
Abstract
Background:
The healthcare need of the elderly in Hong Kong is a major issue. Foreign domestic helpers, especially those from the Philippines, play a significant role in response to the healthcare need of a home-dwelling elder as they are often the sole caregiver of the elders.
Objectives:
This study primarily aimed at exploring the Filipino domestic helpers’ knowledge of and attitude to managing a medical emergency of a home-dwelling elder.
Methods:
This was a questionnaire survey of the Filipino domestic helpers working in Hong Kong and was conducted from 1 July 2015 to 29 February 2016. The survey collected their demographic data, evaluated their first aid knowledge by a test of multiple-choice questions and assessed their attitudes to providing first aid to the elders they cared in terms of confidence and perceived responsibility. Descriptive statistics were used to describe the findings.
Results:
In all, 398 Filipino domestic helpers were surveyed. Most had completed university education. About one third had been trained in first aid. The average mark attained by the respondents on first aid knowledge assessment was 4.5 (full mark = 16). Their knowledge was especially poor in heat exhaustion, choking, external bleeding, epistaxis and scald injury. Their median confidence score was 10 (full score = 15) and median perceived responsibility score was 13 (full score = 20).
Conclusion:
The first aid knowledge among the Filipino domestic helpers surveyed in this study was poor. They were not confident enough in providing first aid to an elder and their perceived responsibility was also low.
Keywords
Introduction
The population of Hong Kong (HK) is aging. The proportion of people aged 65 and over is expected to rise from 13% in 2011 to 30% in 2041. 1 Their healthcare need is a major issue that cannot be neglected. Because of the socio-economic condition of HK, it is not uncommon that families with elders employ foreign domestic helpers to perform household duties and serve as live-in caretakers of the home-dwelling elders. In 2013, there were about 320,000 foreign domestic helpers in HK, of whom 51% were from the Philippines. 2 Because of the large number of families served by them, they may play an important role in response to the healthcare need of a home-dwelling elder. This is indirectly supported by a local finding that domestic helpers, who served as caregiver to an elder, had an impact on the risk of institutionalization of the elder. 3 The elders are vulnerable to acute deterioration of their health and are major users of the emergency medical services in HK. 4 It is therefore important for the domestic helpers, who are often the sole caregivers of the home-dwelling elders, to know how to manage a medical emergency before the emergency medical service is available. This study primarily aimed at exploring Filipino domestic helpers’ (FDHs) knowledge of and attitude to managing a medical emergency of a home-dwelling elder. The secondary objective was to examine the relationship between FDH’s knowledge in medical emergencies and their demographic variables.
Methods
This was a questionnaire survey conducted from 1 July 2015 to 29 February 2016. The questionnaire for the survey consisted of three parts with 31 questions. The first part collected data on the demographic characteristics of the FDHs. The second part consisted of 16 multiple-choice (4-item) questions on the FDH’s knowledge of managing a medical emergency. The questions were adapted from the question bank included in the Hong Kong Red Cross First Aid Manual. They were chosen in such a way that they represented a variety of geriatric medical emergencies encountered in a household environment, including choking, loss of consciousness, bleeding, heart attack, stroke, heat exhaustion, hypothermia and scald injury. The questions were written in simple English and medical terms were replaced by layman terminology for easy comprehension. Each correct answer would score 1 mark. No marks were deducted for wrong answers. The possible mark ranges from 0 to 16. The higher the mark, the better their knowledge was. The third part was to assess the FDH’s attitudes to managing a medical emergency. Two sets of statements were used to assess two domains of attitude, respectively: their confidence to perform first aid in response to a medical emergency to an elder (questions 17–19) and their perception of responsibility to provide first aid treatment (questions 20–23). These statements were modified from a survey carried out by the Hong Kong Red Cross in June 2011 on ‘Public Knowledge and Attitude on First Aid’. 5 A Likert-type scale was used to assess their response to the statements. The Likert-type scale was a 5-point one (strongly disagree, disagree, neutral, agree, strongly agree). Each position was given a score from 1 to 5. Questions 18 and 22 were reversely scored. The scores were then added up to give an overall measure for the two domains, respectively. For the set of statements about confidence, the higher the score, the stronger the confidence (range = 3–15). For the second set about perception of responsibility, a higher score reflected a bigger perceived responsibility (range = 4–20).
