
Abstract
Introduction:
Increased femoral vein size may lead to a higher first pass success rate during central venous cannulation. The aim of this study was to evaluate the effects of body position on femoral vein anatomy for cannulation.
Methods:
This prospective study examined the femoral vein of healthy volunteers by ultrasound scanner. The changes in cross-sectional area and diameter of the femoral vein were evaluated. Right-sided measurements were taken at four different leg positions: neutral, frog leg, back-up, and back-up/frog leg position.
Results:
A total of 50 subjects were enrolled in the study. The mean femoral vein cross-sectional area were 0.57 ± 0.29 cm2, 0.90 ± 0.26 cm2, 1.05 ± 0.33 cm2, and 1.47 ± 0.34 cm2, and the mean femoral vein diameter were 0.75 ± 0.20 cm, 1.05 ± 0.28 cm, 1.25 ± 0.21 cm, and 1.46 ± 0.25 cm in order of neutral, back-up, frog leg, and back-up/frog leg position (p < 0.001).
Conclusion:
Performing the right femoral vein catheterization in back-up and frog leg position is associated with a greater cross-sectional area of the femoral vein.
Introduction
Central venous cannulation (CVC) is an important procedure for volume resuscitation, delivery of vasoactive medications, and hemodynamic monitoring. A national survey of intensivists and hospitalists reported that most common site of real-time ultrasound (US) guidance for CVC was the internal jugular vein. 1 Despite the higher risk of catheter-associated infection, physicians might prefer the femoral vein (FV) for CVC rather than the internal jugular or subclavian veins in patients with resuscitation procedures such as endotracheal intubation or chest compression.2,3 FV may be accessed for temporary hemodialysis, pacemaker placement, and inferior vena cava filter.4,5
Increasing the size of target vessel would likely increase the first pass success rate during CVC. 6 We hypothesized that a simple lower back elevation, achieved by placing a surgical positioner on the lower back (back-up position), would increase cross-sectional area (CSA) of the FV and thereby enhance FV exposure for cannulation.
We sought to evaluate the effects of the four different body positions including neutral, back-up, frog leg, and back-up/frog leg position on FV CSA and compare it by US scanner.
Materials and methods
Study design, setting, and population
We performed a prospective study using US scanner to determine the effect of the four different body positions on the CSA and diameter of the right FV between October 1 and 31 October 2015 at a tertiary academic hospital. A total of 50 healthy volunteers were enrolled. Exclusion criteria included any previous regional surgery or major trauma to the femoral vessels or any history of deep venous thrombosis. The institutional review board approved this study (IRB No. 2015-09-028-001), and all subjects provided written informed consent.
Subject positioning
The neutral position was achieved by placing the patient supine, and frog leg position was achieved by external rotation and abduction of the hip.7,8 For the back-up position, we placed a surgical positioner (Chest Roll Gel Positioner w/Foam Core 20″, 405×150×150 mm; Allen Medical, Acton, MA, USA) just above iliac crest (Figure 1). In addition to the back-up position, external rotation and abduction of the hip were used for the back-up/frog leg position.

Back-up position achieved by placement of a surgical positioner.
Methods of measurement
A single MyLabTM Seven (Esaote, Genoa, Italy) US scanner was used for evaluating right FV CSA and diameter. The site of right femoral venipuncture (1 to 2 cm below the midpoint of the inguinal ligament) by where a clinician would traditionally attempt cannulation of the FV7,9 was scanned transversely with a 13–4 MHz broadband linear probe (Esaote SL1543 Ultrasound Transducer) by a single emergency physician with the lightest possible pressure to decrease effect on the size of FV by the degree of compression.10,11US images were obtained in order of the neutral, back-up, frog leg, and back-up/frog leg position. To exclude the effects of respiratory fluctuations, maximal CSA and diameter were selected. Four positions were performed with a 1 min rest period between each position.
Outcomes
We measured right FV CSA, diameter, and exposed width which can be used to evaluate the potential impact of cannulation in clinical practice. 8 CSA (total area of FV) was measured automatically by US scanner and diameter was measured the longest distance of FV (Figure 2). Exposed width was measured FV length not overlapped by the femoral artery (FA). CSA, diameter, and exposed width were measured by a single intensivist.
