
Abstract
Background:
Delayed transfer of patients from the emergency department to the intensive care unit is associated with adverse clinical outcomes. Critically ill patients with delayed admission to the intensive care unit had higher in-hospital mortality and increased hospital length of stay.
Objectives:
We investigated the effects of an intensive care unit admission protocol controlled by intensivists on the emergency department length of stay among critically ill patients.
Methods:
We designed the intensive care unit admission protocol to reduce the emergency department length of stay in critically ill patients. Full-time intensivists determined intensive care unit admission priorities based on the severity of illness. Data were gathered from patients who were admitted from the emergency department to the intensive care unit between 1 April 2016 and 30 November 2016. We retrospectively analyzed the clinical data and compared the emergency department length of stay between patients admitted from the emergency department to the intensive care unit before and after intervention.
Results:
We included 292 patients, 120 and 172 were admitted before and after application of the intensive care unit admission protocol, respectively. The demographic characteristics did not differ significantly between the groups. After intervention, the overall emergency department length of stay decreased significantly from 1045.5 (425.3–1665.3) min to 392.0 (279.3–686.8) min (p < 0.001). Intensive care unit length of stay also significantly decreased from 6.0 (4.0–11.8) days to 5.0 (3.0–10.0) days (p = 0.015).
Conclusion:
Our findings suggest that introduction of the intensive care unit admission protocol controlled by intensivists successfully decreased the emergency department length of stay and intensive care unit length of stay among critically ill patients at our institution.
Introduction
Prompt diagnosis and treatment are crucial for critically ill patients.1–3 Previous studies showed that early intensive care improved the clinical outcome of critically ill patients diagnosed with conditions such as septic shock,4,5 acute stroke, 6 traumatic brain injury, 7 acute myocardial infarction, 8 pneumonia, 9 and cancers with accompanying severe complications. 10 Delayed transfer from the emergency department (ED) to the intensive care unit (ICU) is related to poor clinical outcomes.11–13 ICU mortality and in-hospital mortality were higher and the length of stay in hospital was longer for patients whose transfer from the ED to the ICU was delayed for more than 6 h. 14 A prospective cohort study showed that the hazard ratio of ICU death in patients admitted to the ICU increased by 1.5% with each 1h delay in ICU admission. 15 The need for application of mechanical ventilation and renal replacement therapy increased in cases of delayed transfer to the ICU, and that delayed transfer to the ICU is an important predictor of death, along with age, diagnosis, and severity of disease. 3
Most critically ill patients visit the ED, receive initial treatment, and are then admitted to the ICU. Several factors are associated with delayed transfer of critically ill patients from the ED to the ICU, including ED crowding and limited ICU resources.16,17 Crowdedness of the ED has been found to hamper appropriate treatment and has been considered a critical problem of the medical service system for a long time.18,19 ED crowdedness is related to increased mortality among critically ill patients admitted through the ED. 20 Systematic literature review showed that crowdedness of the ED is related to poor clinical outcomes of patients. 21 ED crowdedness delays antibiotic treatment and increases the time until chest X-ray examination, which negatively impact the quality of treatment offered to patients with pneumonia. 22
Despite the increasing number of patients in need of ICU admission, ICU resources are limited; thus, delayed transfer from the ED to the ICU became a serious problem at our institution. We designed an ICU admission protocol to reduce the ED length of stay for critically ill patients, in which full-time intensivists determined ICU admission priorities based on the severity of illness. We investigated the effect of the ICU admission protocol, controlled by intensivists with full authority, on the ED length of stay among critically ill patients.
Subjects and methods
ICU admission protocol
The Korean Society of Critical Care Medicine (KSCCM) published the Clinical Practice Guideline for ICU Admission, Discharge, and Prioritization in 2013. The Clinical Practice Guideline of the KSCCM was prepared based on the Guidelines for Intensive Care Unit Admission, Discharge, and Triage, published by the Society of Critical Care Medicine in 1999 and later revised. 23 We had been using the guidelines of KSCCM, but most physicians in the ED were unaware of the protocol and rarely applied this to patients. We prepared a new, revised version of the ICU admission protocol based on the guidelines of the KSCCM.
