
Abstract
Introduction:
Rectus sheath haematoma is a rare condition which is often misdiagnosed. Apart from abdominal trauma and anticoagulation, severe coughing is an uncommon precipitating cause of this rare condition.
Case presentation:
An elderly gentleman with history of ischaemic heart disease on aspirin developed rectus sheath haematoma due to severe coughing during an episode of acute exacerbation of chronic obstructive pulmonary disease. He developed severe abdominal pain and was noted to have epigastric bruising extending to bilateral loins. Ultrasound abdomen and computed tomography of the abdomen with contrast revealed haematoma over bilateral upper rectus abdominis muscles, which subsided with conservative management.
Discussion and conclusion:
Rectus sheath haematoma can be related to severe coughing. In patients, especially those with predisposing factors, presenting with abdominal pain and palpable painful abdominal mass, clinicians should raise the suspicion of this uncommon cause so that timely and appropriate management can be provided.
Introduction
Rectus sheath haematoma (RSH) is a rare condition well known to be associated with blunt abdominal trauma and anticoagulation therapy. 1 However, it can also be related to violent coughing. 2 Although it is often self-limiting, potential fatal complications can occur. 3 It is important to keep this condition in mind when evaluating patients presenting with abdominal pain and palpable abdominal mass, especially if they are on anticoagulation therapy. The present case report describes an elderly gentleman on aspirin who developed RSH due to severe coughing.
Case report
A 76-year-old gentleman having a history of atrial fibrillation (AF), non-ST segment elevation myocardial infarction and chronic obstructive pulmonary disease (COPD) was admitted to the emergency medicine ward (EMW) for management of acute exacerbation of COPD. He was taking digoxin and diltiazem for his AF and aspirin for his ischaemic heart disease. He was afebrile with stable vital signs in room air. Physical examination revealed bilateral diffuse rhonchi on auscultation of his chest. Complete blood count (CBC) showed normal white cell count 7.6 x 109/L (reference range: 3.7 to 9.2 x 109/L), haemoglobin 16.4 g/dL (reference range: 13.4 to 17.1 g/dL) and platelet count 158 x 109/L (reference range: 145 to 370 109/L). His clotting profile, liver and renal function tests were grossly unremarkable. Chest X-ray showed consolidative change over the right lower zone and no pneumothorax. After admission, he developed an episode of fast AF which was controlled with amiodarone. Dosage of diltiazem was titrated to optimize his heart rate control.
During his inpatient stay, he experienced severe coughing and complained of severe chest and epigastric pain with pain score up to 9 out of 10. Serial electrocardiography revealed no new ischaemic changes. Blood amylase level and repeated troponin I levels were normal. He developed epigastric bruising (Figure 1(a)). Aspirin was withheld immediately. Ultrasound (USG) of abdominal wall showed bilateral rectus abdominis muscles enlargement with altered echogenicity. Anechoic areas were seen within. No increased colour flow Doppler was noted. The sonographic features were suggestive of haematoma formation in the abdominal wall muscles (Figure 2). Serial CBC showed no significant haemoglobin drop. However, his abdominal wall bruising progressively extended to bilateral loin regions (Figure 1(b) and Figure 1(c)). Computed tomography (CT) of the abdomen with contrast was then arranged and showed bilateral upper rectus abdominis muscles were mildly enlarged, slightly more on the right side, being isodense to hypodense showing no contrast extravasation or significant enhancement (Figure 3). Features were consistent with haematomas, likely resolving in the presence of hypodense areas within. He was managed conservatively. His chest condition improved with bronchodilators, steroids, antibiotics and chest physiotherapy. Aspirin was then resumed. Patient remained stable and was subsequently discharged. He was followed up 1 week afterwards. On reassessment, his abdominal wall bruising was resolving. Repeated CBC showed static haemoglobin level.
