
Abstract
Background:
Child abuse occurs all over the world, including Hong Kong. The Accident and Emergency Department is one of the places in which cases of child abuse may present to.
Objectives:
As an emergency physician in the hospital, we need to understand the signs and symptoms and the risk factors of child abuse. We also need to perform risk assessment and formulate the plan of management.
Methods:
Databases in Hong Kong were searched to obtain the current situation of child abuse in Hong Kong. Literature about the nature of child abuse was also searched.
Results:
The epidemiology of child abuse in Hong Kong was reviewed. Signs and symptoms, risk factors, and management of child abuse were summarized in this review article. Conclusion: High vigilance is needed for emergency physicians to pick up cases of child abuse. Most cases of child abuse would finally need assessment from a multidisciplinary team.
Introduction and background
Definition
In modern society, the general belief is that the society should ensure that all children can grow and develop in a safe and healthy environment until they can cope with their own living. Support should be provided basically by their parents/guardians.
Child abuse happens all over the world. It can happen in both developing and developed countries. The definition of child abuse varies, and depends on the cultural environment of the specific region. In Hong Kong, child abuse is defined by the Social Welfare Department (SWD) as any act of commission or omission that endangers or impairs a child’s physical/psychological health and development of an individual under the age of 18. 1 Child abuse is not limited to child–parent/guardian situations but includes anyone entrusted with the care and control of a child, such as child-minders, relatives, teachers and so on. 2
The Laws of Hong Kong also protects a child from being abused. There are multiple ordinances existing for this purpose. For example, persons who offend Section 27 (ill-treatment or neglect by those in charge of child or young person) of Offences against the Person Ordinance (Cap 212) shall be guilty, and shall be liable to imprisonment. 3 There is also the Protection of Children and Juveniles Ordinance (Cap 213), which allows the child or juvenile who appears to be in need of care or protection to a place of refuge. 3
Category of child abuse
Child abuse can be divided into four categories: physical abuse, sexual abuse, neglect and emotional abuse. 1
Physical abuse, commonly known as non-accidental injuries, refers to any physical suffering/injuries inflicted onto the child by physical force. 1 It is the most common type of abuse. According to SWD statistics in 2017, physical abuse accounts for 39.5% of all abuse cases. 4 Common presentations of physical abuse include bruises, bite marks, lacerations and abrasions, burns and scalds, fractures, internal injuries such as head injuries and abdominal injuries.
Sexual abuse, the second commonest type of abuse, accounting for 33.3% of all cases in 2017, 4 is the involvement of a child in sexual activities. These include not only indecent assault and sexual intercourse directly on the child, but also inappropriate involvement of them in sexual contents such as exposing them to pornographies.
The child may present with behavioural problems such as poor peer relationship, unwilling to participate in physical activities, excessive reaction to being touched and sexual knowledge not corresponding to the age of child and so on. Physical symptoms and signs may include genital discomfort or pain, bruises or bleeding in the genital region, sexually transmitted disease and early adolescent pregnancy. However, absence of physical signs cannot rule out sexual abuse. A study has found that only 21.4% of sexually abused girls have positive physical findings if examined acutely, and a further lower percentage of positive findings (2.2%) if examined non-acutely. 5
Neglect is the lack of attention to the child repeatedly so that the child’s health or development is endangered. 1 Consistent failure to provide needs of the child in respect of physical (food, clothing, shelter, safe environment), medical, educational and emotional aspects can cause neglect to the child.
Emotional abuse or psychological abuse, is any behaviour and attitudes that endanger or impair the child’s emotional or intellectual development. 1 Clinical symptoms and signs can be vague in this type of abuse. For example, children may present with failure to thrive, speech disorder, anorexia nervosa, abnormal behaviours like strange habits, wetting/soiling, self-harm, conduct problems and so on. Sometimes, clues can be found in the interaction within the family, such as constant scolding, humiliating criticism or bizarre punishment. A high level of vigilance and fine observations are needed in order to identify these cases.
Risk factors
Generally speaking, risk factors for child abuse can be categorized as problems of the family, risk factors intrinsic to the child, and problems of the environment and society.
Family factors include young parents, female perpetrators, substance misuse problem, history of domestic abuse in the same family, emotional volatility, mental health problems, chronic parental stress, parent experienced abuse/neglect as a child and so on.6,7
Child factors mainly include premature babies 7 and disabled children. 6 Psychiatric illness of children, for example, attention deficit and hyperactivity disorder, also increase the risk of being abused. 8
Environmental factors include a feeling of poor social support by the parents. 7 Difficult macroeconomic status of the whole society also increases the rate of hospitalization for physical abuse of children. 9
Specific to the situation in Hong Kong, the SWD has summarized the risk factors for child abuse for professionals’ reference (Table 1).
Characteristics commonly associated with child abuse, summarized by the Social Welfare Department of Hong Kong SAR. 1

SAR: Special Administrative Region.
Current situation in Hong Kong
Epidemiology
Child abuse is a medical as well as a social issue. Cases of child abuse are referred to and registered under the SWD through different means. Some children would have been picked up by a teacher/social worker when familial problems arise. Others may present to the Accident and Emergency Department (A&E) when injuries have already happened, or when emotions are significantly disturbed. Occasionally, the children may be brought to the A&E severely injured or dead.
A brief review of the local epidemiology and incidence of child abuse was performed. Data of child abuse were retrieved from registries and databases, including the Newly Reported Child Abuse Cases by the SWD, the A&E Information System (AEIS) and the Clinical Data Analysis and Record System (CDARS) of the Hospital Authority of the Hong Kong Special Administrative Region (HKSAR).
Statistics from the SWD showed that there were 947 reported cases of child abuse in Hong Kong in 2017. 4 The most common abuser was the parents (59.4%; Table 2). There have been generally more female victims than male victims in the past few years in Hong Kong. From 2012 to 2017, the percentage of female and male victims averaged 58.4% (55.7%–63.4%) and 41.6% (36.6%–44.3%), respectively.4,10–14 There were no major changes in the gender ratio through recent years.