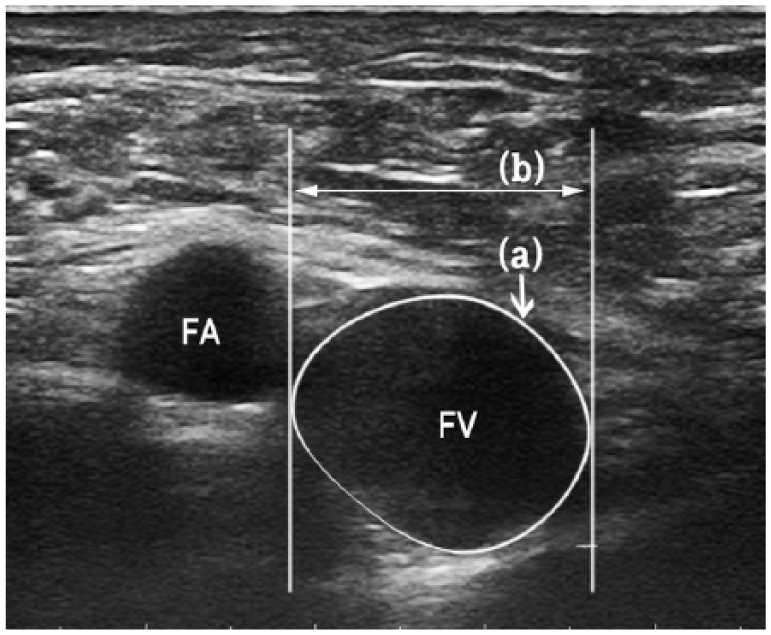
Ultrasound image for measuring (a) cross-sectional area (CSA) and (b) diameter of the right femoral vein.
Statistical analysis
All data are presented as means ± standard deviations (SDs). A one-way analysis of variance (ANOVA) was used to compare changes in FV CSA and diameter in the four different body positions. All statistical analyses were performed using SPSS software (version 18.0) for MS Windows (SPSS, Chicago, IL, USA). A p value less than 0.05 was considered significant.
Results
Demographics
A total of 50 subjects (25 males and 25 females) were enrolled. The mean age (±SD) was 26.1 ± 4.1 years, the average weight was 62.3 ± 12.1 kg, the average height was 167.5 ± 7.6 cm, and the average body mass index was 22.04 ± 3.19 kg/m2 (Table 1).
Demographic data.
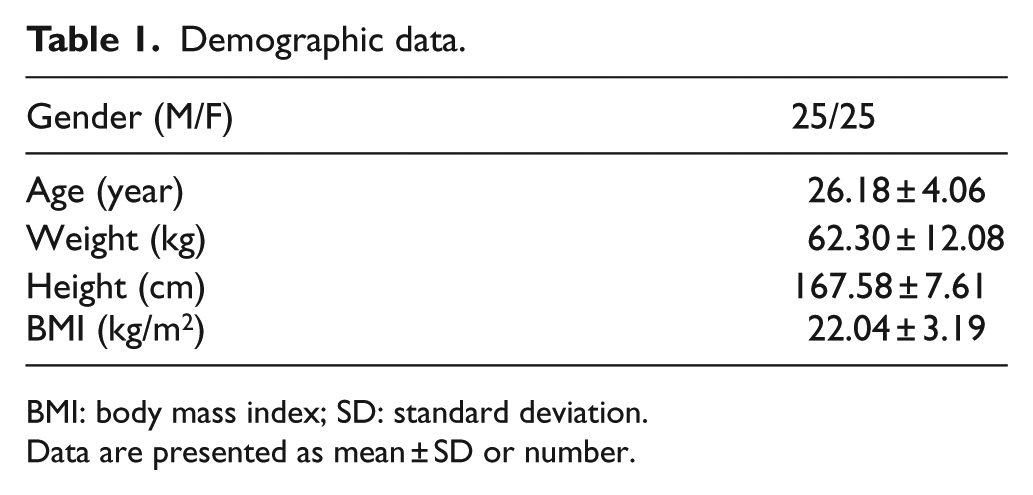
BMI: body mass index; SD: standard deviation.
Data are presented as mean ± SD or number.