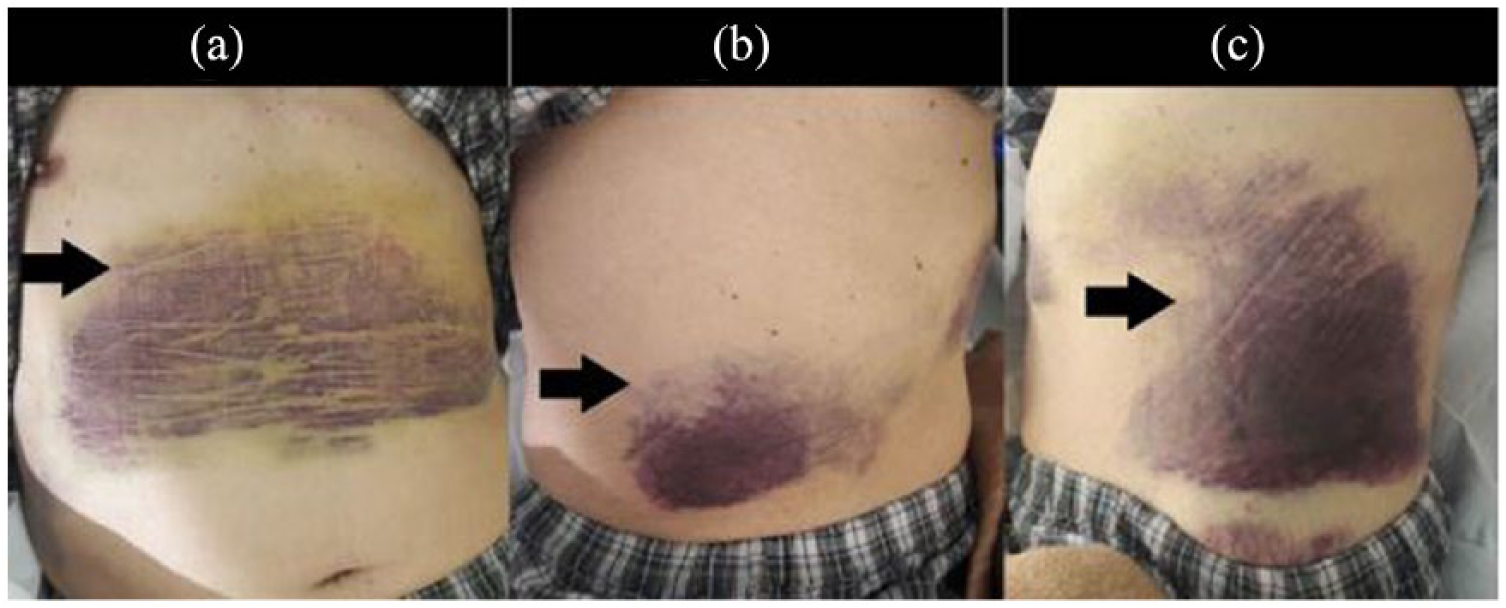
Bruising (black arrows) over epigastric region of the patient (Figure 1(a)) and progressively extending to bilateral loins (Figure 1(b) and 1(c)).
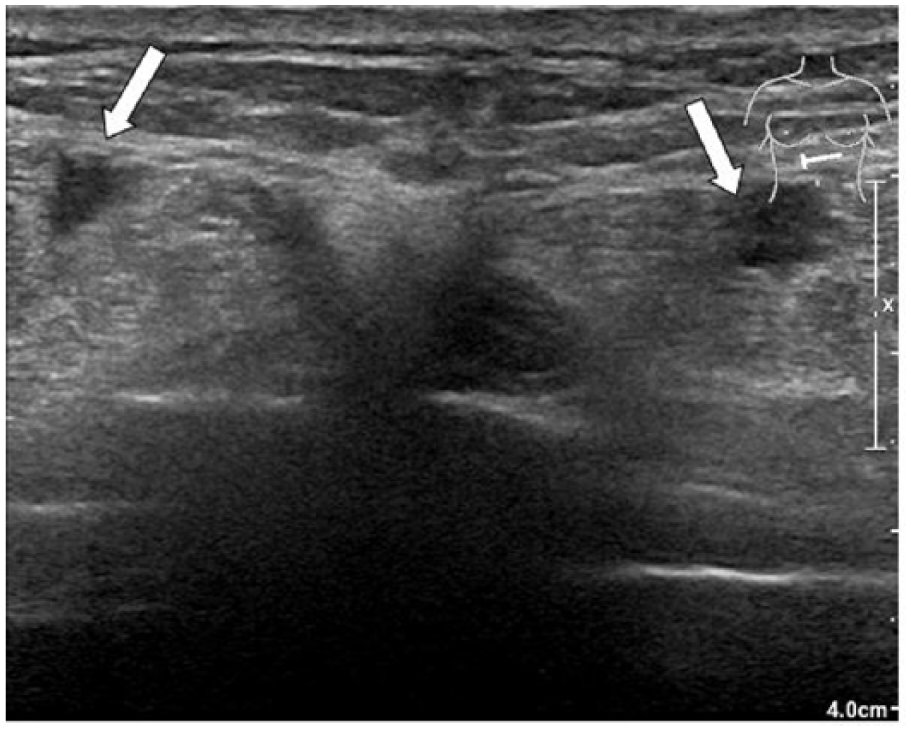
Ultrasound showed enlarged bilateral rectus abdominis muscles with altered echogenicity. Anechoic areas were seen within (white arrows).