Newly reported child abuse cases from January to December 2017, by Social Welfare Department of Hong Kong SAR. 4
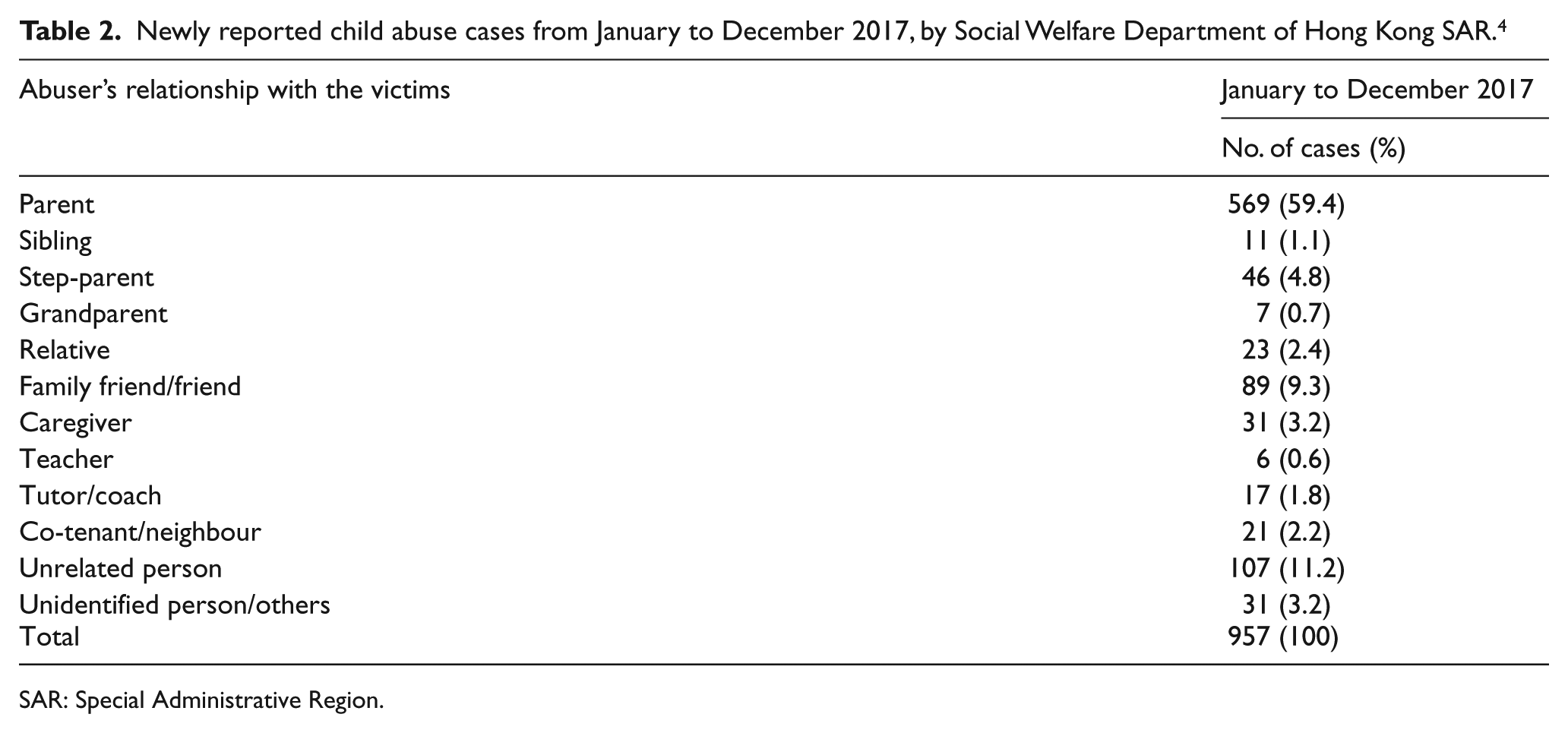
SAR: Special Administrative Region.
Distribution of cases of child abuse among 18 districts in Hong Kong was also reported. From the years 2005 to 2017, 15 Yuen Long district ranked the highest proportion of child abuse cases reported (Table 3). Corresponding to this result, the A&E attendance for child abuse (per 10,000 paediatric attendance) is also the highest in the New Territories West Cluster (NTWC; Figure 1), which serves Yuen Long, Tuen Mun and Tin Shui Wai.
