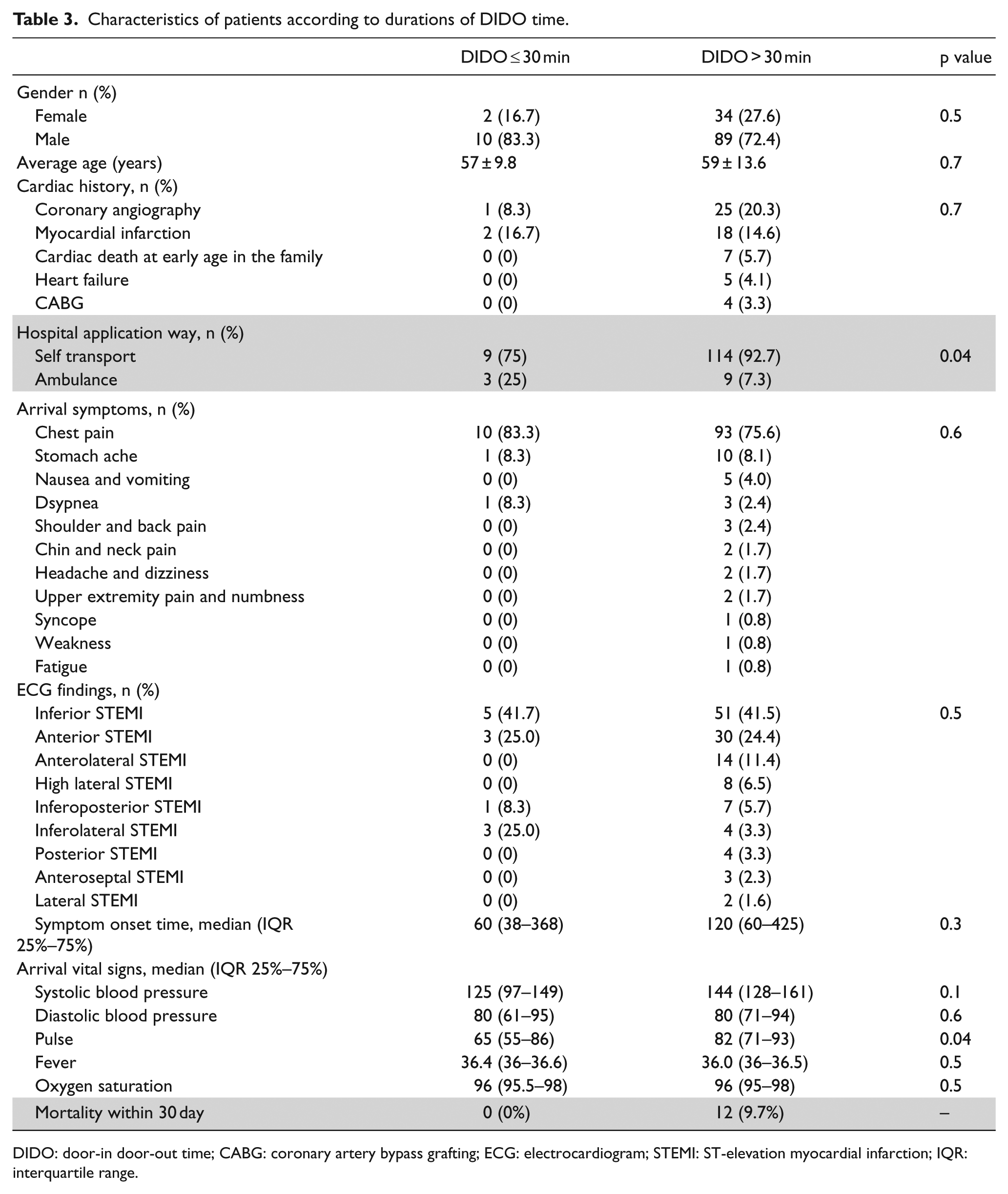
DIDO: door-in door-out time; CABG: coronary artery bypass grafting; ECG: electrocardiogram; STEMI: ST-elevation myocardial infarction; IQR: interquartile range.
Furthermore, no deaths were observed in patients with 30 min or less duration of DIDO time within first 30 days; however, 12 (9.7%) deaths were observed in patients with over 30 min duration of DIDO time (Table 3).
