
Abstract
Introduction
A spinal epidural abscess (SEA) is a rare, potentially devastating pyogenic infection located between the spinal dura mater and vertebral periosteum. 1 It can be challenging to diagnose and has often evaded timely diagnosis, with up to 75% of cases misdiagnosed at the initial healthcare encounter.2–4 The incidence of SEA is increasing from 1975 to 1998; the incidence increased from 0.2–1.2 to 2.5–3.0 cases per 10,000 hospital admissions. 5 One reason for this is the rising number of invasive cervical procedures, such as acupuncture, tattooing, epidural analgesia, and nerve block.6,7
Cervical spondylosis is the most common type of spinal pathology, observed most commonly in middle-aged or older populations; it can often affect physical and mental health. 8 Patients with cervical spondylosis frequently present with chronic neck pain. In East Asia, many people seek Chinese medicine and folk remedies for the treatment of physical pain, such as moxibustion, acupuncture, and wet cupping. 9 Needle-knife acupotomy therapy, a treatment method similar to acupuncture but using specially designed needle-scalpels, is considered by some doctors to be more effective for neck stiffness and pain relief than traditional acupuncture-cupping, with a shorter treatment time.10–12 Although widely considered safe, needle-knife acupotomy, as with any invasive procedure, can cause infection, 9 and it is possible for superficial and subcutaneous tissue infection to spread to the spinal epidural space.
Case report
The patient was a 69-year-old woman with no history of diabetes mellitus or hypertension, who had suffered chronic neck pain for many years. Two weeks before admission, her daughter took her to receive needle-knife acupotomy for her neck pain, performed by a Traditional Chinese Medicine practitioner at a local clinic (Figures 1 and 2). The patient attended our emergency department because she had experienced gross hematuria for 1 week, with fever (38.1°C) and bilateral flank pain. The initial physical examination revealed bilateral mild costovertebral angle tenderness on percussion. All four limbs exhibited normal muscle power. The urine analysis revealed pyuria (white blood cell (WBC) count, 869/μL; bacteria, >4/HPF; nitrite, 2+; leukocyte esterase, 3+), and the blood analysis showed leukocytosis with left shifting (WBC, 21,200/μL; neutrophilic segment, 92.5%) and extreme elevation of high-sensitivity C-reactive protein (25.53 mg/dL). She was diagnosed with bilateral acute pyelonephritis and assigned for admission to the nephrology ward. However, 4 h later, she experienced the acute onset of weakness of both right limbs, with Medical Research Council (MRC) grade III/V power in her distal right upper limb myotomes (most weakness at the right finger flexors) and MRC grade IV/V power in her right lower limb myotomes. The neurologist confirmed right hemiparesis, with a positive Babinski sign on her right side, suggesting an acute ischemic stroke (a suspected pure motor lacunar infarction with a National Institutes of Health Stroke Scale score of 3). However, she did not have facial palsy or slurred speech; the brain computed tomography also showed negative findings.

Needle-knife acupotomy wounds on the posterior neck and back of our patient.

Instruments used to perform needle-knife acupotomy.
The patient was admitted to the neurology ward and administered levofloxacin 750 mg intravenous infusion per day for bilateral acute pyelonephritis. However, she experienced a spiking fever every day. After admission, she complained of progressive four limbs numbness, weakness, and urinary retention. And she experienced fullness and discomfort around the entire T6 dermatome. The neurologic examination showed positive Babinski signs bilaterally and decreased pinprick sensation in both her lower limbs. We suspected cervical and thoracic myelopathy. An emergency neck magnetic resonance imaging (MRI) with gadolinium contrast was arranged instead of the originally planned brain MRI. This showed an extensive cervical subcutaneous, intramuscular, and epidural abscess from C3 to T1 (Figure 3).