Reported cases of child abuse in Hong Kong by district (Top 3). 15
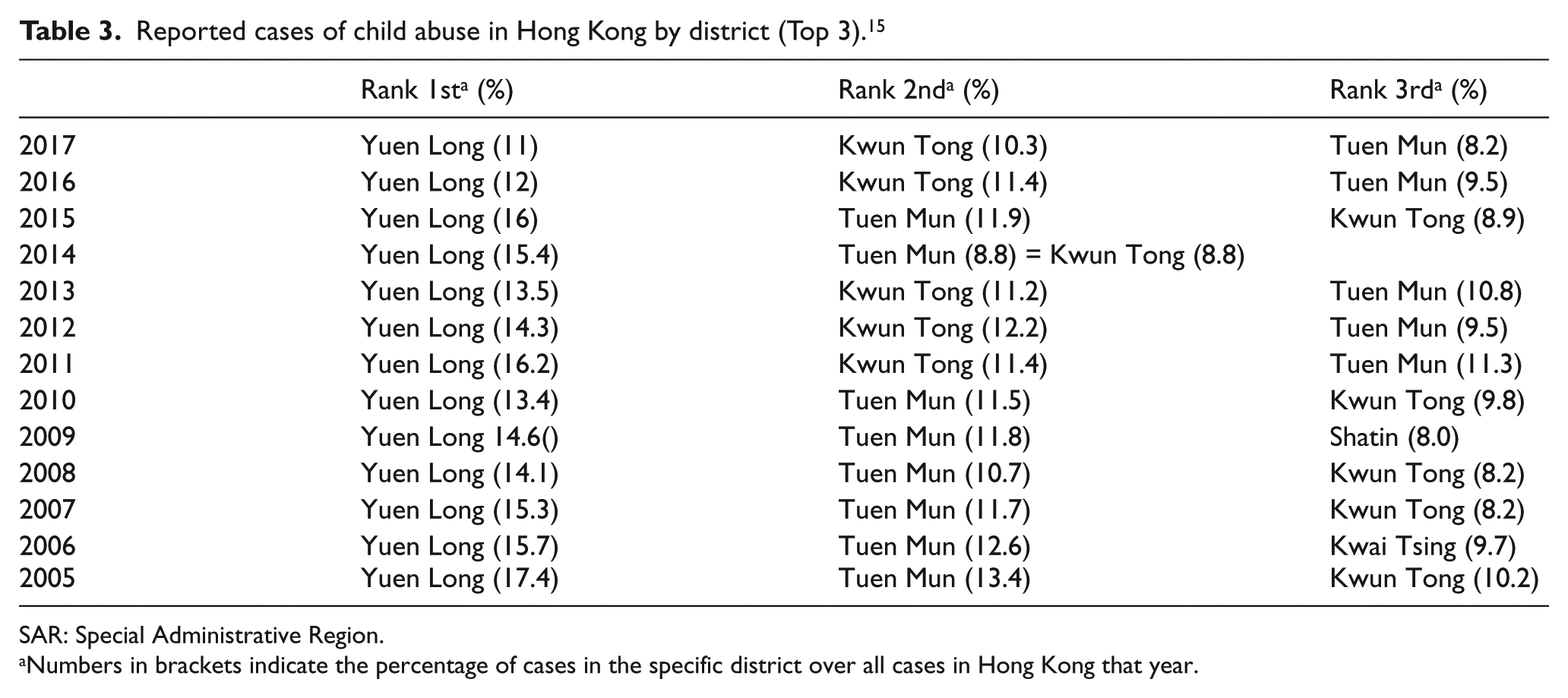
SAR: Special Administrative Region.
Numbers in brackets indicate the percentage of cases in the specific district over all cases in Hong Kong that year.
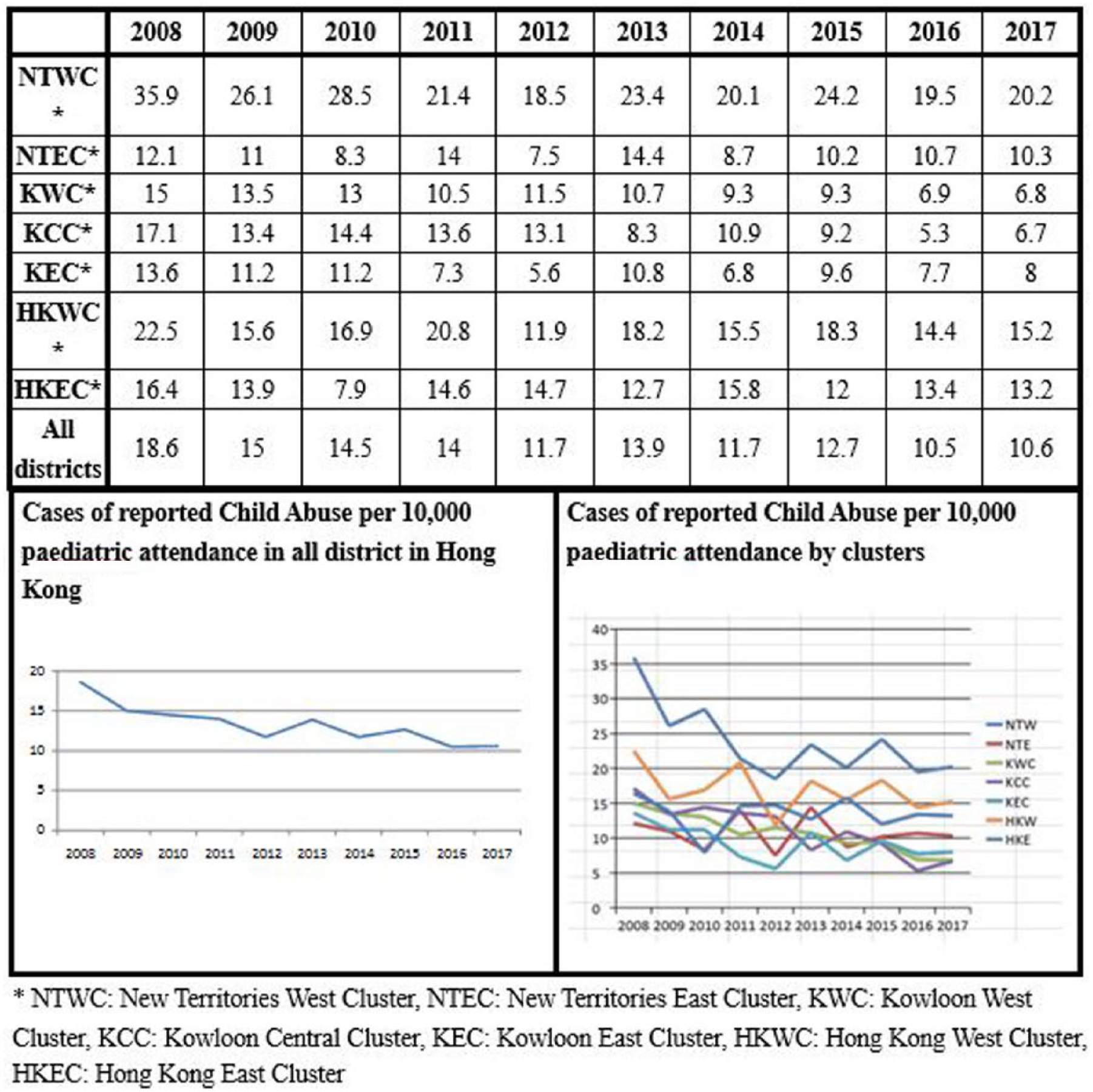
Cases of reported child abuse per 10,000 paediatric attendance by different clusters in Hong Kong.