Discussion
Today, we know that PCI is more effective and more preferred than fibrinolytic treatment as a reperfusion strategy in STEMI patients if it is performed within several time targets. Although the best of known these time targets is “door-needle time” among the physicians, another time target, which is not often taken into consideration, is DIDO time for non-PCI-capable hospital when given a transfer decision to another PCI-capable hospital. Therefore, current guidelines recommend that DIDO times are measured and improved all over the country. As a result, in this study, aiming to measure DIDO times, there are four important results. First of all, we found that the rate of meeting the recommended duration of DIDO time was very poor. Compliance rates to the DIDO time target were below 10%. The second important result is the findings about the causes of this prolongation. According to our results, the cause of prolongation of DIDO time of almost half of the cases (46%) was delay of the ambulance performing the transfer of the patient to PCI-capable center. The third important result is the ambulance admission rate of the patients who met DIDO time was higher than the patients with which it could not be met. In our opinion, the most important reason for this is the patient is transfer to PCI-capable center with the same ambulance without waiting for another one just after the ECG was taken. However, in a univariate regression analysis, we noticed that applying by ambulance was not significant in predicting the DIDO time (p = 0.055, odds ratio: 4.2%95% CI: 0.9–18.4). Nevertheless, when we consider that only 12 out of 135 STEMI patients are admitted to hospital by ambulance, we think that it is not possible to make general conclusions on this issue. As a reason of a significant delay in the DIDO time, another headline was determined as EMS system could not immediately find a PCI-capable hospital where the patient could be transferred to (24% of all cases). Finally, the fourth important result is, when the time of the day was taken into account, all durations, including the DIDO time, are considered to be the shortest between 04:00 and 08:00. However, a statistical significance was only found in connection with the door to EMS activation time.
Although current guidelines recommend that DIDO times be measured at regular intervals, the number of studies about DIDO times is limited. For example, in an important study conducted by Wang et al. with 14,821 STEMI patients who were transferred to PCI-capable centers from non-PCI capacity centers, it has been found that the median duration of DIDO time of patients was 68 min (IQR 43–120 min) and only 1627 patients (11%) met the criteria for DIDO time. In addition, the study found that 56% of patients’ duration of DIDO time was over 60 min and 35% patients’ duration of DIDO time was over 90 min. The authors reported that significant factors associated with patient’s DIDO time exceeding 30 min included older age, female gender, presenting during off-working hours, and admission to the first hospital with non–EMS transportation. It has also been observed that there is a progress in the percentage of patients who met the DIDO time. The median duration of DIDO time was 90 min (IQR 55–180 min) in January 2007, while the median duration of DIDO time was 58 min (IQR 38–103 min) in March 2010. Door-to-balloon (DTB) times were calculated and compared in both groups, whether they met the criteria for DIDO time or not. The median duration of DTB time in patients who met DIDO time was 85 min, while the median duration of DTB time in patients did not meet DIDO time was 127 min (p < 0.001). In comparison, DTB time (120 min or less) recommended in the guidelines, 91% of the patients with DIDO duration was 30 min or less and 43% of the patients with DIDO duration was over 30 min whose met the criteria and the difference was significant (p < 0.001). Observed in-hospital mortality was significantly higher among patients with DIDO times over 30 min compared to patients with DIDO times of 30 min or less (5.9% and 2.7%, p < 0.001). 11 And finally, when the authors evaluated various variables in terms of predicting prolongation of DIDO time, they identified the ambulance referral as an effective parameter of meeting a DIDO time target similar with our results. However, in our univariate regression analysis, the odds ratio value for applied to hospital by the ambulance was insignificant, while Wang and colleagues found in their study, which has a much larger sampling, that the odds ratio for applied to hospital by the ambulance was 1.26 (95% CI: 1.08–1.4) found significant.
Another retrospective observational study was conducted by Lambert et al. with 988 STEMI patients who were transferred from non-PCI-capable hospitals to PCI-capable hospitals for primary PCI. The authors reported that the median duration of DIDO time of 988 patients was 51 min (IQR 35–82 min) and only 139 patients’ (14.1%) DIDO time was 30 min or less. In addition, factors associated with longer DIDO time were found as female sex, more comorbidities, longer symptom duration, presenting during working hours, arriving at a center with a low STEMI volume, and admitting to the first hospital with non-EMS transport. 12
In another retrospective observational study by Herrin et al., they included 13,776 patients with STEMI from 1034 non-PCI-capable centers. Similar to previous studies and our study results, the median of the duration of DIDO time was measured 64 min (IQR 43–104 min). Only 1343 (9.7%) patients had a DIDO time of 30 min or less. The factors associated with patient’s DIDO time exceeding 30 min were found as older age, female gender, and patients with contraindication to fibrinolytic therapy. In patients with no contraindication to fibrinolytic therapy, it was found 75% of them had a DIDO time of over 43 min and 25% of them had a DIDO time of over 110 min. 10
In another study, Harjai and colleagues examined the duration of DIDO time in 193 patients with STEMI who were transferred for PCI from a non-PCI capacity center and the mean of DIDO was found 80 ± 42 min. Also, according to the authors, they found that the most important delay in DTB time was caused by this DIDO delay. 13
To summarize, the results of all these studies, which have large study populations, and our study showed that most of the patients could not met the criteria of DIDO time and it is a significant problem all over the world in STEMI management. Although each country has different reasons for these delays, it seems reasonable that the common variable cause of prolonging the DIDO time was associated with EMS transportation delays.