The FDHs were recruited by convenience sampling from helpers participating in activities organized by the Domestic Helper Empowerment Project, which is a Student Development Project under the Centre of Development and Resources for Students of the University of Hong Kong and from the FDHs gathering in Central on eight Sundays during the study period. FDHs of all ages and gender who had a legal employment contract at the time of recruitment and consented to participate in the study were enrolled. These criteria ensure that the participants are legal residents of HK and by legal status, domestic helpers. Another inclusion criterion was that there was at least one elder in the family they were working for. Those who failed to communicate in English were excluded as the questionnaire was provided in English only. An eligible FDH would be given the questionnaire after an investigator had explained to her or him about the study and obtained consent from them. They were asked to complete the questionnaire within 60 min. Discussion with other FDHs was discouraged. Participation was completely voluntary and anonymous. No reward was given to the participants. Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference number: UW15-335).
The demographic characteristics and knowledge level of the FDHs were described by descriptive statistics. With reference to the knowledge level, comparison was made in FDHs who had past experience of handling an emergency in the elders or not, who had experience of taking care of elders or not and who had received first aid training previously or not. Their knowledge level was also compared according to their education level and employment history including duration and type. Significance testing was by chi-square test. A p-value < 0.05 was considered significant. The responses of the FDHs to the statements in part 3 of the questionnaire were treated as ordinal data. Descriptive analysis was used for analysis and they were reported as median and interquartile range (IQR). For sample size, to attain a margin of error of 5% with a confidence level of 95% regarding FDHs’ knowledge level (assumed to be 50% of correct answers to maximize the sample requirement), the minimum sample size was 385. All statistical analyses were done by IBM SPSS Statistics 23 and Microsoft Excel 2013.
Results
A total of 318 out of 350 FDHs invited from the Domestic Helper Empowerment Project and 80 out of 120 invited in Central completed the survey. The response rate was 90.9% and 66.7%, respectively. The demographic characteristics of the respondents are summarized in Table 1. There was