Among all the cases of child abuse reported to the SWD, not all cases were presented to the A&E. The number of cases that were brought to the A&E consisted of about one-third of all reported cases (Table 4). The remaining two-thirds were referred to the SWD by different routes such as direct referral to social workers by school teachers.
Number of child abuse cases reported/registered by different organizations in Hong Kong SAR from 2008 to 2017.
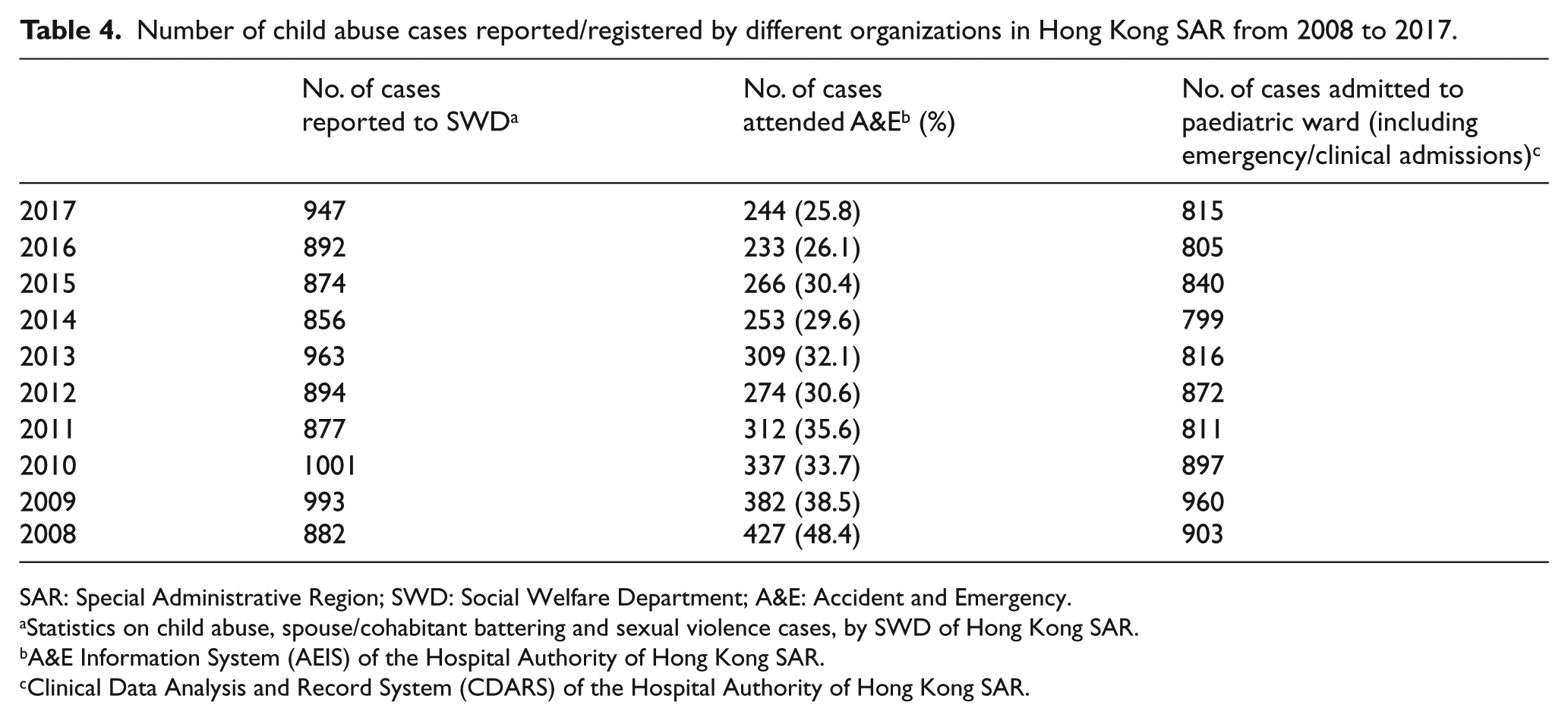
SAR: Special Administrative Region; SWD: Social Welfare Department; A&E: Accident and Emergency.
Statistics on child abuse, spouse/cohabitant battering and sexual violence cases, by SWD of Hong Kong SAR.
A&E Information System (AEIS) of the Hospital Authority of Hong Kong SAR.
Clinical Data Analysis and Record System (CDARS) of the Hospital Authority of Hong Kong SAR.
From the perspective of A&E, cases of child abuse are presented with different chief complaints and the children were triaged into five categories according to their clinical condition. Category 1 (Critical) and category 2 (Emergency) patients are those suffering from a life-threatening or potential life-threatening condition(s) with unstable/borderline vital signs requiring immediate/emergency treatment in resuscitation room. Category 3 (Urgent) patients are those who suffer from a major condition with potential risk of deterioration despite stable vital signs. Category 4 (Semi-urgent) and Category 5 (Non-urgent) patients are those whose condition and vital signs are stable such that they can afford to wait some time.
During the year from 2015 to 2017, there were 753 reported cases of child abuse in all 18 A&E in Hong Kong. A total of 5 cases (0.7%) were triaged as categories 1 and 2 where resuscitation was required, 469 cases (62.3%) were category 3 and 279 cases were categories 4 and 5 (37.1%).