Two full-time intensivists controlled ICU admission according to the protocol. When critically ill patients were admitted to the ED, the physician in the ED carried out resuscitation and, at the same time, decided the need for ICU admission. Emergency physicians directly consulted with intensivists and the intensivists decided the ICU admission priority according to the clinical decision. Our protocol emphasized the clinical decisions of intensivists and simplified the number of ICU admission protocol steps from four to three (Figure 1). Level I patients are those who need ICU admission with the highest priority, including those who have survived after cardiopulmonary resuscitation, those undergoing extracorporeal membrane oxygenation, and those under mechanical ventilation following endotracheal intubation. For level I patients, the ICU prepares for prompt admission ahead of other patients awaiting ICU admission. Level III patients are those who may not benefit from ICU admission, including patients who are expected to have poor clinical outcomes due to terminal stage cancer or chronic disease, and patients with low possibility of clinical deterioration. The intensivists selected patients expected to have poor clinical outcomes due to terminal stage cancer or chronic disease, and received do-not-resuscitate (DNR) orders in advance. The intensivists were able to delay the ICU admission of patients with low possibility of clinical deterioration. Level III patients were admitted to the ICU depending on the availability of ICU beds. All other critically ill patients not levels I and III were classified as level II, including those with unstable vital signs, massive hemorrhage, severe electrolyte imbalance, endotracheal intubation without mechanical ventilation, high probability of clinical deterioration, and those undergoing continuous renal replacement therapy. The ICU admission priority of level II patients was decided only according to the clinical decision of intensivists. The intensivists decided on the priority of ICU admissions by comprehensively considering clinical diagnosis, vital signs, laboratory test results, and clinical course of patients.
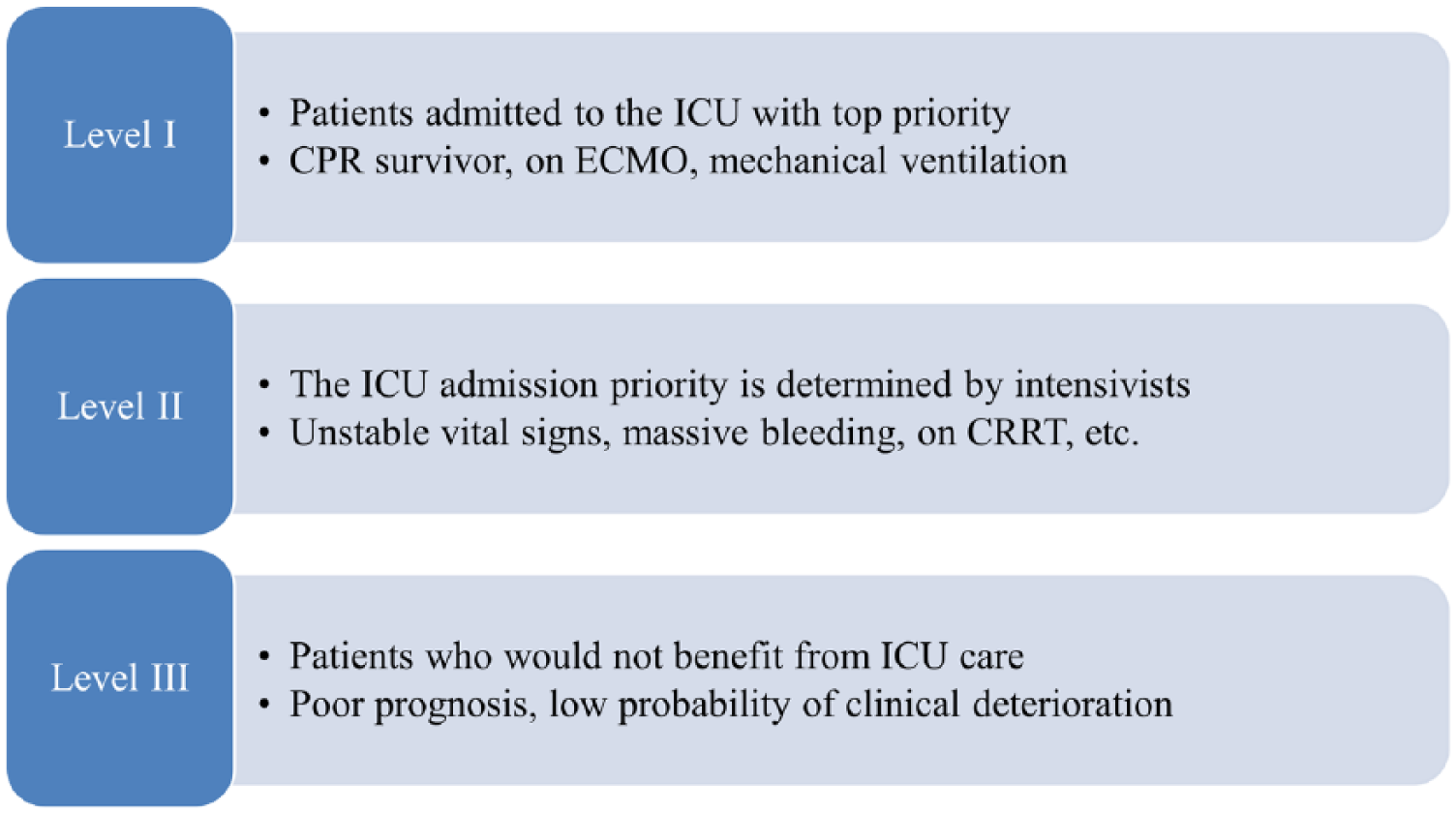
ICU admission protocol in Dong-A University Hospital.
