
Abstract
Introduction:
Prognosis of cardiopulmonary arrest occurring in patients with blunt trauma is very poor; patients rarely recover from this condition. We either do not attempt cardiopulmonary resuscitation or terminate it after some time in blunt trauma–cardiopulmonary arrest cases. We presented a rare case of successful resuscitation of a patient with blunt trauma–cardiopulmonary arrest.
Case presentation:
A 54-year-old man was admitted to our emergency department after being injured in a traffic accident. The patient suffered from ventricular fibrillation, and spontaneous circulation was restored by a defibrillator. The estimated arrest time was 20 min.
Discussion:
On arrival of our emergency department, the patient showed intra-abdominal hemorrhage and we performed emergency surgery; 10 days after admission, the patient suffered from pulseless ventricular tachycardia—coronary angiography was performed, which revealed that the patient had coronary artery stenosis.
Conclusion:
We experienced trauma patients concealed with coronary artery stenosis. In traumatic arrest with ventricular fibrillation, it may be due to a medical reason, and more prolonged and intensive resuscitation may be considered.
Introduction
The prognosis of cardiopulmonary arrest (CPA) in patients with blunt trauma (BT) is very poor;1,2 patients rarely recover from this condition. Poor outcomes are typically due to widespread damage from BT, as opposed to the limited damage resulting from penetrating trauma (PT). Furthermore, the neurologic prognosis for BT-CPA patients who survive is extremely poor.3,4 Battistella et al. 3 reported a good neurologic outcome in 3% (9/300) of the patients with PT-CPA and zero patients (0/304) with BT-CPA. In addition, Stratton et al. 4 reported that none (0/382) of their BT-CPA patients experienced a good neurologic outcome.BT-CPA patients have a poor outcome in terms of both overall survival and neurologic prognosis. Therefore, we either do not attempt cardiopulmonary resuscitation (CPR) or terminate it after some time in BT-CPA patients. For this reason, many countries terminate CPR after a certain period of time in almost all BT-CPA patients prior to admission. In Japan, however, all CPA patients are administered CPR regardless of the prognosis. This system has been considered futile or without merit. However, a rare survivor may sometimes be encountered in the midst of this system in Japan. We report a rare case of “BT with CPA,” which was successfully treated to the point of survival with out-of-hospital CPR followed by emergency laparotomy on admission. This patient was neurologically intact upon discharge.
Case report
A 54-year-old man was admitted to our emergency department (ED) after being injured in an unwitnessed traffic accident. The patient was driving alone and crashed unwitnessed into a guardrail. He was pulled out from his vehicle by a pedestrian soon after the accident. He appeared to be suffering from CPA. Immediate CPR in the form of chest compression was initiated while a bystander summoned an ambulance. On reaching the accident site, emergency responders performed electrocardiography (ECG), which revealed ventricular fibrillation (Vf) (Figure 1). Spontaneous circulation was restored by a defibrillator, and the arrest time was estimated as approximately 20 min.
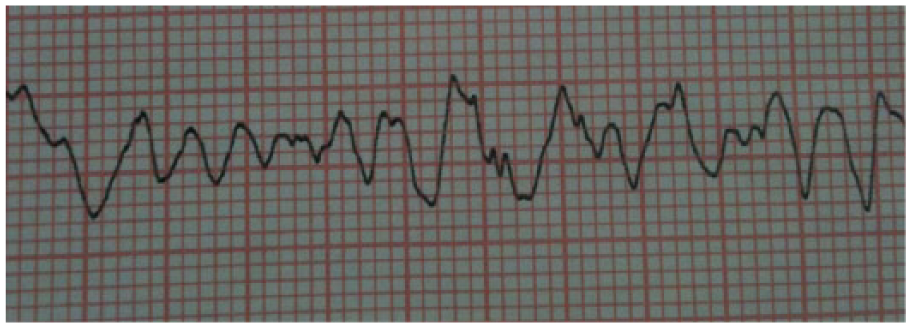
Prehospital initial ECG monitor performed by emergency medical technician (EMT) showed ventricular fibrillation (Vf).
On admission to the ED, the patient’s vital signs were as follows: blood pressure was 143/86 mm Hg, pulse was 90 beats/min, and oxygen saturation was 100% on 10 L of oxygen supplement; the Glasgow Coma Scale score was 4/15 (E1V2M1). Physical examination revealed a lap-shoulder seat belt (3-point) mark on the chest and bilaterally on the lower abdomen (Figure 2). Injury severity score (ISS) was 35 points and calculated probability of survival (PS) was 0.67 at ED. We intubated him and performed focused assessment with sonography for trauma, which only showed left pleural effusion. ECG showed normal sinus rhythm, no axial deviation, and no ST change. The cardiologist commented that this patient had no obvious cardiac disease. Computed tomography showed bilateral lung contusions, left multiple rib fractures, mesenteric injury (Figure 3), and some abdominal fluid. Because the accumulation of fluid in the patient’s abdomen increased and acidosis worsened over the next 12 h, we performed immediate surgery to control the abdominal hemorrhage caused by the mesenteric injury. Surgical findings revealed abdominal bleeding (900 mL blood) from the ileocecal branch of the mesenteric artery. The intestine was not perforated and did not require removal. We ligated the bleeding vessels and repaired the mesenterium by continuous sutures (Figure 4).