Interestingly, the male to female ratio is somewhat different from the statistics by SWD. Data retrieved from the Hospital Authority showed that during 2015–2017, male patients contributed to 52.7% of all A&E cases, while the data from SWD showed only 41.6% of cases were male victims. This may be due to more significant injuries to male patients in cases of abuse, leading to proportionally more attendance to A&E.
Over the past years, there was a gradual declining trend in the number of child abuse cases attending A&E (Table 4). For every 10,000 paediatric attendance in all A&Es in Hong Kong, the number of cases of child abuse dropped from 18.6 to 10.6 from 2008 to 2017. However, the number of cases of child abuse reported to SWD has mildly increased in the past years. The estimated paediatric population in Hong Kong was retrieved from the population census (Table 5). The incidence of child abuse per 10,000 paediatric population had mildly increased from 6.68 to 8.78 (Table 5). With an increasing incidence rate noted in the SWD registry but a decreasing trend in A&E attendance, the reasons behind may be contributed by an increasing rate of case pickup and reporting from the society/school before significant injuries happened. This may also explain the decreasing number of admissions due to child abuse in paediatric wards.
Cases of child abuse per 10,000 paediatric population in Hong Kong SAR.
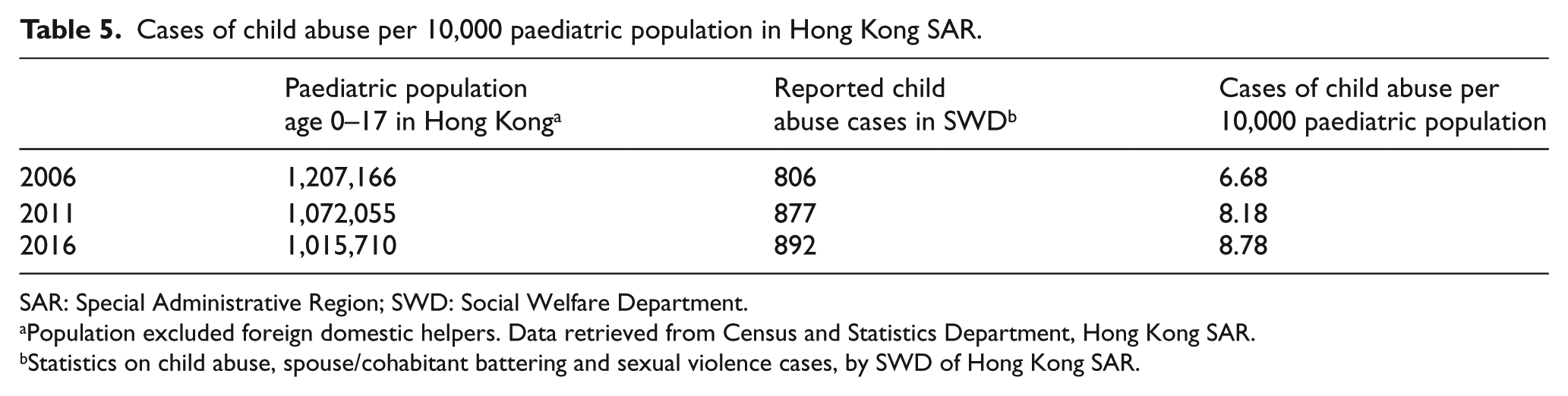
SAR: Special Administrative Region; SWD: Social Welfare Department.
Population excluded foreign domestic helpers. Data retrieved from Census and Statistics Department, Hong Kong SAR.
Statistics on child abuse, spouse/cohabitant battering and sexual violence cases, by SWD of Hong Kong SAR.
Statistics of child abuse were also reported in other cities in Southeast Asia, but most of the reported data are the absolute number of abuse cases. Only Taiwan has reported the number of cases of child abuse based on paediatric population. The incidence of child abuse was 0.40% in 2010. 16
Role of emergency physicians – approach to suspected child abuse
Correct diagnosis
Management of child abuse in the A&E is a clinical challenge. Multiple aspects should be addressed. First, making a diagnosis of child abuse is not an easy task. This requires a comprehensive history and physical examination of the child, the parents, the relatives or other associated personnel. Hidden agenda are often present, especially in those cases in which the abuse is mild or the abuser is the caretaker themselves.
Children who suffer from child abuse can present to A&E in various manners. If the children are brought to the hospital by the police, social worker or teacher, it would usually be obvious that the children are suffering from abuse. However, the diagnosis of child abuse may sometimes be difficult. Children may be brought to the hospital by parents for non-specific complaints, such as withdrawal of communication, oppositional behaviour, inconsolable crying, temper tantrum, eating disorders, developmental delay and so on. 6
History
History taking in suspected case of child abuse requires some specific technique. Direct confrontation with the suspected abuser should be avoided. Open-ended questions should be asked to the victim. History taken from the child may be more accurate if the parents/abusers are not present.
Histories suggestive of child abuse include vague description of the incident, inconsistent history from different relatives or injury not compatible with the history described. Apart from the content of the history, other clues such as interaction between the suspected abuser and the child, and the emotion of the family should also be noted. The risk of child abuse may be higher if there is excessive scolding of child during consultation, overwhelming parental control, fearful expression of children when talking, or abnormally calm parents which does not correspond to the severity of disease in the children.
For the content of the history, cultural variations and social background should be considered. For example, children in Chinese society are generally more dependent while those in Western societies are more independent. Therefore, the cultural standard of ‘neglect’ would be different. Similarly, traditional Chinese families may consider appropriately limited physical punishment as a method of teaching. The ‘definition’ of physical abuse may be somewhat different from Western society.