female predominance (99.0%). About 66% of the respondents had university level of education. Nearly 70% of them had no experience in taking care of an elder. About 34% of them had ever had first aid training.
Demographic characteristics of the Filipino domestic helpers (N = 398).
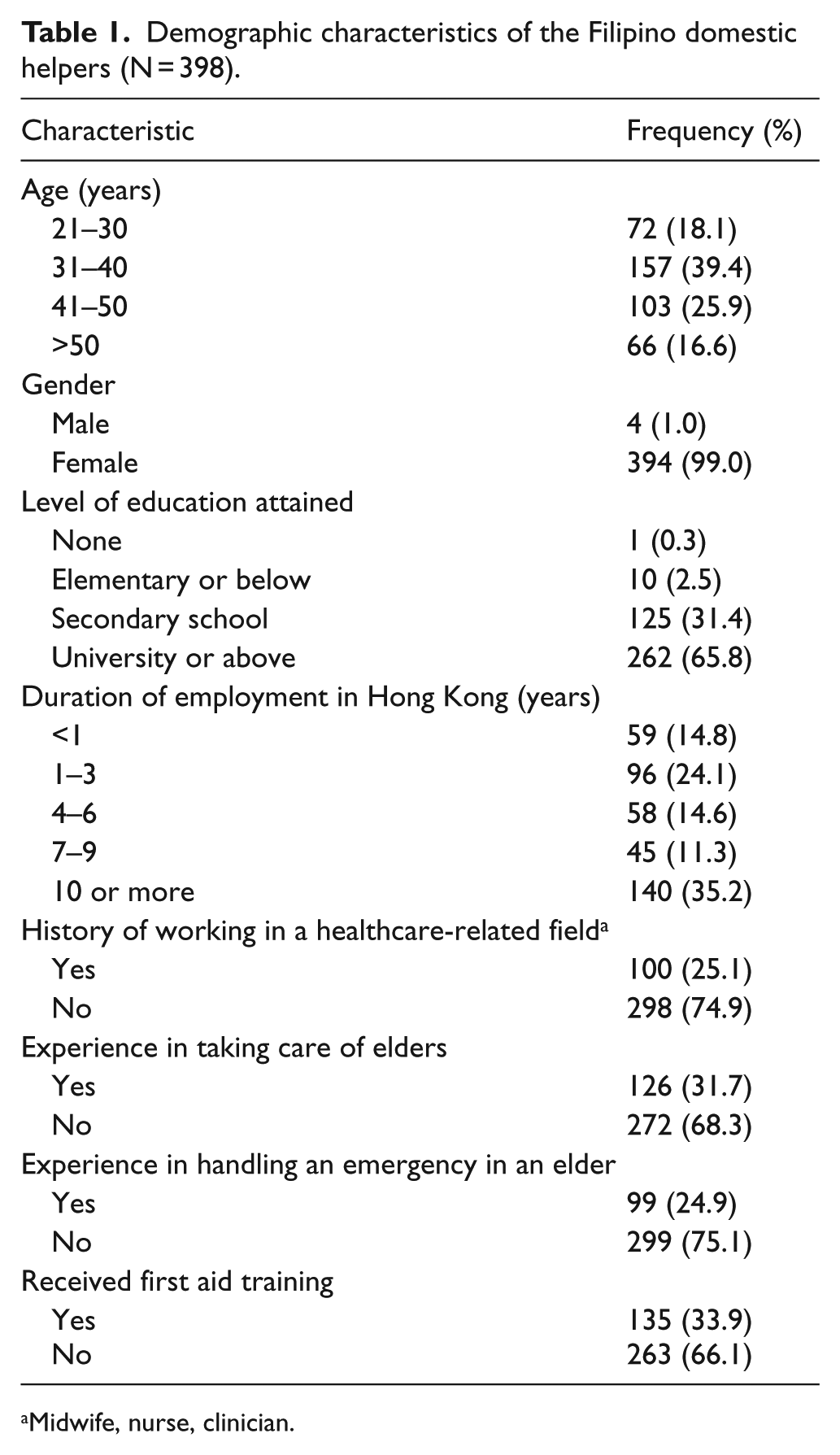
Midwife, nurse, clinician.
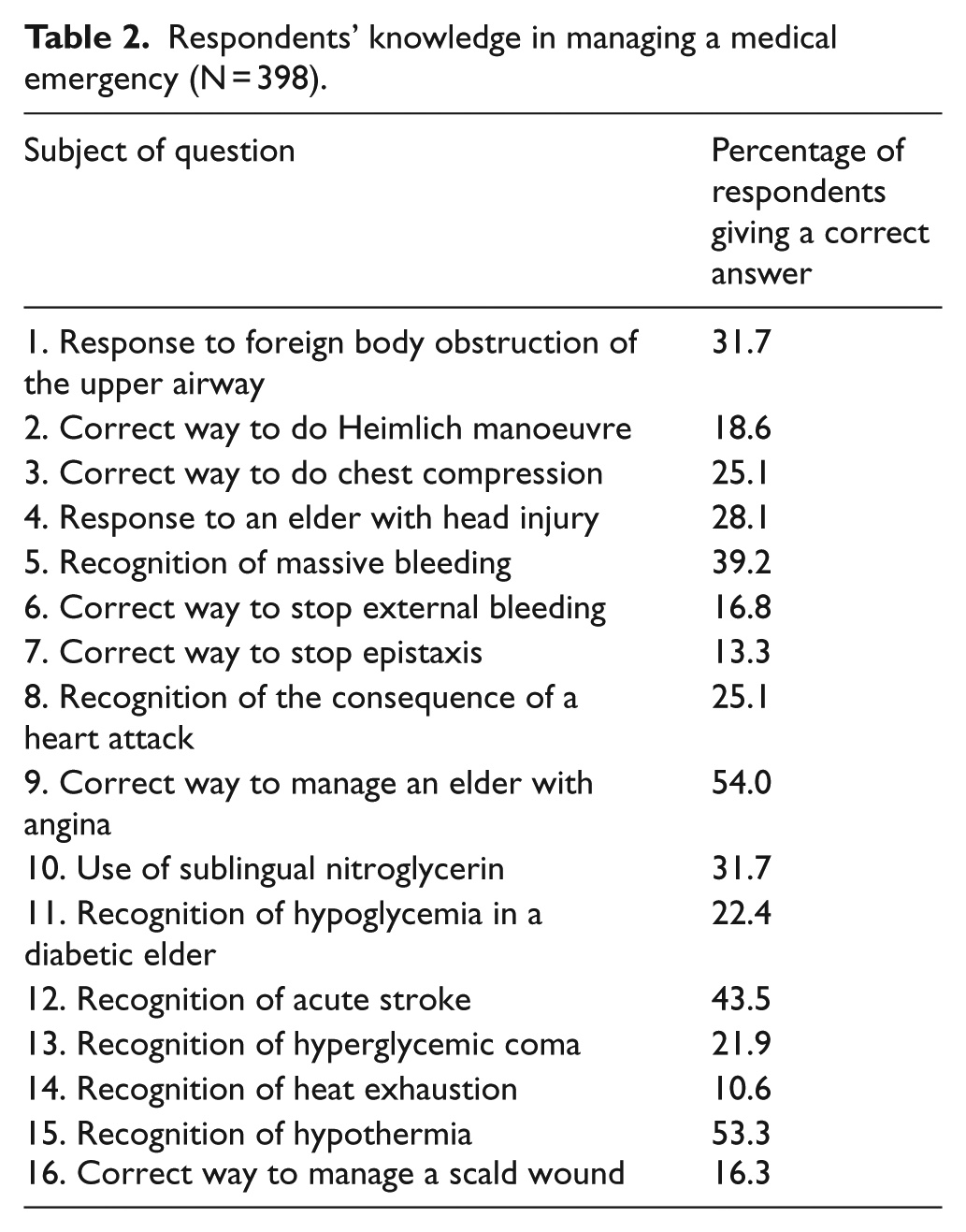
The average mark attained by the respondents on first aid knowledge assessment was 4.5. The range was from 1.0 to 12. Only 8% of the respondents were able to answer at least half of the questions correctly. Table 2 shows their performance in terms of percentage of respondents giving a correct answer to a question. They did most poorly on recognizing heat exhaustion. Only 10.6% could give a correct answer. Less than 20% of the respondents answered correctly on first aid of choking, external bleeding, epistaxis and scald injury. FDHs who previously worked in a healthcare-related field, who had past experience in handling a medical emergency in an elder, who had higher education level and who had been trained in first aid scored a significantly higher mark (Table 3).
Respondents’ knowledge in managing a medical emergency (N = 398).
Comparison of demographic characteristics and knowledge in managing a medical emergency.