Skin bruising by seat belt in right lower abdominal wall.

Mesenteric injury was showed in contrast-enhanced computed tomography on arrival.
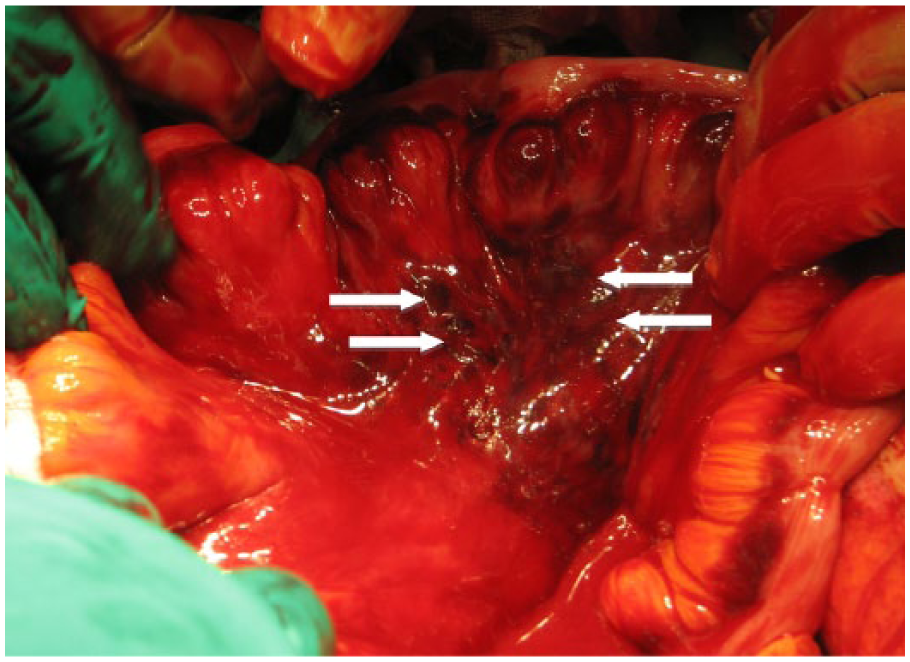
Intraoperative photo of this patient shows a 7-cm diameter laceration in the mesenterium and oozing from the ileocecal branch of the mesenteric artery.
The patient’s postoperative clinical course was smooth without any major sequelae, and he was discharged from the intensive care unit (ICU) 10 days after the surgery. After discharge from the ICU, however, we noticed that the patient showed Ventricular Tachycardia (VT) while putting on routine cardiac monitor. Therefore, we performed coronary angiography, which revealed stenosis in the left anterior descending coronary artery. The patient’s cerebral performance was judged as Category 1 according to the Glasgow–Pittsburgh Cerebral Performance Categories. 5
Discussion
In this case, arrhythmia (Vf) was considered as the major cause of CPA of this patient. He suffered from Vf which resulted in the traffic accident and blunt injury. We could not know the reasons of Vf and it might come from intrinsic disease, because there was no evidence of severe injury of cardiovascular structure, including myocardial depression. In other words, the patient had “CPA with BT” and not BT-CPA. The National Association of Emergency Medical Services (NAEMS) Physicians Standards and Clinical Practice Committee and the American College of Surgeons Committee on Trauma state that resuscitation efforts may be withheld or terminated for any BT patient who, based on out-of-hospital personnel’s thorough primary patient assessment, is found apneic, pulseless, and without organized ECG activity upon arrival of emergency medical services at the accident site. 6 In fact, we have not been able to resuscitate many cases of BT-CPA, and even if the patient’s spontaneous circulation returns to normal, he or she remains bedridden in most cases. Table 1 shows the review of the literature, and almost all cases of BT-CPA reveal miserable prognosis. Therefore, attempting CPR for patients with BT-CPA has been criticized as a futile and an inappropriate use of valued medical resources.8,9 Consequently, we sometimes hesitate to implement CPR in BT-CPA patients. However, this could be problematic because we may misdiagnose the causes of CPA. For example, Mushtaq and Ritchie 10 reported that out of 63 postmortem examinations performed by a forensic pathologist, 25 revealed inaccurate diagnoses (99% confidence interval: 24.3%–56.6%; p < 0.01) in the ED. Furthermore, numerous cases involving discrepancies between clinical diagnoses and autopsy findings have been reported.11,12 However, these BT-CPA cases can include “BT with CPA” patients. Actually, our patient might have possibility regard as trauma causing death if we cannot rescue him.
Various reports of the prognosis (survival rate and neurological outcome) of BT-CPA.