Physical examination
Non-accidental injuries, although alarming to the clinician, are much less common than accidental injuries. Therefore, it is important to identify those injuries that are inflicted on purpose of abuse from those accidents. Classically, injuries that may indicate non-accidental injuries 17 include fractures under 1 year old, injuries to mouth such as torn frenulum, bruises of different age and specific marks such as patterned marks of offending object/grasp marks/cigarettes, burns over genitalia and scald in glove and stock pattern. Signs and symptoms of inflicted traumatic brain injury include retinal haemorrhage, decreased Glasgow Coma Scale and seizure and so on. In contrast to abusive head injuries, accidental head injuries commonly present with local scalp swelling or parental concern of an asymptomatic child. 18
However, many a time the physical findings are not clear-cut. Typical signs of child abuse may not be present in every case, especially those children who are not yet being abused to a significant extent. On the other hand, presence of ‘typical’ signs is not the same in child abuse. Some well-known diseases which mimic abusive injuries include osteogenesis imperfecta, bleeding disorder, Mongolian spots, vasculitis, dermatological diseases and so on. Vaginal discharge/laceration can be due to sexual abuse, but the differential diagnoses of vaginitis or accidental straddle injury should always be in mind. Furthermore, ‘inflicted’ injuries may not necessarily be due to abuse. For example, in the Chinese society, traditional treatment such as cupping or spooning may cause multiple bruises over the body. Therefore, physical examination alone is not adequate in ruling in or ruling out child abuse. Integration with a comprehensive history is frequently needed.
Mental state examination
Mental state examination, although less commonly being discussed, is still an important aspect in the assessment. One type of child abuse is the psychological abuse, or emotional abuse. Some abnormalities may be noted in mental state examination, including blunted affect of the child or the parents, excessive anxiety of the child, poor emotional interaction between the parents and the child and so on. Sometimes the children may even demonstrate an idea of self-harm/suicide. A list of signs and symptoms, together with associated factors, is suggested by the SWD to aid in identification of victims for professionals dealing with child abuse (Table 6).
Common clinical presentation of child abuse, 1 summarized by the Social Welfare Department of Hong Kong SAR.
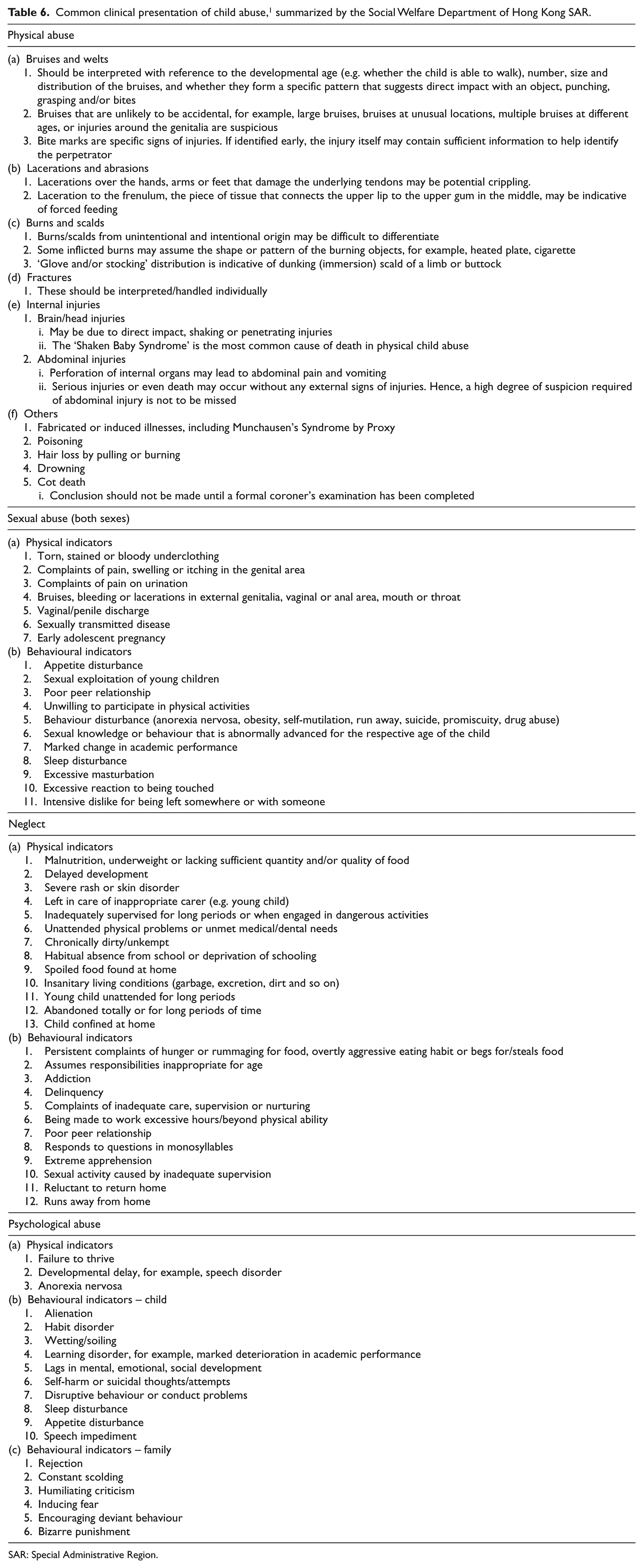
SAR: Special Administrative Region.
Management overview
Cases of child abuse are generally managed in cooperation with different specialties. Commonly, this would involve social workers, paediatric doctors and the police. Many cases of child abuse are nowadays being picked up by school teachers/social workers. These cases would usually be referred directly to paediatric departments and the police for further cooperative management. Emergency physicians, on the other hand, are sometimes the ‘first-touch’ personnel, or as a referral target for cases suffered from injuries. The main role of emergency physicians is to identify cases of suspected child abuse and to arrange further assessment for the victims.