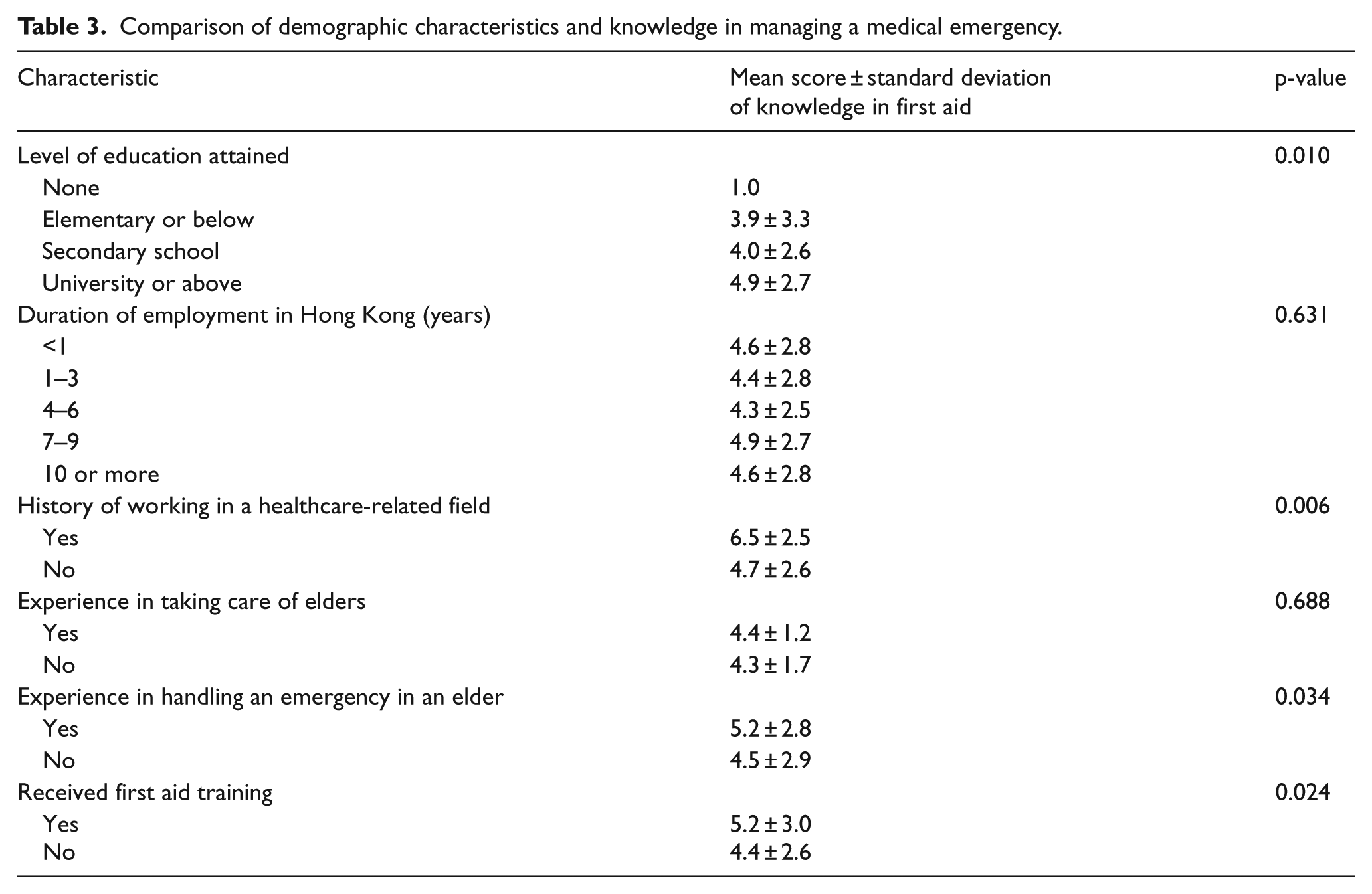
Table 4 is the results of attitude assessment. Concerning the FDHs’ confidence to perform first aid in response to a medical emergency in an elder, the overall median score was 10 with an IQR of 9 and 11. Nearly 80% of FDHs agreed that they would perform first aid to an elder if they possessed the knowledge and skills. For their perception of responsibility to provide first aid treatment, the overall median score was 13 (IQR: 12, 14). Of note, over 60% of them thought that it is the medical professional’s responsibility to provide first aid in the first place.
Respondents’ attitudes to managing a medical emergency in an elder (N = 398).