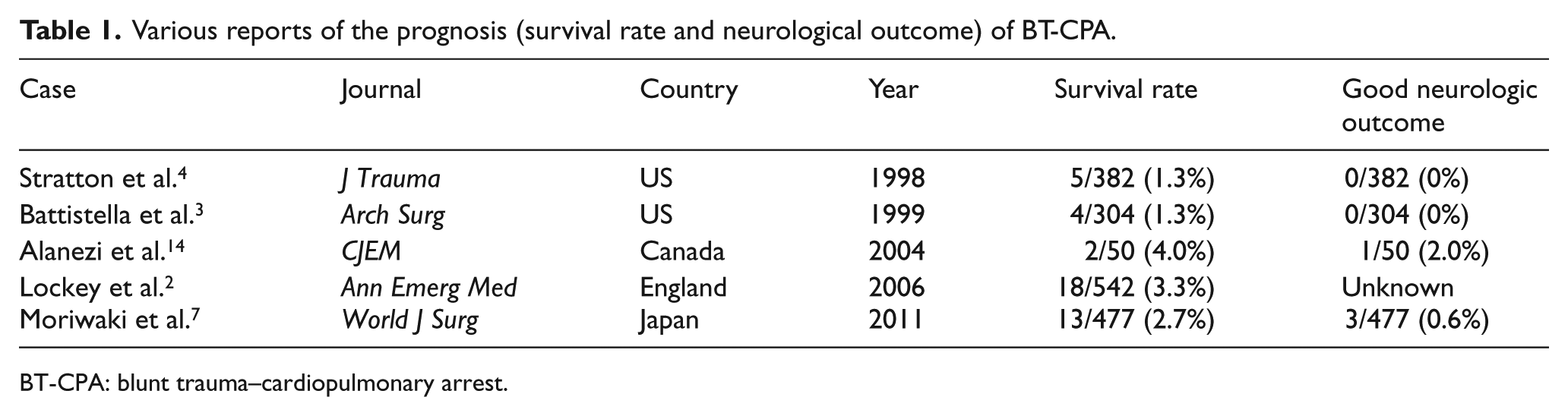
BT-CPA: blunt trauma–cardiopulmonary arrest.
Although the protocols of all institutions require rigorous examinations of all patients, a definitive diagnosis may not be achieved because of many complicating factors. For example, some patients diagnosed with CPA as a consequence of BT may be died of pre-existing disease or a disease that arose independently of the traumatic event. Therefore, we considered this possibility with respect to the case presented here and assessed this patient by ECG, ultrasound, and blood tests. The results did not reveal an ST change on the ECG, asynergy, or elevated levels of cardiac enzymes. Even though these data indicated that an ongoing disease was unlikely, we consulted a cardiologist as a precautionary measure. The cardiologist commented that the patient was not suffering from obvious cardiac disease. But 10 days after admission, pulseless ventricular tachycardia was detected on routine ECG. These findings indicate the importance of considering the possibility of pre-existing diseases while encountering patients with BT-CPA.
Another factor contributing to successful treatment is prioritizing the various treatment options. Ideally, the trauma and the cause of CPA must be simultaneously treated. It is important to evaluate the underlying problem: trauma or the cause of CPA. In the case presented here, trauma was the critical problem as indicated by worsening acidosis and accumulation of abdominal fluid; surgery was also performed accordingly. However, if this patient exhibited persistent Vf or other abnormal cardiac findings, it may be necessary to treat these first. Moreover, unstable conditions and the surgery itself may pose high risks to the patient and affect his survival. We often discuss the best timing of treatment or the most appropriate procedural priority to address the most life-threatening injury in polytrauma patients. 13 However, we rarely consider which one is more important: treating pre-existing disease or treating trauma. This is an important consideration in this present case. However, to our knowledge, few reports similar to ours have been published.
Finally, the above-mentioned guidelines 6 also state that traumatic CPA patients with a >15-min transport time to an ED or a trauma center after the arrest may be considered nonsalvageable, and termination of resuscitation should be considered in these patients. In the present case, the arrest time was estimated to be about 20 min, which means that if the 15-min termination guideline had been applied, our patient would have died. Furthermore, a lot of “BT with CPA” cases may be included in this guideline. Moriwaki also reported that the single surviving patient in his study (out of 477 BT-CPA patients) experienced more than 15 min of arrest time. Therefore, we completely agree with his recommendation of administering CPR for at least 20 min, and not 15 min, in BT-CPA cases. 7 We suggest that the timing of termination of CPR must be judged carefully even in cases of BT-CPA which have a very poor prognosis. In traumatic arrest with Vf, it may be due to a medical reason, and more prolonged and intensive resuscitation may be considered.
In future, we want to identify those patients with BT-CPA having a higher survival chance, so as to avoid meaningless CPR. Conducting aggressive CPR for all these patients would not be cost-effective. Prediction tool of survival in BT-CPA patients is needed.
Footnotes
Acknowledgements
We thank all the paramedics, emergency medical technicians, nurses, and physicians who assisted us in treating the patient. Y.K. conducted a search of the literature and wrote this manuscript. T.A. provided editorial commentary. Y.K., M.F., and I.K. participated in the care of this patient. I.K. is the chief director of the Department of Emergency Medicine and oversaw the editing process. All authors have read and approved the submitted version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Ethical approval
Ethical approval does not require in our institution because of a case report.