Data collection
This study was conducted in a large academic tertiary care hospital with 1000 beds. The ICU at Dong-A University Hospital (DAUH) is a 22-bed, mixed medical–surgical ICU. Data were gathered from patients who were transferred from the ED to the ICU at DAUH from 1 April to 30 November 2016. The new ICU admission protocol was applied to critically ill patients who visited the ED beginning 1 August 2016. The study protocol was approved by the Institutional Review Board of DAUH. Data regarding demographic variables (i.e. age and sex), and clinical variables (i.e. vital signs, laboratory test results, duration of mechanical ventilation, in-hospital mortality, ICU mortality, ICU length of stay, and application of cardiopulmonary resuscitation) were collected from the medical records. Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were recorded prospectively by ICU physicians. The ED length of stay, which was the primary outcome of this study, was obtained from the ED records.
Statistical analyses
The collected data were analyzed using IBM SPSS version 21.0 (IBM Corp., Armonk, NY, USA) for Windows. Nominal variables were expressed as the number and the incidence rate (%), while continuous variables were expressed as mean ± standard variation or as the median value and the interquartile range, rounded off to one decimal place. Continuous variables that were normally distributed were analyzed using the student’s t-test; those that were not normally distributed were analyzed using the Mann–Whitney U test. Nominal variables were analyzed using the Chi-square test or Fisher’s exact test, as appropriate. Significance was assumed at a p < 0.05 in all the analyses.
Results
Characteristics of patients
The subjects of this study were 292 patients who were transferred from the ED to the ICU from 1 April to 30 November 2016. Of the 292 patients included, 120 and 172 were admitted before and after the introduction of the ICU admission protocol, respectively. Table 1 compares the baseline characteristics of the two groups. In the pre-intervention group, the mean age of the patients was 62.6 (±17.2) years and 78 patients (65%) were male. In the post-intervention group, the mean age of the patients was 63.7 (±16.7) years and 106 patients (61.6%) were male. No significant differences were found between both groups in terms of age and sex. The predominant reasons for admission were infection, including sepsis, septic shock, or organ failure due to severe infection. The proportion of sepsis patients was higher in the post-intervention group than the pre-intervention group; however, this difference was not statistically significant. The mean APACHE II scores at ICU admission were similar. No significant difference was found between the groups in terms of vital signs or laboratory test results at the time of visiting the ED. After the introduction of the ICU admission protocol, there was a significant reduction in the rates of endotracheal intubation and mechanical ventilation in the ED. The proportion of patients who underwent cardiopulmonary resuscitation in the ED also decreased, but there was no statistical significance.
Comparison of baseline characteristics between pre-intervention and post-intervention groups.