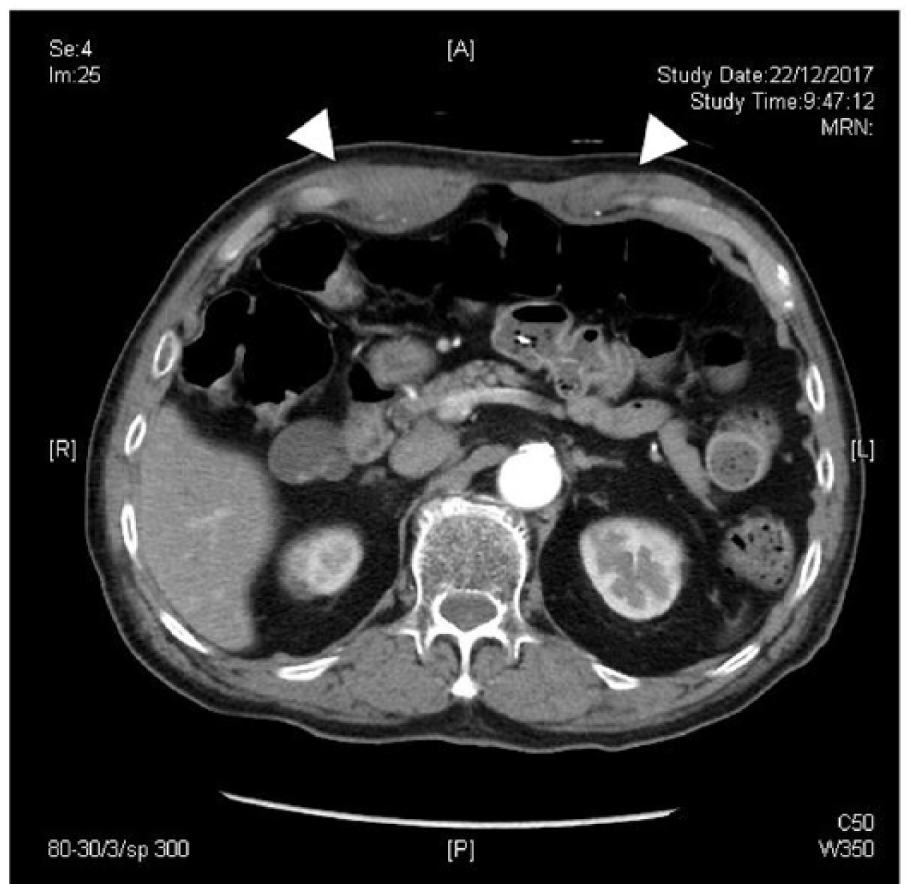
CT abdomen image showed enlarged bilateral rectus abdominis muscles which were iso- to hypodense in the image (white heads). No contrast extravasation or significant enhancement was noticed.
