
Abstract
Background:
Nonoperative management for hemodynamically stable splenic injury has been accepted as appropriate treatment. Objectives: This study aimed to investigate the changes in management and clinical outcomes of splenic injury by introducing a protocol for splenic injury at a newly established regional trauma center.
Methods:
From January 2005 to December 2016, we reviewed the outcomes of all 257 patients who sustained blunt trauma to the spleen at the first regional trauma center in South Korea. This 11-year period was divided into two intervals, before 1 January 2014 (period I, n = 189 patients) and after 1 January 2014 (period II, n = 68 patients), when the trauma center was established and a formal management protocol was followed for patients with blunt traumatic splenic injuries.
Results:
The proportion of emergency operations performed for patients with more serious (grades 3–5) splenic injuries was lower in period II than in period I (29% vs 22%, respectively, p < 0.001) whereas the rate of angioembolization was higher (89% vs 39.0%, respectively, p < 0.001). The time to intervention, irrespective of whether emergency operation or angioembolization was performed, was shorter in period II than in period I (312.8 min vs 129 min, respectively, p = 0.001). A greater proportion of patients was managed non-operatively in period II (78% vs 71%), and the non-operative management success rate was higher in period II than it was in period I (100% vs 83%; p = 0.014). Similarly, the splenic salvage rate was higher in period II (78% vs 59%, p = 0.03).
Conclusion:
After establishing a regional trauma center and introducing a protocol for the management of blunt splenic injuries, the rates of non-operative management and splenic salvage improved significantly. The reasons for this may be multifactorial, being related to the early involvement of a trauma surgeon, expansion of angiographic facilities and resources, and the introduction and application of a protocol for managing blunt splenic injury.
Background
Over the past 30 years, non-operative management (NOM) has generally been accepted as appropriate treatment for hemodynamically stable patients with blunt splenic injuries. The advantage of NOM is that it preserves splenic function, avoids overwhelming post-splenectomy sepsis, and decreases the risk of complications associated with operative splenectomy.1–4 Appropriate patient selection is important for the success of NOM, and controversy over these criteria still exists. Although many studies have shown that angioembolization of the bleeding splenic artery enhances the success rate of NOM in high-grade splenic injury, there are no clear criteria regarding which patients should undergo angioembolization, and the protocols and execution rates differ between centers. 5
The purpose of this study was to investigate changes in the management and outcomes of adult patients with blunt splenic injury after our major trauma center introduced and followed a protocol for blunt splenic injury.
Materials and methods
The data of patients managed for blunt splenic injury at our trauma center between January 2005 and December 2016 were retrospectively reviewed. We excluded patients aged < 15 years and those who had a cardiac arrest at the scene of injury or during transit to our emergency department. Splenic injury was diagnosed by computed tomography (CT) at our hospital or at a previous hospital. The diagnosis was confirmed by our radiologist or staff trauma surgeon and graded according to the Organ Injury Scale of the American Association for Surgery of Trauma. The trauma surgeon confirmed the grade of injury by reviewing both the surgical findings and the pathologic report in cases in which the spleen was removed.
The study period was divided into two periods: before (period I) and after (period II) 1 January 2014, when the trauma center was designated a regional trauma center. The Ministry of Health and Welfare in South Korea has started a project to establish a nationwide trauma system. 6 The primary goal was to establish a regional trauma center; such a center was formally opened at our hospital in January 2014—it is South Korea’s first trauma center. The trauma center is equipped with a trauma bay, two dedicated operating rooms for trauma patients only, a 20-bed trauma intensive care unit (ICU), a trauma intervention room, and a staff of dedicated trauma surgeons. The operating rooms and angiography suite are not used for elective procedures. Trauma surgeons are paid by the government; they manage only trauma patients and work in 24 h shifts. The trauma center is staffed 365 days a year. Our trauma center is properly equipped following the standard of level I trauma centers in the United States, with 14 full-time trauma surgeons, 2 trauma coordinators, and 7 physician extenders currently employed. Emergency physicians and an anesthesiologist stay at the center, and neurosurgery and orthopedic consultants are available round-the-clock. At this point, a new protocol for patients with splenic injury was also developed. This protocol was based on Eastern Association for the Surgery of Trauma practice management guideline and was modified for our hospital. 7
During period I, trauma patients underwent an initial assessment by an emergency medicine physician in the emergency room. When the emergency medicine physician found a splenic injury, the general surgery physicians were called to assess the patient. Hemodynamically unstable patients underwent exploratory laparotomy, whereas hemodynamically stable patients were admitted to ICU for bed rest, continuous monitoring of vital signs, and frequent monitoring of hematocrit. For these patients, serial abdominal examinations were performed as part of standard NOM. Delayed splenectomy—defined as splenectomy performed >12 h after admission—was performed when persistent bleeding was suspected. At the beginning of period I, it was not possible to perform angioembolization of the bleeding splenic artery, but this capacity was available for some patients after 2008.