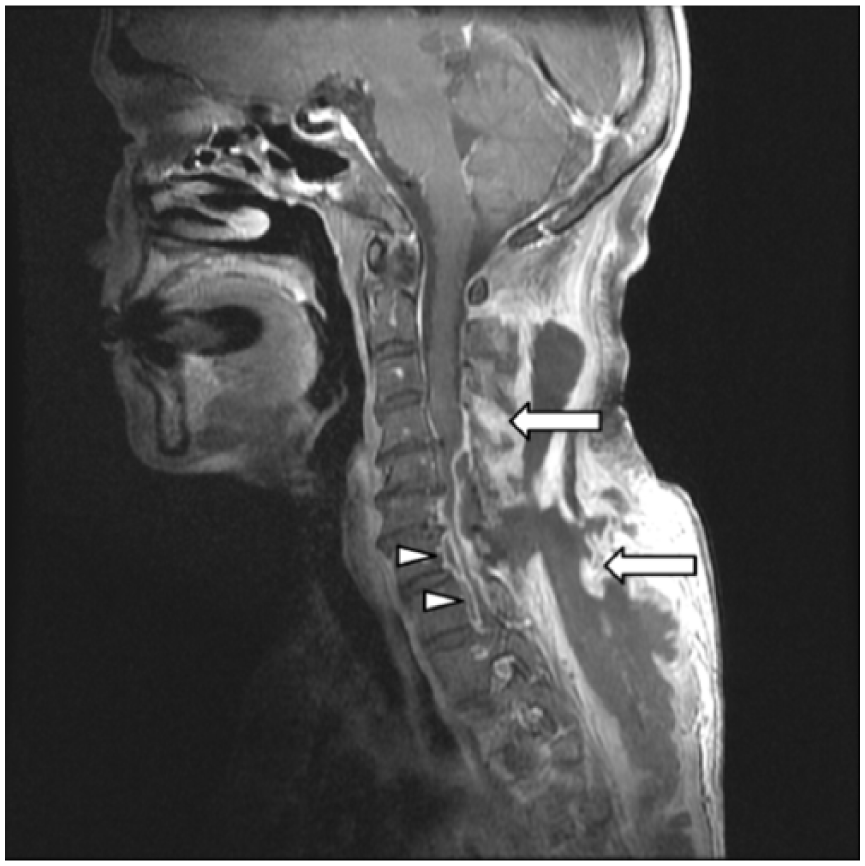
Cervical spine MRI. T1-weighted images with contrast showed an extensive multi-lobulated lesion in the subcutaneous and deep level of the bilateral posterior neck and back (arrows), and a thin collection of marginal enhancements in the anterior epidural region (arrowheads).
A C3-T1 laminectomy was performed by a neurosurgeon, and the residual abscess was debrided 11 days later. Her pain, numbness, weakness, and urinary retention improved gradually. The spinal deep pus retrieved during the operation was cultured, revealing methicillin-resistant Staphylococcus aureus (MRSA); this pathogen was also found in her previous blood and urine cultures. 56 days after the first operation, she was discharged with near total recovery.
Discussion
In this case, we were initially misled by the patient’s acute pyelonephritis and right hemiparesis. However, she had undergone an invasive procedure on her nuchal area and back; in such circumstances, spinal pathology such as a SEA and a hematoma should be taken into consideration,13,14 as these can mimic acute ischemic stroke. Because serial chest X-rays found no pneumonia, and echocardiography showed no valvular vegetations, it is reasonable to take into consideration that it was the needle-knife acupotomy that introduced the MRSA into her skin, where it entered to the subcutaneous area and invaded the epidural space, blood stream, and urine.
The most commonly isolated pathogen in the SEA was S. aureus, followed by Streptococcus. 15 On the third day of the patient’s admission, the blood and urine culture yielded MRSA; we therefore shifted the antibiotics from levofloxacin to vancomycin, which was maintained after the laminectomy and debridement.
The patient and her family told us that the doctor in the local clinic made the acupotomy needle-knife by himself (Figure 2), and that it was made of metal and was reusable rather than disposable. The doctor inserted the needle-knife into acupoints on the patient’s back and then separated the adhesion sites of the lesion. The myofascial release was confirmed by our neurosurgeon, who found a highly unusual loose space between the patient’s skin and muscle; much pus came out from this space when the neurosurgeon incised the patient’s skin. The cervical MRI also suggested myofascitis and an abscess (Figure 3).
Conclusion
A SEA is difficult to diagnosis, and it can sometimes mimic an acute ischemic stroke. This rare complication should be considered for patients who have undergone invasive cervical procedures. Needle-knife acupotomy is a more invasive procedure than the traditional acupuncture. Although it is considered safe and effective for cervical spondylosis, it can be complicated by spinal infection. Careful disinfection should therefore be performed, and disposable needle-knives should be used.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of the patient.
Ethical approval
The authors removed the identifying features of our patient in this case report. We also asked the patient herself for the publication and signed the inform consent (as above).
Informed consent
Written informed consent was obtained from patient herself for anonymized patient information to be published in this article.
Human rights
About the measures that have been taken to anonymize the details: not report the exact date and place, the photo only contain the patient’s upper back, no specific identifying features can find in the figures.