
Abstract
Haemopericardium with cardiac tamponade following minor blunt trauma is a rare, life-threatening condition. The diagnosis of cardiac tamponade as well as therapeutic management may be delayed, since the link between trauma and illness is often overlooked. We report the case of an old woman who developed a relatively delayed cardiac tamponade due to an otherwise minor blunt chest trauma following syncope.
Introduction
Cardiac tamponade is a life-threatening condition characterized by compression of the heart caused by a slow or rapid accumulation of liquid, pus, blood, clots or gas in the pericardium. These are usually secondary to inflammation, trauma, rupture of the heart or aortic dissection.1–3
Haemopericardium with cardiac tamponade following minor blunt trauma is a rare and challenging condition for any physicians working in emergency units. 4 Clinical sequelae from blunt cardiac trauma may range from minor electrocardiographic abnormalities to death due to free-wall rupture; 5 however, concomitant comorbid conditions of patients could play a major contributory role and should be carefully considered.
Case report
An 87-year-old woman was admitted to the Emergency Department because she fell to the ground due to a likely syncopal episode. As a result of the trauma, the patient had a contusion of the left part of the chest in the absence of radiologically evident rib fractures. Chest and hemithorax X-ray as well as abdominal ultrasound were unremarkable. Her clinical history evaluation disclosed multiple comorbidities such as hypertension (treated with angiotensin-converting enzyme inhibitors and diuretics), paroxysmal atrial fibrillation in oral anticoagulant therapy (warfarin), New York Heart Association (NYHA) class II heart failure, chronic kidney disease and chronic vascular encephalopathy with mild cognitive impairment.
At the time of the first visit, the patient appeared awake, collaborating although confused. The thoraco-abdominal physical examination as well as thorough neurological evaluation did not show significant alterations or acute deficits (in particular she did not present any chest wall tenderness or bruises). Vital parameters were normal, blood pressure 120/70 mmHg, heart rate 75 beats per minute and oxygen saturation was optimal (96%). Blood chemistry tests confirmed stable renal dysfunction, international normalized ratio (INR) coagulation test was in the therapeutic range for warfarin treatment and D-dimer index was within the normal one. The following morning, the patient’s clinical conditions rapidly worsened with the appearance of dyspnoea, arterial hypotension and loss of consciousness. High-flow O2 was administered with a slight improvement in the respiratory panel and electrocardiogram revealed atrial tachyfibrillation with a mean frequency of 150 bpm along with the evidence of low voltages in all leads (Figure 1). A trans-thoracic bedside echocardiography was performed and this test documented a significant pericardial effusion (with apparently corpuscular fluid) mainly located at the right atrium level, with atrial wall compression, and resultant acute cardiac tamponade (Figure 2). The clinical picture worsened rapidly, thus preventing any further therapeutic procedures also considering the will of the patient’s relatives who denied a pericardiocentesis measure. Finally, the patient died due to the significant haemodynamic failure related to the cardiac (likely haemorrhagic) tamponade.