In period II, the initial assessment was performed in the trauma bay. The patient was initially examined by both a trauma surgeon and an emergency medicine physician. Hemodynamically unstable patients underwent immediate splenectomy in one of the dedicated operating rooms. The indication for angioembolization was determined by the CT grade and the presence of extravasation of the intravenous contrast agent if the patient was stable. When the trauma center was established, emergent access to the angiography facility was secured for trauma patients. Three radiologists are on call at all times and are immediately available; hence, it is possible to perform angioembolization whenever needed. NOM was performed in the same way as it was in period I, and angioembolization was chosen as first-line management even in patients with persistent bleeding or re-bleeding. These criteria were implemented and followed, as per the new protocol (Figure 1).
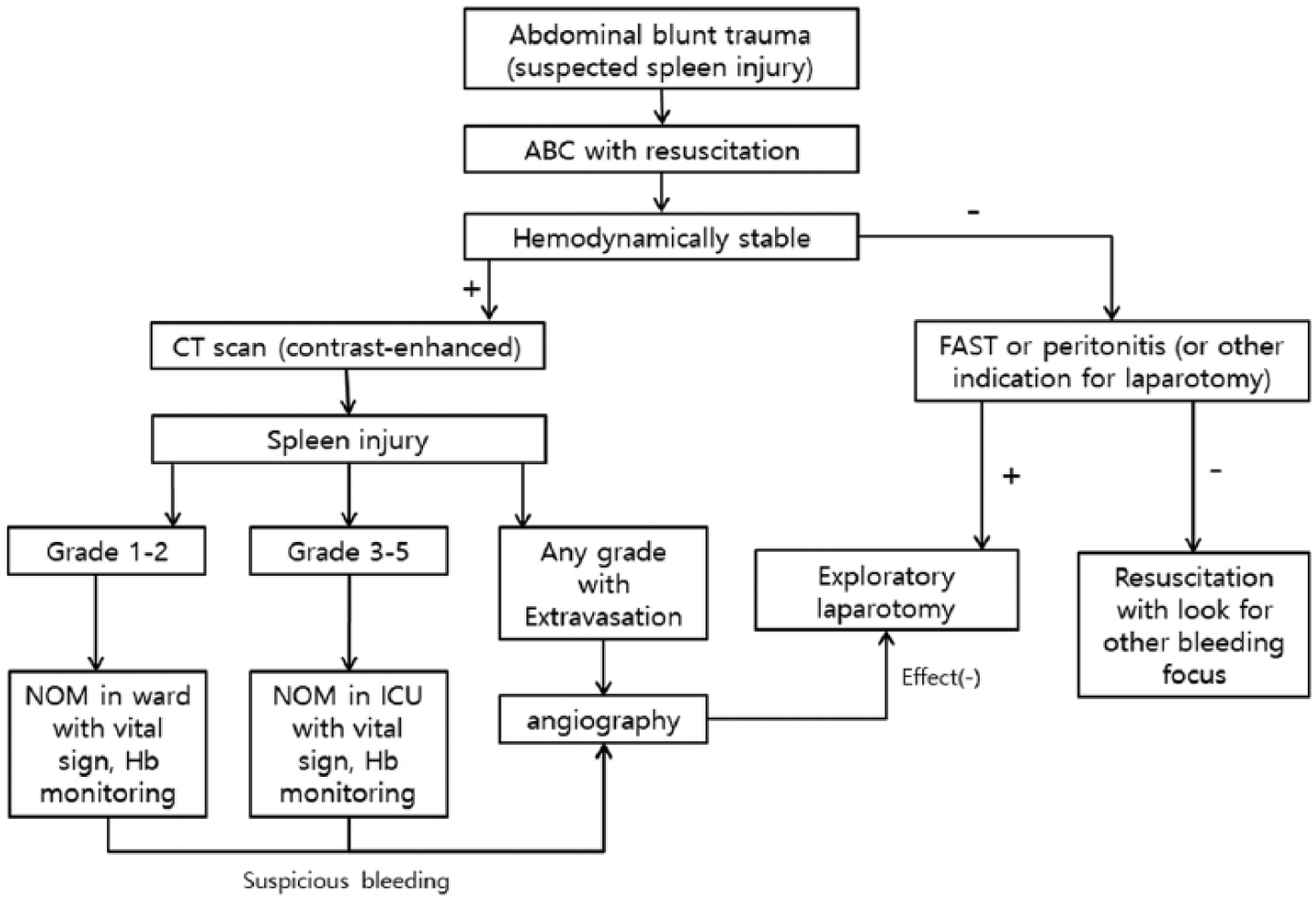
Protocol for the management of blunt traumatic splenic injury.
The patients’ medical records were retrospectively reviewed, and the following data were collected: sex, age, mechanism of trauma, initial vital signs, laboratory findings, grade of splenic injury, injury severity score (ISS), type and success of management, and mortality.
