
Abstract
A 70-year-old man presented to the emergency department with a 2-week history of watery diarrhea. Fecal materials were found in the Foley catheter. A computed tomography of the abdomen and pelvis revealed chronic diverticulitis with enterovesical fistula. The patient was treated with broad-spectrum antibiotics and underwent an urgent surgery with a transverse loop colostomy. The presence of fecaluria should raise the clinical suspicion of enterovesical fistula. Computed tomography is the choice of diagnostic modality.
Case
A 70-year-old man with diabetes mellitus and dementia was brought to our emergency department (ED) with a 2-week history of watery diarrhea. On his ED admission, he was severely hypothermic (tympanic temperature 32.0°C) and hypotensive (blood pressure 75/42 mmHg). His abdomen was soft and flat, without tenderness to palpation. Plain radiographs of the chest and the kidney, ureter, and bladder (KUB) were unremarkable. Complete blood counts revealed marked leukocytosis. Biochemistry studies found prerenal azotemia. He was treated as septic and hypovolemic shock. A 16-Fr two-way Foley catheter was placed to monitor urine output. Some brownish debris was noted in the Foley catheter; hence, fecal materials in the urine were suspected (Figure 1). His urinalysis revealed a specific gravity of 1.018, a pH of 6.0, and per high-power field, 638 white blood cells (WBCs), 20 red blood cells (RBCs), and >100 bacteria. The urinary levels of nitrite, urobilirubin, and bilirubin were unremarkable. A computed tomography (CT) of the abdomen and pelvis (Figures 2 to 4) was obtained.

Fecal materials in the Foley catheter (arrow).

CT (axial view) of the abdomen and pelvis.

CT (coronal view) of the abdomen and pelvis.
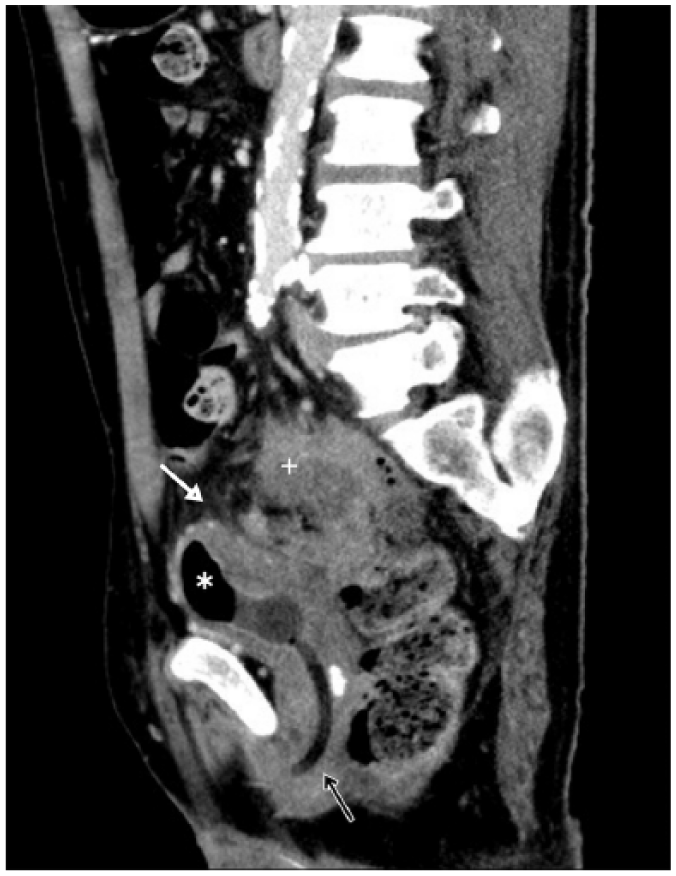
CT (sagittal view) of the abdomen and pelvis.
Questions
How do you describe “fecal materials in the urine”?
What were the CT findings?
What was the diagnosis?
Answers
Fecaluria.
The axial view of CT (Figure 2) showed colon mural thickening with air pockets (white arrow), a distended urinary bladder with irregular wall thickening (black arrow), and an air-fluid level within the urinary bladder (asterisk). The coronal view of CT (Figure 3) showed a dilated colonic loop with intraluminal air and stasis of fecal materials (white arrow), and adjacent fat infiltrations of the rectosigmoid colon and urinary bladder (black arrow). The sagittal view of CT (Figure 4) showed inflammatory masses over the rectosigmoid colon (cross), adjacent fat infiltrations of the rectosigmoid colon and urinary bladder (white arrow), an air-fluid level within the urinary bladder (asterisk), and a Foley catheter in place (black arrow).
The diagnosis was chronic diverticulitis with enterovesical fistula.
Discussion
The patient was treated with broad-spectrum antibiotics and inotropic agents. He underwent an urgent surgery with a transverse loop colostomy and was admitted for intensive care. His urine culture yielded Morganella morganii and Enterococcus avium. The enterovesical fistula could be associated with chronic diverticulitis involving the adjunctive urinary bladder. He was discharged smoothly after a hospital stay of 68 days.
Diverticulosis is affecting nearly half of adults over 50 years old. Patients with acute diverticulitis usually have a combination of left lower quadrant pain, tenderness, leukocytosis, and fever. However, only 57% of patients with chronic diverticulitis had left lower quadrant abdominal pain, and these patients rarely had abdominal tenderness, rebound, guarding, fever, or leukocytosis. 1 The intra-abdominal complications of chronic diverticulitis include an abscess or phlegmon, fistula formation, stricture disease, bowel obstruction, or peritonitis. Enterovesical fistula is a rare but devastating complication of various malignancies or inflammatory diseases. 2 Symptoms of enterovesical fistula may originate from the gastrointestinal or urinary tract. 3 Clinical suspicion of enterovesical fistula may arise from fecaluria, pneumaturia, or malodorous urine. 4 CT scans are the choice for diagnosing enterovesical fistula and surveying the adjacent anatomical structures. 5 Treatments include broad-spectrum antibiotics and timely surgical intervention. 5
Footnotes
Acknowledgements
P.-H.F and W.-Y.L. drafted the manuscript and contributed equally as the first authors. All authors contributed substantially to the revision of the manuscript. C.-H.L. is the corresponding author who takes responsibility for the paper as a whole.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s family for their anonymized information to be published in this article.
Ethical approval
The study procedures were in accordance with ethical standards.