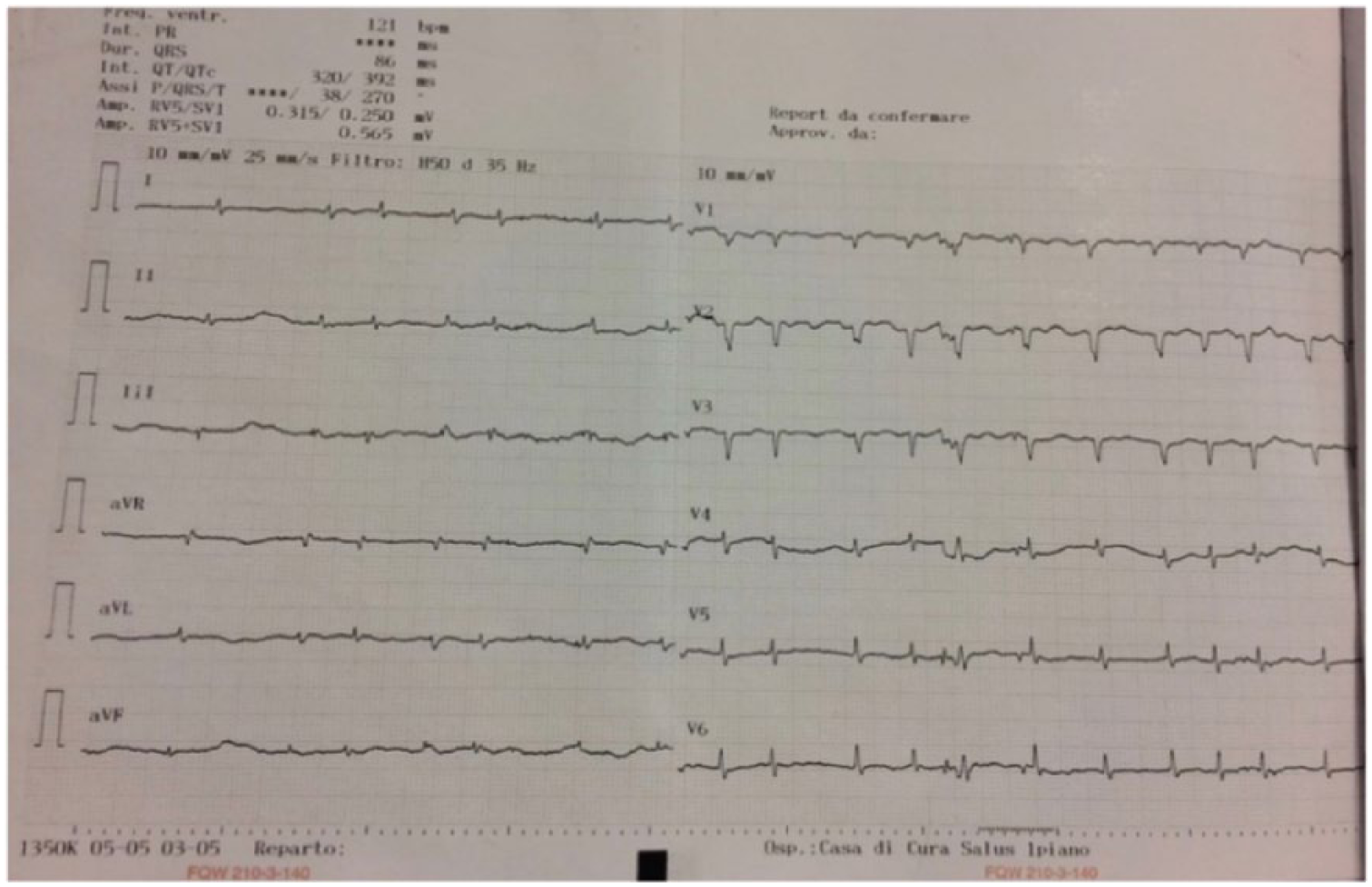
Representative ECG showing the low voltage in all leads and electric alternations suggestive of cardiac tamponade.
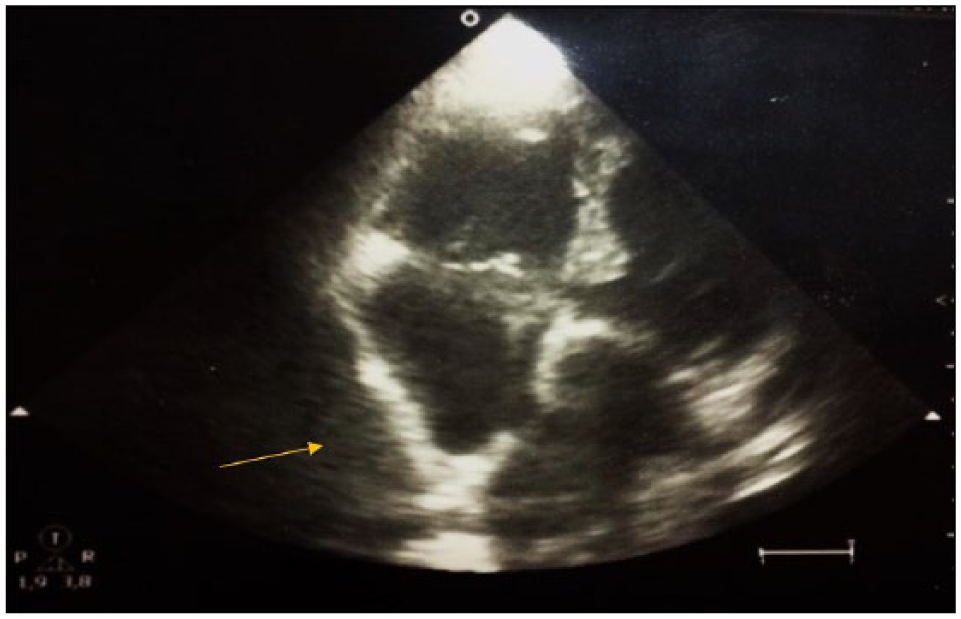
Bedside echocardiography picture showing accumulation of fluids (arrow) in the pericardial area indicative of cardiac tamponade.