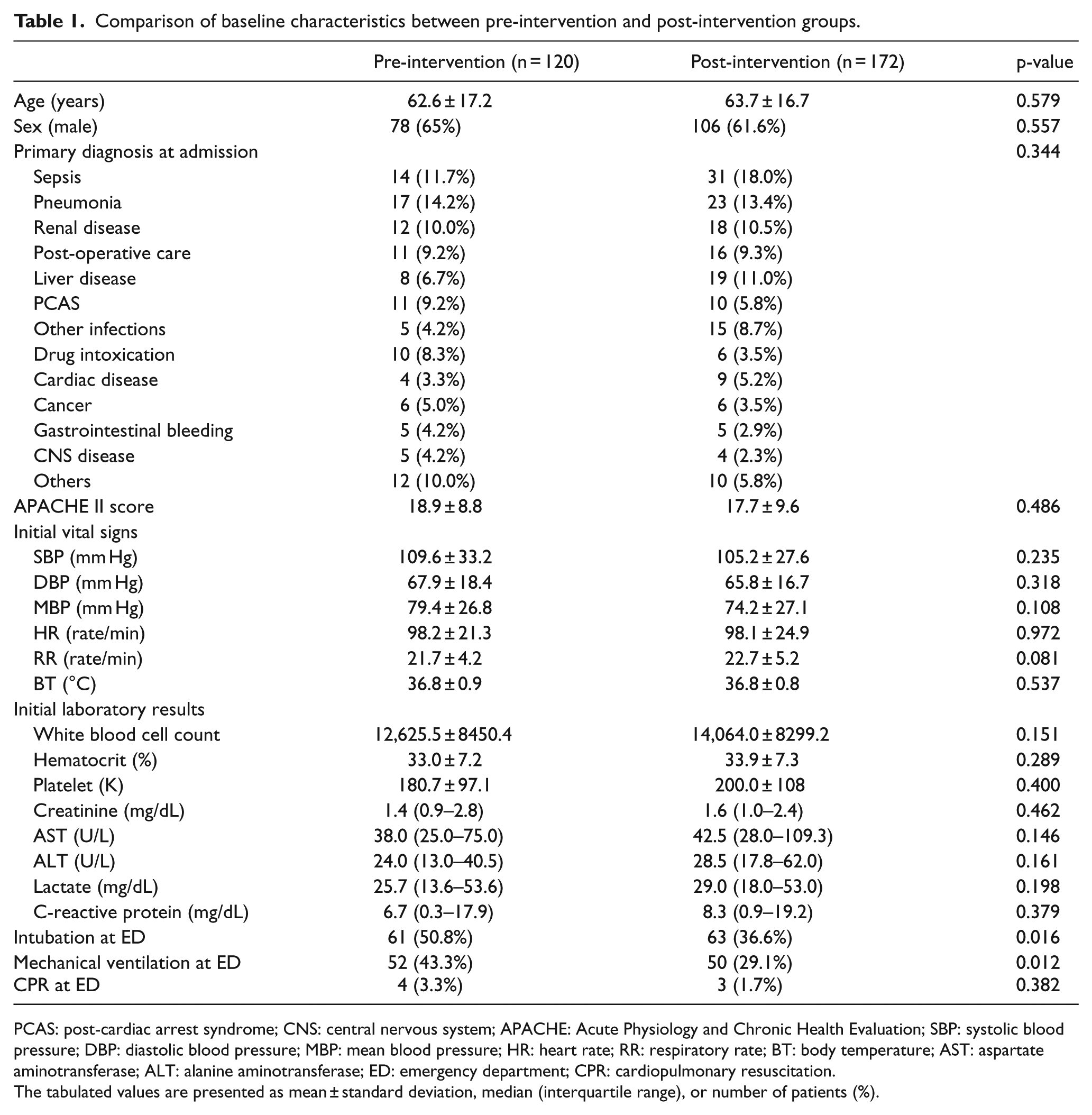
PCAS: post-cardiac arrest syndrome; CNS: central nervous system; APACHE: Acute Physiology and Chronic Health Evaluation; SBP: systolic blood pressure; DBP: diastolic blood pressure; MBP: mean blood pressure; HR: heart rate; RR: respiratory rate; BT: body temperature; AST: aspartate aminotransferase; ALT: alanine aminotransferase; ED: emergency department; CPR: cardiopulmonary resuscitation.
The tabulated values are presented as mean ± standard deviation, median (interquartile range), or number of patients (%).
ED length of stay and clinical outcomes
After application of the new ICU admission protocol, the ED length of stay among critically ill patients significantly decreased from 1045.5 (425.3–1665.3) min to 392.0 (279.3–686.8) min (p < 0.001) (Table 2). According to the transfer procedure from the ED to the ICU, the ED length of stay was divided into time from visit to ED to decision on ICU admission and time from decision on ICU admission to actual transfer to the ICU. The time until the decision on ICU admission (311 min vs 231 min) and the time from the decision on ICU admission to transfer to the ICU (290 min vs 124 min) also significantly decreased depending on the application of the protocol (p < 0.001).
Comparison of emergency department length of stay and clinical outcomes between pre-intervention and post-intervention groups.