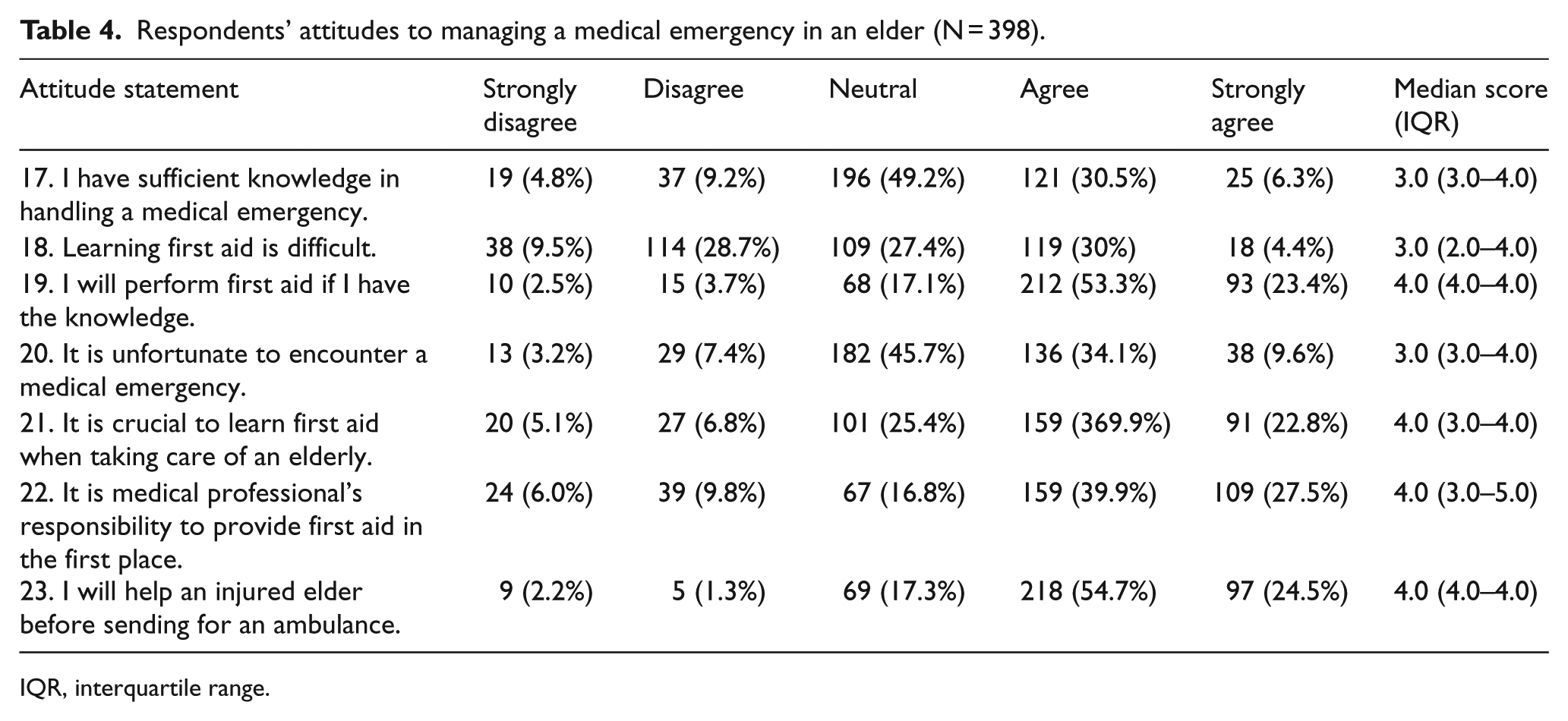
IQR, interquartile range.
Discussion
In the medical literature, the number of studies about the level of first aid knowledge among workers of a certain occupation, for example, school teachers and industry workers, is limited.6,7 This study is probably the first one that evaluated the first aid knowledge of FDHs working in HK and their attitudes towards the first aid management of an elder with a medical emergency.