A univariate analysis was performed using Student’s t-test for continuous variables and the χ2 test for categorical variables. Logistic regression was used to examine risk factors associated with splenic resection. During logistic regression, we performed univariate analysis for each predictor and then performed multivariate analysis on the meaningful predictors. Statistical significance was set at p < 0.05. All statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
Results
During the study period, 299 patients were managed for blunt traumatic splenic injury. After exclusions, the data of 257 patients were analyzed (Table 1). There were no differences between the patients managed during periods I and II in terms of age, sex distribution, mechanism of injury, systolic blood pressure at the time of admission, and laboratory findings. However, the ISS was significantly higher in period II than in period I (22.5 vs 17.6, respectively, p = 0.038). The overall distribution of patients by grade of injury was as follows: grade 1, 15.2%; grade 2, 33.1%; grade 3, 31.5%; grade 4, 16.0%; and grade 5, 4.3%, with no difference in distribution between periods I and II.
Comparison of patient demographics between the two periods.
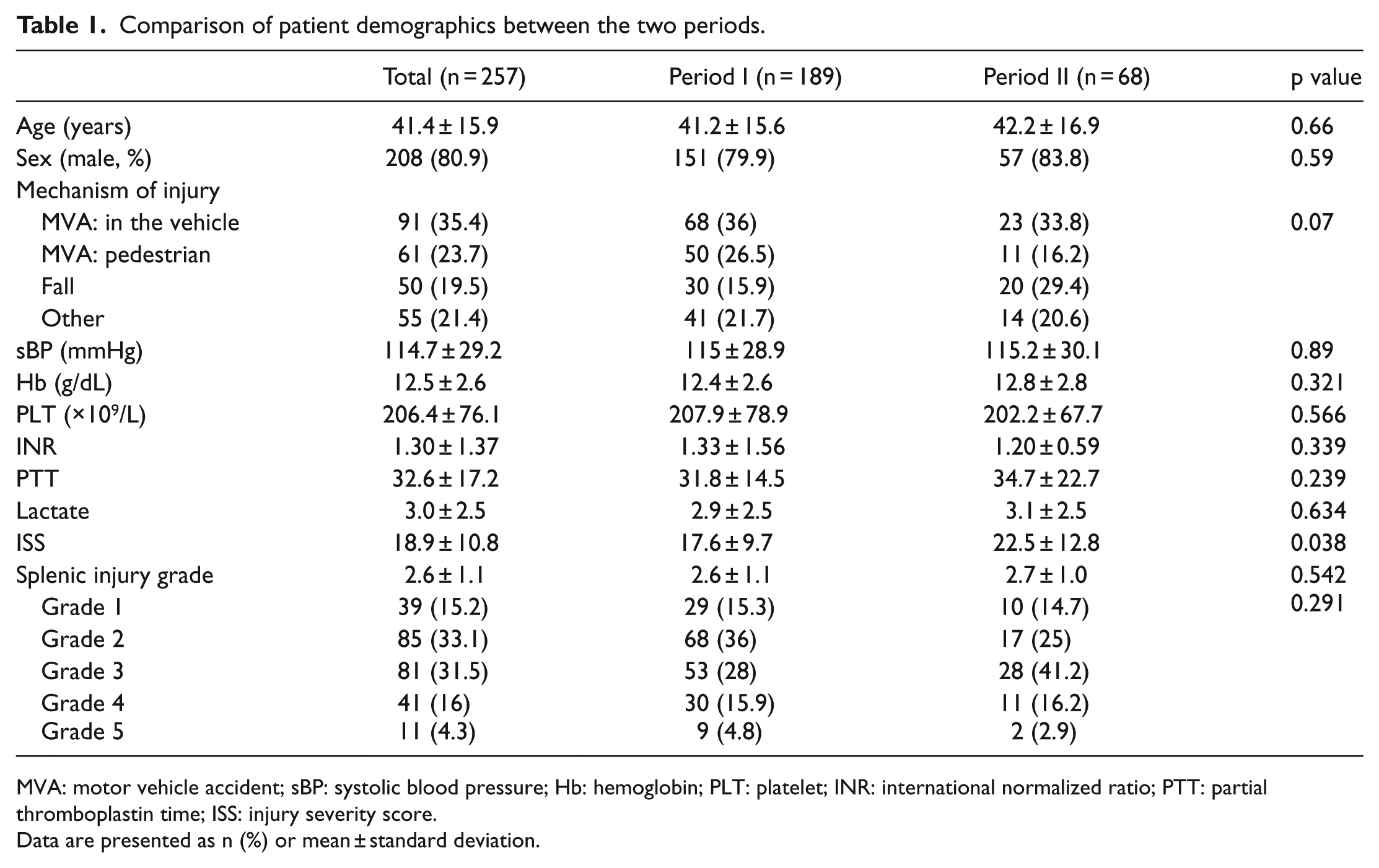
MVA: motor vehicle accident; sBP: systolic blood pressure; Hb: hemoglobin; PLT: platelet; INR: international normalized ratio; PTT: partial thromboplastin time; ISS: injury severity score.
Data are presented as n (%) or mean ± standard deviation.
We evaluated changes in the management and clinical outcomes of patients with splenic injuries of grade 3 or higher. There were significant differences between the two periods in both the management method and time taken to manage these patients. In period I, the rate of performing emergency operations was 29.3%; this decreased to 22.0% in period II. Delayed operations were performed in 12.0% of patients in period I but were not performed at all in period II. Conversely, the frequency of performing angioembolization was higher in period II than in period I (39.0% vs 8.7%, p < 0.001). When emergency surgery was required, the interval from admission to undergoing surgery was significantly lower in period II, decreasing from 302.3 to 68.9 min (p = 0.002). In addition, the time to intervention—whether emergency surgery or angioembolization—was significantly lower during period II, decreasing from 312.8 to 128.6 min (p = 0.001). There was no significant difference in the volume of packed red blood cell (RBC) and fresh frozen plasma (FFP) transfused within the first 24 h after admission. The amount of platelet concentrate transfusion was significantly reduced in period II. The RBC:FFP ratio was significantly different between the two periods (Table 2).
Management of patients with splenic injuries of grade 3 or higher.