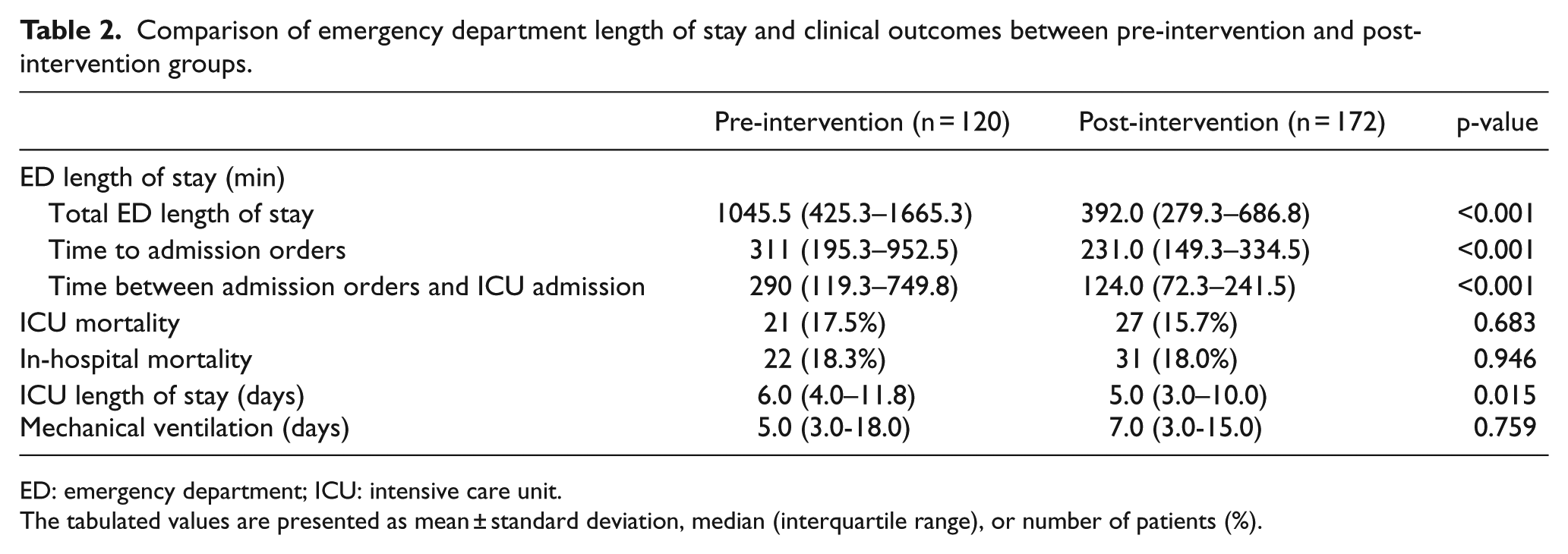
ED: emergency department; ICU: intensive care unit.
The tabulated values are presented as mean ± standard deviation, median (interquartile range), or number of patients (%).
The ICU mortality and in-hospital mortality rates were not significantly different between the groups. The ICU length of stay significantly decreased from 6.0 (4.0–11.8) days for the pre-intervention group to 5.0 (3.0–10.0) days for the post-intervention group. There was no significant difference in the duration of mechanical ventilation (Table 2).
Discussion
In this study, the application of a new ICU admission protocol controlled by intensivists reduced the ED length of stay in critically ill patients. After application of the admission protocol, the entire ED length of stay decreased by 650 min, and both the time required to decide on admission and the time for admission preparation also significantly decreased. In addition to the ED length of stay, the ICU length of stay also decreased significantly between the two groups with similar variables including age, sex, and APACHE II score at ICU admission. This implies that critically ill patients were promptly transferred from the ED to the ICU and received early intensive care, leading to their early discharge. Many previous studies have shown that early intensive care for critically ill patients improves clinical outcomes.4–10
There are complicated reasons for transfer delay from the ED to the ICU.16,17 Before implementation of the ICU admission protocol, when critically ill patients presented to the ED, emergency physicians first performed resuscitation of patients and then consulted with the physician in the relevant department. Patients with multiple conditions had delayed admission to the ICU until all relevant departments had made decisions about patient care. After implementation of the protocol, emergency physicians determined the need for ICU admission and consulted with the intensivist for rapid ICU admission. Some critically ill patients with complicated problems were directly admitted to the Department of Intensive Care Medicine. Another important factor in the transfer delay to the ICU was ICU overcrowding.16,17 For efficient utilization of ICU resources, we produced an ICU admission and discharge protocols and educated medical staff about such protocols. Furthermore, we attempted to secure ICU beds for level I patients and prepared for the ICU admission of these patients from the ED with top priority.