Discussion
Coughing-induced abdominal wall haematoma is a relatively rare condition. Bleeding could occur in various abdominal wall muscles. Rectus sheath is the most commonly involved.1,2 Abdominal muscle contraction during coughing causes either direct tear of the rectus muscle or rupture of epigastric arteries supplying the muscle leading to formation of RSH. RSH is more commonly seen in women. 3 It is possibly due to an anatomic difference that women have less rectus muscle mass. Mean age of patients varies from 46 to 69. 3 The incidence appears to increase with age. 3 The most common precipitating causes are blunt abdominal trauma and the use of anticoagulation therapy. In a review of 115 patients with spontaneous RSH, more than three quarters of the patients (77.4%) were on anticoagulants. 1 Coughing or intense rectus muscle contractions as in vigorous exercise and activities involving significant Valsalva effort has been described as one of the precipitating causes for RSH. 3 In a retrospective review of 126 RSH cases treated at Mayo Clinic, about one third of the patients experienced an acute coughing spell. 2 Apart from RSH, different types of abdominal wall haematomas related to coughing have been reported in the literature over the years. Ozlu et al. 4 reported a case of abdominal wall haematoma between the right internal oblique and external oblique muscles in a 56-year-old lady on aspirin who experienced violent coughing. A 73-year-old lady, who was not on any anti-thrombotic therapy, was reported to develop internal oblique haematoma due to severe cough. 5 Other factors including iatrogenic causes, pregnancy and various medical comorbidities such as hypertension, atherosclerosis and haematological conditions were also described. 1
Presentation of RSH and other abdominal wall haematomas depends on its size and location. More than 80% of RSH patients complained of abdominal pain. Palpable abdominal wall mass was reported in 63%–92% of the cases, abdominal wall tenderness in 71% of the cases and guarding in 49% of the cases. 3 Several clinical signs, including Carnett’s sign, Fothergill’s sign, Cullen’s sign and Grey-Turner’s sign, have been described to aid the clinical diagnosis of abdominal wall haematoma. Large haematomas can result in hypovolaemia and even abdominal compartment syndrome. 3
In diagnosing abdominal wall haematoma, USG is reported to have high sensitivity up to 90%, whereas CT scan has its sensitivity and specificity approaching 100%. 3 On USG image, the haematoma typically appears as a homogeneous and sonolucent cyst-like space, described as spindle shape on longitudinal scan and ovoid shape on transverse and coronal sections. 6 On CT image, acute RSH is characteristically described as hyperdense mass posterior to the rectus abdominis with ipsilateral muscle enlargement anterolaterally. 7 It can be classified into three grades according to the appearance on CT. 3 Grade I RSH is intramuscular, unilateral and does not dissect along the fascia planes. It is generally mild with minimal haemodynamic disturbance. Grade II RSH is bilateral, dissecting along adjacent fascia but without extension into the prevesical space. A minor drop in haemoglobin may be present. Grade III RSH is bilateral and dissects between the transversalis fascia and muscle into the peritoneum and prevesical space. It is the most severe type of RSH with significant haemoglobin drop and haemodynamic compromise. The CT scan in our patient revealed enlarged bilateral rectus abdominis muscles with iso- to hypodense appearance which indicated a subacute nature of the haematomas.
Treatment depends on the clinical condition of the patient and the severity of the haematoma. It is generally regarded as a self-limiting condition. Overall mortality rate is estimated to be around 1.6%. 6 Most patients, including those with Grade I and Grade II RSH, could be managed conservatively with rest, pain relief and optimization of underlying predisposing factors. Fluid resuscitation, blood transfusion and reversal of anticoagulation are given where necessary, especially for grade III RSH. In cases of failed conservative treatment or active significant bleeding, 1 interventional measures, such as angiographic embolization or surgical ligation, are needed. 3
Conclusion
Violent coughing can lead to various complications including rib fractures and abdominal wall haematoma. In the background of rising number of frail elderly patients and increasing use of anticoagulation, clinicians should be aware of this diagnosis to facilitate timely diagnosis and appropriate management of the patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the patient for his anonymized information to be published in this article. A completed consent form is provided separately.