CSA and diameter of FV in four different positions
The mean FV CSA were 0.57 ± 0.29 cm2, 0.90 ± 0.26 cm2, 1.05 ± 0.33 cm2, and 1.47 ± 0.34 cm2 and the mean FV diameter were 0.75 ± 0.20 cm, 1.05 ± 0.28 cm, 1.25 ± 0.21 cm, and 1.46 ± 0.25 cm in the order of neutral, back-up, frog leg, and back-up/frog leg position (p < 0.001; Table 2; Figure 3).
Cross-sectional area (CSA), diameter, and exposed width of the femoral vein (FV) in different anatomical positions.
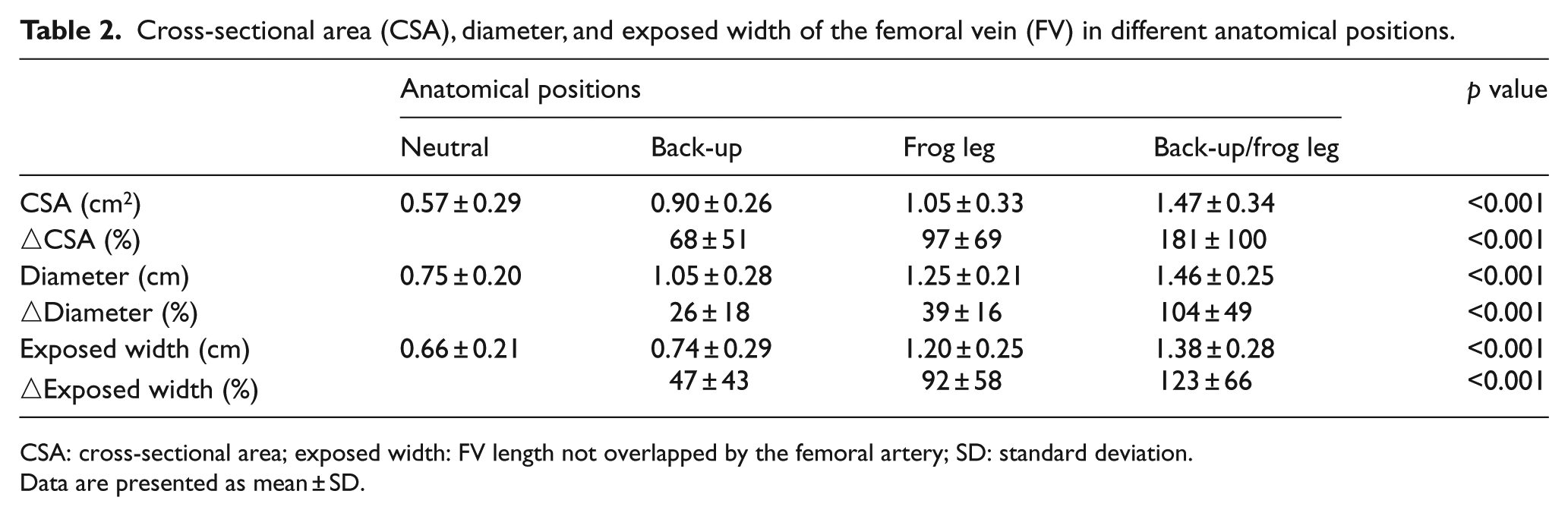
CSA: cross-sectional area; exposed width: FV length not overlapped by the femoral artery; SD: standard deviation.
Data are presented as mean ± SD.

Ultrasound images of the right femoral vein (white star) and femoral artery (yellow star) with the patient in different anatomical positions: (a) neutral position, (b) back-up position, (c) frog leg position, and (d) back-up/frog leg position.
Influence of back-up/frog leg position
Statistical analysis indicated that the mean CSA and diameter of the FV were significantly greater in the back-up, frog leg, and back-up/frog leg position than in the neutral position (p < 0.001). However, the back-up position provided less benefit than the frog leg position and the back-up/frog leg position (p < 0.001). The CSA and diameter of the FV increased in the order of neutral, back-up, frog leg, and back-up/frog leg position (p < 0.001; Figure 4).