We believe that the first step in solving a problem is to recognize that it does exist. The current guidelines recommend that these times should be measured at regular intervals and studies should be done to improve the causes of possible delays. As a good example of this suggestion, Glickman et al. evaluated 436 patients with STEMI in non-PCI capacity hospital. As part of the national regionalization program (RACE, Reperfusion of Acute Myocardial Infarction in North Carolina Emergency Departments), standard protocols for STEMI patients were implemented for 1 year and emergency health system, emergency service, and hospital related regulations were made. Then, the DIDO times were analyzed both before and after these regulations. A significant improvement in median of the DIDO time was observed after this program (median of the DIDO time was 97 min (IQR 56–160 min) before regulations and 58 min (IQR 35–90 min) after regulations). 14 To our knowledge, our study is the first to measure the duration of DIDO time in the regional sense and to reveal the possible causes of delay. In this sense, we believe that similar measures should be repeated by making similar regional improvement arrangements like those presented by Glickman and his colleagues.
We think that the delay due to the arrival time of ambulances transferring patients to PCI-capable centers is the most effective on duration of DIDO time. Indeed, our study showed that in 46% of patients who cannot meet the DIDO time, the cause was ambulance-related delays. As ambulance-related delays are influenced by many factors, such as location of the hospital, traffic flow in the region, whether the paramedic team is close to hospital or not, and whether the paramedic team is appropriate at that time or not, it is the most important issue need to focus on. In our country, EMS system call center (112) is not sought only for emergency patients; therefore, real emergency patients’ needs cannot be met on time. Although the number of people per ambulances has declined over the years (32,466 in 2009, 14,899 in 2016),15,16 patients with low levels of urgency are more likely to use ambulances, which often causes force the capacity of EMS. Another important result—supporting unnecessary EMS using—is that in our study, we found that DIDO time was shortest and also the numbers of patients who met the criteria for DIDO time was increased during the 04:00–08:00 compared to rest of the day. On the contrary, during working hours, such as 08:00–12:00 and 12:00–16:00, the rate of patients who met the criteria for DIDO time decreased. In studies conducted in other countries, DIDO time of STEMI patients was found to be shorter during the working hours of the daytime.11,12 We think the reason for this difference is that ambulance services in our country are mostly used for non- or less-urgent situations during working hours. Especially after midnight, both the EMS centers and ambulance services are only used for truly urgent cases, and the delays experienced during these times may be diminished.
Limitations
One of the most important limitations of our study are the parameters such as the time of arrival at the hospital, the length of stay in the hospital, and mortality of the patients whom transferred to another hospital were not followed up. Thus, DTB time could not be measured in our study. Data were collected from only one center during the study, and for this reason, no comparison can be made between hospitals in different regions. In addition, we believe that there might be several factors which contributed to delay DIDO time excluding our main reasons for delays. However, in our study, we aimed to focus on possible reasons of delayed DIDO time–related EMS systems.
Conclusion
In conclusion, our study showed that compliance with DIDO time is very poor and is far behind in meeting the criteria recommended by current guidelines. The most important parameter that causes this delay is the fact that the ambulance, which will perform the transfer, cannot reach the emergency service at the appropriate time. Although there is a need for different studies to define the reasons for delay in the ambulances, we believe that most ambulance-related delays in DIDO time occur due to the use of EMS system in non-urgent or low emergency potential situations. In addition, our study shows that applying to the hospital with an ambulance caused a significant shortening in of the DIDO time. In order to prevent ambulance-related delays and to raise awareness, community-oriented training programs should be established.
We believe that after the relevant regulations have been made, it is necessary to repeat the control studies at regular intervals to determine whether the current durations have been improved.
Footnotes
Acknowledgements
Ş.K.Ç. and I.D. conceived and designed the experiments; I.D., E.E., and H.A. performed the experiments; Ş.K.Ç., Y.Ç., and E.E. analyzed and interpreted the data; Ş.K.Ç., H.A., and Y.Ç. contributed reagents, materials, analysis tools, or data; Ş.K.Ç. and I.D. wrote the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
If the SPSS record is needed, it can be availed.
Informed consent
The patient informed consent was signed by all participations.
Ethical approval
The local ethics committee approved this study.
Human rights
During the study period, the research was conducted in accordance with the tenets of the Helsinki Declaration and Human Rights.