Discussion
Cardiac tamponade results from an accumulation of pericardial fluid increasing the pressure around the heart, leading to impaired cardiac filling and haemodynamic abnormalities. 2 Beck’s triad, that is, sinus tachycardia, elevated jugular venous pressure and low arterial blood pressure, along with pulsus paradoxus, represents the main clinical features suggesting the occurrence of such life-threatening condition. Although mainly clinical, the diagnosis of cardiac tamponade should be confirmed by a number of tests including electrocardiogram, chest X-ray, echocardiography and/or more accurate imaging techniques.1,2 A recent randomized trial has shown that the use of transthoracic echocardiography improves the timing of the hospital admission of traumatized patients and their transfer to the operating room, thus resulting in a reduced mortality rate.1,6 This case suggests that bedside echocardiography should be used to unravel complications caused by minor chest traumas in elderly patients with various comorbidities and under polypharmacological treatment.7,8 The treatment of cardiac tamponade is aimed to sustain circulation and decompress the pericardial area by removing the accumulated fluids. This helps relieving pressure surrounding the heart and restore cardiac pump function leading to haemodynamic improvement. 8 The rapid worsening of clinical conditions, the advanced age and comorbidities without putting aside the ongoing effect of warfarin treatment were all arguments to the detriment for invasive decompression of pericardium in our patient.
Blunt chest trauma may cause cardiac damage varying from minor contusion up to major complications, such as cardiac tamponade. 9 Clearly, this latter event is expected with major traumas, as the high intensity of impact generates serious damage to the heart that can lead to the development of effusion or even the breaking of the ventricular wall. However, although to a lesser extent, even minor traumas may determine cardiac tamponade as indicated by this and other 11 cases4,9,10–19 that have been summarized in Table 1. Notably, there is no direct timing correlation between the traumatic event and cardiac tamponade, that is, the latter occurring from few hours up to months (Table 1).
Other cases that correlate minor trauma to pericardial tamponade.