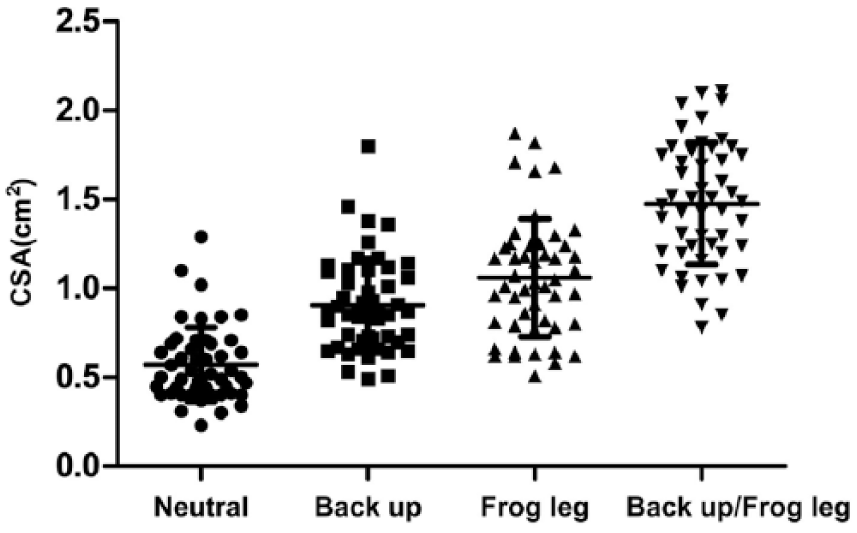
Scatter plot of the change in the cross-sectional area (CSA) of the right femoral vein in different anatomical positions. Data are presented as mean ± SD (95% confidence interval).
Discussion
Although US-guided catheter insertion is recommended for central vein access during the resuscitation period, CVC is still performed using surface landmarks for guidance.1,2,9 It is helpful to maximize the CSA and diameter of the FV for successful cannulation, regardless of US usage.8,12
Previous studies reported that certain dynamic maneuvers including hip abduction and external rotation (frog leg position), the Valsalva maneuver, and the reverse Trendelenburg position can increase the diameter of the FV and can be useful for avoiding vessel overlap in both pediatric and adult patients.13 –15 However, these maneuvers are not be applicable to all patients because the Valsalva maneuver and the reverse Trendelenburg position may not be possible or disadvantageous in patients with hemodynamic instability or with altered mental status.16 –18
Our results indicate that a simple bed-side elevation of the lower back with the frog leg position maximizes the diameter and CSA of the FV, and this position will increase the accessibility of the FV. Overlapping of the FV by the FA can lead to inadvertent arterial catheterization or arteriovenous fistula. The larger the exposed width of the FV is, the greater the chances of a successful FV cannulation without complications. 8 Although the reason for the superiority of the back-up/frog leg position remains unclear, we postulate that venous return from the abdominal and pelvic cavity might be decreased by back-up position, thus leading to a venous pooling effect.
This study has several limitations that might impact interpretation of the data. First, we examined healthy young adults, so the results may not be generalizable to acute critically ill patients. Although a randomized trial enrolling patients with shock or cardiopulmonary arrest can be challenging because of their need for urgent treatment, there is little harm in placing a pad underneath the patients back; therefore, further studies are needed whether this simple intervention would improve first pass success rate and time to placement and reduces complications. Second, this study only evaluated the right FV, and body position could have a different effect on the left FV. However, we chose to examine the right FV because two-third of FV cannulation are attempted in the right side. 19 Third, knowing the position of the patient could influence the imaging and measurement of the CSA and diameter of FV resulting bias. The frog leg and back-up position are hard to be blinded for the operator. Fourth, positive end expiratory pressure during mechanical ventilation can influence the CSA of FV, 11 and further research is warranted to answer to this question.
Conclusion
In this study, performing the right FV catheterization in back-up and frog leg positions is associated with a greater CSA of the FV. Our data suggest that future studies are needed to clarify this patient’s positioning would improve patient-oriented outcomes on critically ill patients.
Footnotes
Acknowledgements
J.W.L., H.J.A., K.D.K., J.H.K., and S.W.Y. were involved in the conception and design of the study, or acquisition of data, or analysis and interpretation of data. J.W.L., H.J.A., Y.I.S., and K.C.S. drafted the article or revised it critically for important intellectual content. All authors approved the final version to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
This study protocol was reviewed and approved by the Institutional Review Board of Chungnam National University Hospital (IRB No. 2015-09-028-001). Informed consent was submitted by all subjects when they were enrolled.