Notifying the parents
The first step after making the diagnosis of child abuse would be to inform the parents. This may be easy if the abuser is any personnel other than the parents. They would usually assist and cooperate in these cases. The most problematic situation is when the suspected abuser is the parents themselves. As discussed above, the most common abusers in Hong Kong are parents. The parents may deny abusing the child, and refusing further help or referrals. Therefore, maintaining good rapport with the parents during consultation is needed. In situations where there is disagreement in management of the suspected abused kids between the physicians and the parents, consideration should be sought for the best interest and welfare of the kid. Early involvement of child abuse experts, social workers and police may be necessary.
Disposal plan
Not all cases of child abuse require admission. Unnecessary detention of the child in hospital may cause secondary psychological trauma to the child. From hospital databases, the admission rate averaged about 80.5% from 2015 to 2017 for A&E attendance of child abuse. Discharge with follow-up can be arranged if a safe environment is ensured, for example, the child can be taken to a place away from the suspected abuser, under the care of responsible personnel. Before discharging such cases, prior contact with the paediatric team for follow-up would be ideal. Contact information about the patient such as telephone number, school and class should also be obtained and confirmed so that the child can be traced if the child did not return for follow-up.
Admission is usually required when there are significant physical/psychological problems that need to be treated without delay. These include large wounds, fractures, unstable emotions and so on. Admission may be necessary if the risk of further abuse is high, and there is no safe environment readily available for the child after discharge. As suggested by the SWD, there are multiple factors that should be considered when assessing the risk of child (Table 7). Some of the factors that should be considered include characteristics of the precipitating incident, assessment of the physical and mental status of the child and assessment on the mental status of the caretaker.
Risk assessment for cases of child abuse, suggested by the Social Welfare Department of Hong Kong SAR. 1
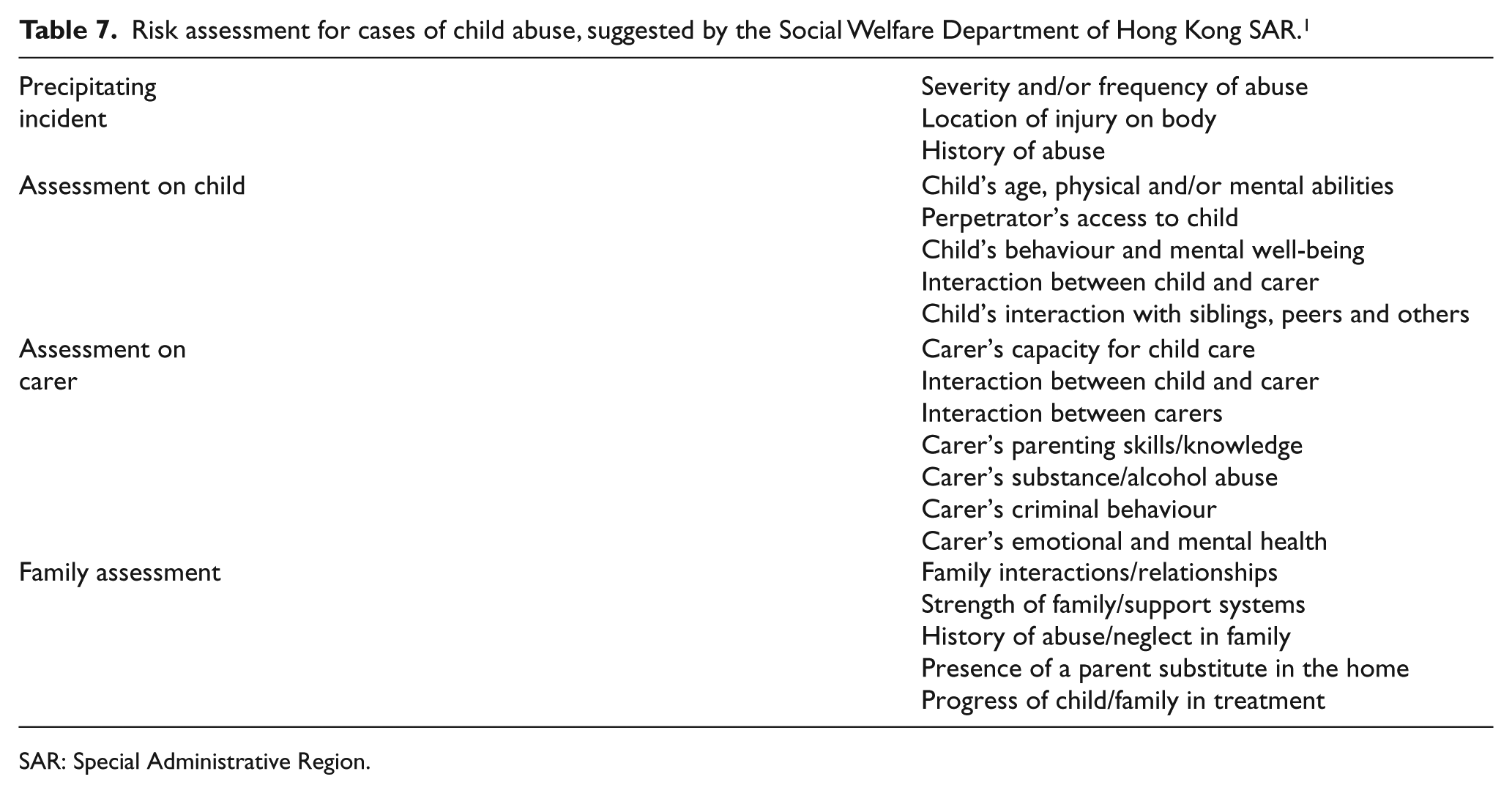
SAR: Special Administrative Region.
If the parents/guardians refuse admission despite explanation and persuasion, and there is a substantial risk to the child, social worker and the medical coordinator of child abuse should be involved early for a proper management plan. As a last resort to protect the child, under the Protection of Children and Juvenile Ordinance (Cap 213), the child can be detained in the hospital against parents’/guardians’ wishes. The police may also assist in enforcing the law.