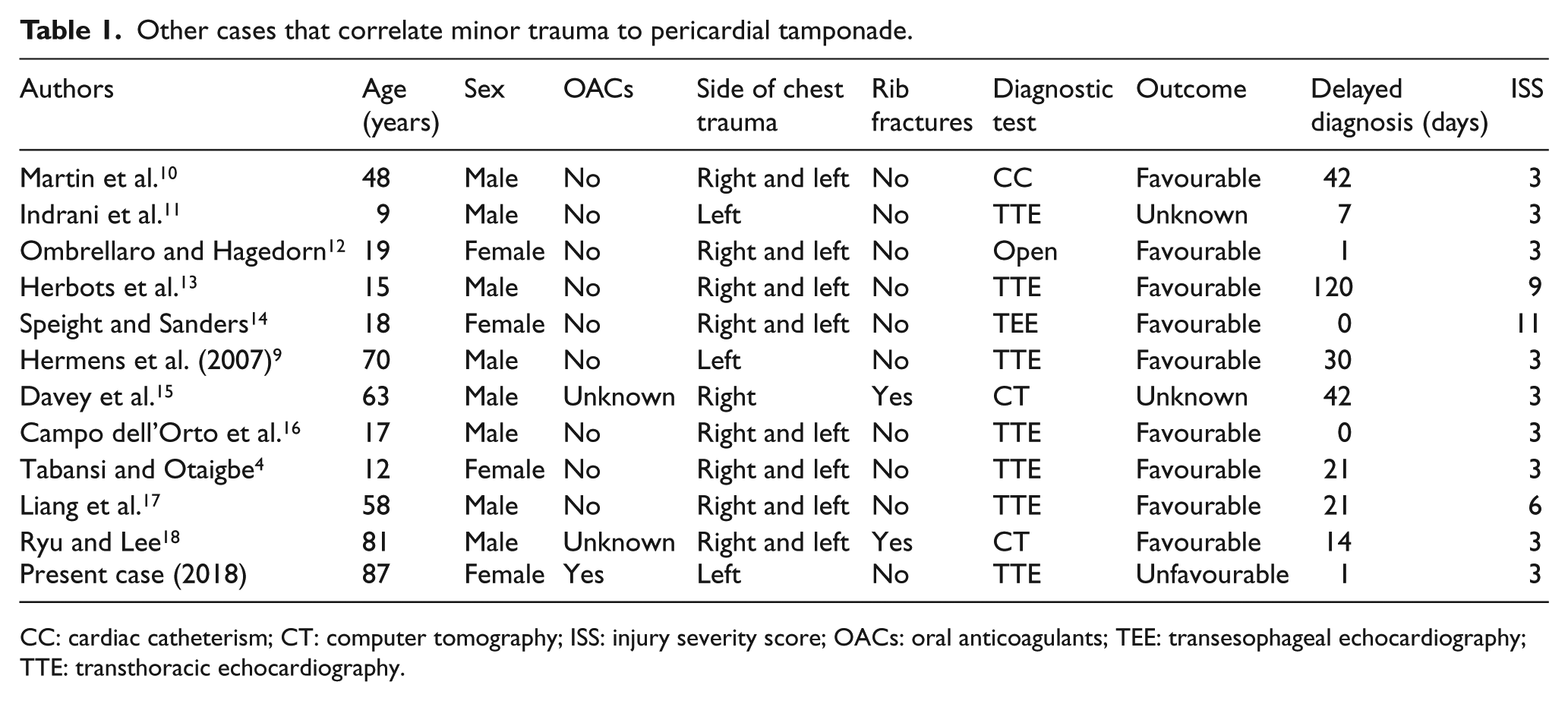
CC: cardiac catheterism; CT: computer tomography; ISS: injury severity score; OACs: oral anticoagulants; TEE: transesophageal echocardiography; TTE: transthoracic echocardiography.
This case highlights that a clear distinction about major and minor traumas is difficult to be established, particularly in the emergency setting. Many protocols have been developed in order to identify and treat properly major traumas of the chest. In our case we used the injury severity score (ISS), which measures traumatic events and if the score is more than 15 it indicates a major trauma. 19
In addition to the trauma score, another important factor to be considered is that the elderly population is gradually growing alongside with the co-occurrence of comorbidities. Ageing, multi-morbidities and poly-therapy (including anticoagulants and antiplatelet drugs) are three major risk factors for the development of serious complications. Indeed, our case showed that a minor chest trauma caused a life-threatening condition, that is, cardiac tamponade, in a patient with multi-morbidities and under warfarin treatment.
Conclusion
The experience gained with this case suggests that regardless the intensity of the trauma, any chest injury should require a thorough clinical and instrumental (i.e. beginning with bedside echocardiography) evaluation to timely detect cardiac tamponade. Frail, elderly patients taking anticoagulant or antiplatelet compounds 6 are at risk for such life-threatening complication even if the traumatic injury occurred is mild.
Footnotes
Acknowledgements
The authors thank Dr Donato Bragatto, Dr Claudia Righini, Mrs Manuela Zappaterra (Biblioteca Interaziendale di Scienza della Salute, Hospital of Ferrara), Mrs Egizia Zironi and Mrs Silvia Bellotti (Unità Servizi Interbibliotecari, University of Ferrara) for their valuable collaboration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Human rights
All procedures performed on the reported patients were conducted in accordance with good clinical practice respectful of any human rights.
Informed consent
Since the report did not show any identification with the patient involved, there was no need for ethics committee approval. Nonetheless, all procedures on the reported patient were subjected to informed consent.