From this study, it was found that first aid knowledge among FDHs in HK is far from sufficient. The average mark attained by the respondents was 4.5, which is less than one third of the full mark. Their first aid knowledge was particularly poor in how to relieve foreign body obstruction, stopping bleeding especially epistaxis, managing a scald injury and recognizing heat exhaustion. These and other medical conditions used in the questionnaire are not uncommon among elders. Prompt first aid may minimize morbidity and even avoid mortality. Since the FDHs are often the main caregiver to a home-dwelling elder, their suboptimal first aid knowledge as revealed by the test cast doubt on their ability to help the elder they take care of in a medical emergency. At present, it is not mandatory for an FDH to have first aid training. In view of their poor first aid knowledge, it seems reasonable to propose that pre-employment first aid training should be compulsory, especially for the FDHs who are to work in a household with elderly members.
FDHs who had previously worked in a healthcare-related field, had past experience in managing an emergency in an elder, had attained university education and had been trained in first aid were able to attain a higher mark in the knowledge test. Even so, their marks were still below an acceptable pass of answering correctly in at least 50% of the questions. This suggests that the first aid knowledge of FDHS in HK is in general poor. It is not surprising to find that those with past working experience in a healthcare-related field scored a higher mark. This may be attributed to their previous working experiences in a medical environment that requires better knowledge of first aid principles. For FDHs with history of managing an emergency in an elder, their better performance in the knowledge test may reflect the importance of learning in a real, hands-on situation. FDHs who were university graduates did better in the test. This may be explained by their better comprehension of English, as the test was written in English and not their native language of Tagalog. Previous training in first aid was found to be a statistically significant positive factor in test score. This indicates that previous training would have at least some use on improving the respondents’ knowledge on managing an elder in an emergency.
As for their attitudes towards managing a medical emergency in an elder, the findings suggest that they lack confidence in providing first aid. This is reflected by an overall median score of 10. A more clear-cut indication of confidence is a score of 12 (score 4 in the three questions). This is supported by the finding that over 60% of respondents were either neutral in or disagreed to the notion that they had sufficient knowledge in handling an emergency in an elder. Their perceived responsibility to provide first aid treatment to an elder was also low as evidenced by an overall median score of 13, which is below a more clear-cut score of 16 (score 4 in the four questions) indicating perceived responsibility. It is worrisome to find that nearly 67% of them thought that it was medical professional’s responsibility to provide first aid in the first place. This inevitably results in delay in giving the necessary first aid to an elder in need. Another study that investigates the reasons of low confidence and low perceived responsibility may be warranted. From this study, it is difficult to attribute the low confidence and low perceived responsibility to the low first aid knowledge level. However, it may be reasonable to say that these three aspects are inter-related and may lead to a vicious circle.
Limitations
The representativeness of the respondents is undermined by the adoption of convenience sampling method. Convenience sampling is associated with selection bias of subjects for the survey. Thus, the findings of this study may not reflect the actual situation among the population of FDHs in HK. The responses to the attitude statements were self-reported and not validated. This may result in information bias. Although only those FDHs who could communicate in English were recruited, the confounding effect of poor understanding of English cannot be completely excluded. Furthermore, the investigators were not able to obtain the characteristics of non-respondents for comparison.
Conclusion
The level of first aid knowledge among the FDHs surveyed in this study is low. They also lack confidence in providing first aid to an elder in need. What is worrisome is many of them did not think that they had the responsibility to provide first aid to the elder they look after in the first place. Making first aid training a mandatory requirement for an FDH to work in a household with elderly members may be necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Summarized in tables included in other parts of the submission.
Informed consent
By Consent form (attachment).
Ethical approval
Approved by the Institutional Review Board of the University of Hong Kong/Hospital, Authority Hong Kong West Cluster (HKU/HA HKW IRB) (IRB Reference number: UW 15-335).