Delayed ICU admission and prolonged ED stay has been a burden to emergency physicians.18–22 Until ICU admission, emergency physicians performed all treatments, including endotracheal intubation, mechanical ventilation, continuous renal replacement therapy, extra-corporeal membrane oxygenation, and so on. We designed the new ICU admission protocol to reduce the ED length of stay for critically ill patients. To implement the ICU admission protocol, we educated medical staff about the protocol, and emergency physicians and intensivists worked together to shorten the ED length of stay. The combined effort of emergency physicians and intensivists to implement the admission protocol may have affected the ICU length of stay. As a result, we could promptly hospitalize critically ill patients to the ICU and discharge improved patients to general wards.
The new ICU admission protocol enabled efficient operation of the ICU by reducing the ICU length of stay. Decreased ICU length of stay is important, as it leads to the efficient utilization of ICU resources. The ICU bed turnover ratio increases as the ICU length of stay decreases, which means that more critically ill patients can receive ICU care. Since ICU resources are limited, despite increasing demand for intensive care, there is a need for an efficient method of utilizing limited ICU resources.16,17,24 The application of the new admission protocol that prioritizes ICU admission may be a method for efficient operation of the ICU.23,25
The ICU admission priority levels of critically ill patients were determined only by the clinical judgment of the intensivists, who comprehensively considered the diagnosis, vital signs, laboratory test results, and clinical course of patients. No completely scientific evidence-based ICU admission protocol has been available until now, and decisions on ICU admission have been mostly dependent on clinicians who determine the clinical severity of patients’ conditions.26,27 The judgment of patient condition may be more accurate when made by experienced physicians, rather than judgment based on formulaic and objective numerical values. 28 A recent study showed that for the prediction of long-term outcomes, including in-hospital mortality and 6-month mortality among critically ill patients, clinical judgments made by physicians were more accurate than the results of an outcome prediction model based on objective numerical values. 29
The purpose of the ICU admission protocol is to select patients who may benefit from ICU treatment from those who would not. 30 We classified patients who would not benefit from ICU admission as level III. Patients who were expected to have poor outcomes submitted DNR consent, and ICU admission of patients with a low possibility of clinical deterioration was postponed. A previous study defined two groups of patients who may benefit less from ICU treatment than from treatment in wards; one group with stable conditions not requiring ICU treatment and the other group with unrecoverable conditions that would not benefit from ICU treatment. 31 The meaningless life-sustaining treatment for critically ill patients is related to delayed treatment of other patients. 32
This study has several limitations. First, this was a single-center retrospective study and thus is prone to all limitations associated with this design. Second, confounding variables could not be eliminated because historical controls were used. We compared the clinical data of patients before and after protocol application. Although the basic characteristics of the two groups were similar, multiple variables that were not controlled might introduce further bias. Third, patients who were transferred to other hospitals after ceasing treatment may have been included, thus affecting duration of ICU stay and available mortality data. Fourth, data from patients who visited the ED and consulted with an intensivist during the study period were not available. It was also impossible to investigate the proportion of patients admitted to the ICU before and after the implementation of the protocol.
Conclusion
The ICU admission protocol authorized the intensivists to make ICU admission decisions, and intensivists rapidly triage critically ill patients to the ICU. The ICU admission protocol controlled by intensivists significantly decreased the ED length of stay and the ICU length of stay in critically ill patients at our institution. Our data suggest that an ICU admission protocol operated exclusively by intensivists will enable efficient operation of the ICU by reducing both the ED waiting time and ICU length of stay.
Supplemental Material
5_Supple – Supplemental material for Intensive care unit admission protocol controlled by intensivists can reduce transfer delays from the emergency department in critically ill patients
Supplemental material, 5_Supple for Intensive care unit admission protocol controlled by intensivists can reduce transfer delays from the emergency department in critically ill patients by Ji Eun Kim, Seul Lee, Jinwoo Jeong, Dong Hyun Lee and Jin-Heon Jeong in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
J.E.K., S.L., J.J., D.H.L., and J.-H.J. contributed to the study design and data collection. J.E.K. and J.-H.J. analyzed the data and drafted the manuscript. S.L., J.J., and D.H.L. contributed to the data analysis and editing of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dong-A University Research Fund. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
The ICU admission protocol is provided as Supplementary Appendix 1. The primary data used in the analysis can be provided if requested.
Informed consent
This was a retrospective study using medical records. Informed consent was waived by the Institutional Review Board of Dong-A University Hospital.
Ethical approval
The study protocol was approved by the Institutional Review Board of Dong-A University Hospital.
Human rights
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s Human Research Committee.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.