Investigations
Investigations should be performed according to the clinical findings. Imaging for the severity and extent of injuries can be arranged, for example, X-rays, skeletal survey, computed tomography (CT) or magnetic resonance imaging (MRI) scans and so on. Blood test may also be ordered, for example, clotting profile to rule out coagulopathy causing multiple bruises. Consultation with paediatric team may be needed to rule out other potential causes such as osteogenesis imperfecta, vasculitis and so on.
Physical management
This is relatively straightforward. Treatment should be given to the victims according to the injuries. For example, splinting and orthopaedic opinion may be sought for fractures, and wounds should be managed and dressed. If necessary, consultation to wound nurse/surgeon may be appropriate.
Social and psychological management – multidisciplinary case conference on protection of child with suspected abuse
Child abuse is a complicated problem. Children are persons who are not expected to be able to take care of themselves completely. Since abusers are commonly the primary caretakers of the children, for example, parents, 4 management cannot simply depend on the parents. Therefore, different professionals are usually involved in caretaking of the victim.
Cases of child abuse can be referred to the multidisciplinary case conference (MDCC) by emergency physicians, usually through consultation with paediatricians of the hospital. Meanwhile, child abuse cases may also be referred to the MDCC directly by social workers if the child’s physical/mental status does not warrant A&E attendance (Table 4), for example, absence of significant physical injuries. Cases of child abuse with less acute physical injuries may also be directly brought to the paediatric team by social workers for assessment.
Typically, the conference is held within 10 days. 1 The conference will include social workers, family members, medical personnel, clinical psychologist, school personnel, police officers and professionals currently providing services to the child or the family and other professionals who may get involved in the future. 1
In the MDCC, a case manager, usually the social worker in charge, would be appointed. 1 He/she would be primarily responsible for communicating with the child. This aims to reduce the stress of the child as the victim would only need to interact with the case manager most of the time. The case manager would then coordinate with other professionals for a comprehensive plan. The role of the social worker would also include formulating a plan for the child on the social aspects. Examples would include housing problems, school problems, or financial problems and so on.
Medical Coordinators on Child Abuse (MCCA) are doctors designated by the Paediatrics Department in hospitals under the Hospital Authority for handling child abuse cases. 1 The duty of MCCA is to provide medical service to child abuse cases, assist admission of victims to hospital if needed, provide expert medical advice and coordinate different agencies through the assistance of medical social workers (MSW).
Psychologically, as child abuse usually involves a tragic experience, for example, injured by their own close relatives or parents, clinical psychologists may be consulted.
If criminal offences are involved, the police may take part in evidence collection and law enforcement. Forensic examination may also be needed in specific cases, such as sexual abuse.
Prevention of child abuse
The most effective way of dealing with child abuse is prevention. Prevention of child abuse can be categorized into different levels. Primary prevention would include proper education of parenting technique, promoting channels of help seeking in the society, arranging home visits and offering help to those families with higher risk, for example, parents being illicit drug users, young parents, parents with mental illness, child having long-term illness, high parental stress and so on.
Secondary prevention is to identify those children who had suffered from mild abuse, or are being treated sub-optimally. This mainly depends on personnel that often have contact with the children for example, teachers. Training programmes should be arranged for teachers so that school teachers can learn more about the signs and symptoms of an abused child.
Apart from teachers, emergency physicians or primary care doctors may also play a role as children who are suffering from mild maltreatment may be brought to the A&E or clinics for seemingly unrelated symptoms, for example, insomnia, poor concentration, non-specific abdominal pain and so on. High vigilance of the attending physician may help to identify early cases of child abuse so that prompt assessment and help can be offered and serious consequences avoided. Secondary prevention also applies to children who have siblings suffering from child abuse. As the risk is high for these cases, prompt assessment of the siblings should be arranged when a case of child abuse is suspected/established.
Tertiary prevention, which aims to minimize further harm to the child after established cases of child abuse, mainly depends on the work of social workers. These include arranging care of the child under a safe and responsible adult, for example, relatives, proper use of social resources of child care, or the use of Protection of Children and Juveniles Ordinance to keep the child by social worker/police in a safe place against the wishes of the parents/guardians. Proper treatment for physical and mental problems can also reduce further harm to the victim.
Screening tools for child abuse have been developed and investigated around the world. However, multiple reviews suggest that these screening tools still cannot achieve a significant clinical use.19–21 Development of a more accurate screening tool is needed before massive screening can be done for children.
Instead of a universal screening tool, different countries have different society guidelines in screening for suspected child abuse, followed by a preset protocol of management. For example, there is a National Institute for Health and Care Excellence (NICE) guideline in the United Kingdom on child abuse, 22 and a guideline from the American Academy of Pediatrics in the United States. 23 In Hong Kong, a procedural guide for handling child abuse cases (revised 2015) is available in the SWD. The guide includes basic knowledge of child abuse, handling of referrals and enquiries, investigation, roles of relevant departments/organizations and so on.
Conclusion
Child abuse is a medical as well as a social problem. For an emergency physician, an abused child being brought to the A&E is occasionally seen. Not all cases of child abuse have obvious injuries, and a high vigilance on suspecting child abuse is needed to pick up cases early before significant harm is done to the child. A well-taken history with proper physical examination is needed. If child abuse is suspected, care must be taken before discharging the child back home. However, we should bear in mind that unnecessary admission may cause secondary psychological trauma to the child. Referral to a multidisciplinary team is needed for further assessment and management.
Footnotes
Acknowledgements
All authors had fulfilled the requirement by the ICMJE definition of authorship, including substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; AND drafting the work or revising it critically for important intellectual content; AND final approval of the version to be published; AND agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.