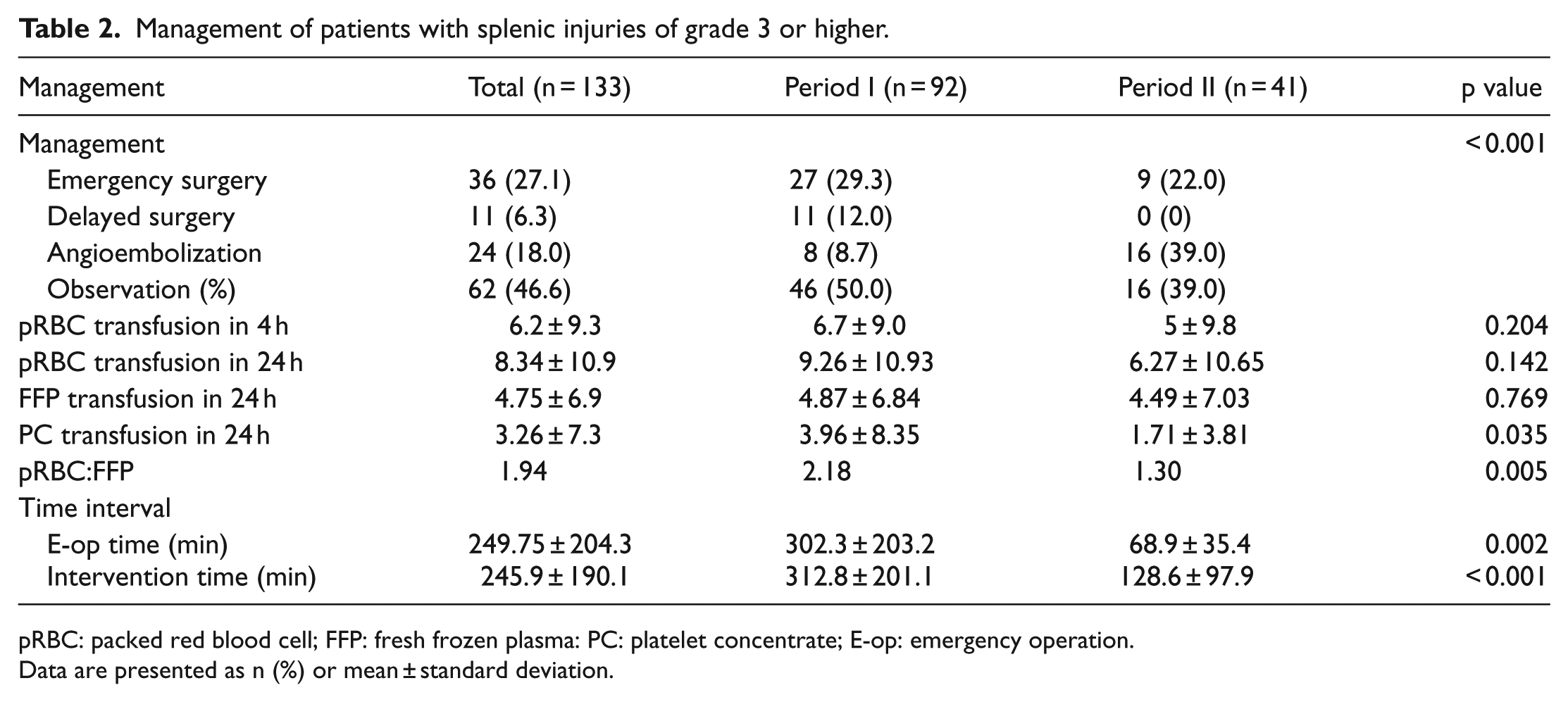
pRBC: packed red blood cell; FFP: fresh frozen plasma: PC: platelet concentrate; E-op: emergency operation.
Data are presented as n (%) or mean ± standard deviation.
NOM was initially performed in 70.6% (n = 65) of patients with high-grade (grades 3–5) splenic injury; this approach failed in 16.9% (n = 9) of patients during period I—these patients underwent splenectomy. In contrast, in period II, NOM was attempted in 78% (n = 32) of cases with high-grade injury; no treatment failures occurred (p = 0.014). There was no difference in ICU stay and hospital stay between periods I and II. However, the spleen salvage rate was significantly higher in period II (78.0%) than in period I (58.7%; p = 0.03). There were no significant differences in overall mortality, hemorrhagic death, and length of ICU or hospital stay between the two periods (Table 3).
Outcomes of patients with splenic injuries of grade 3 or higher.
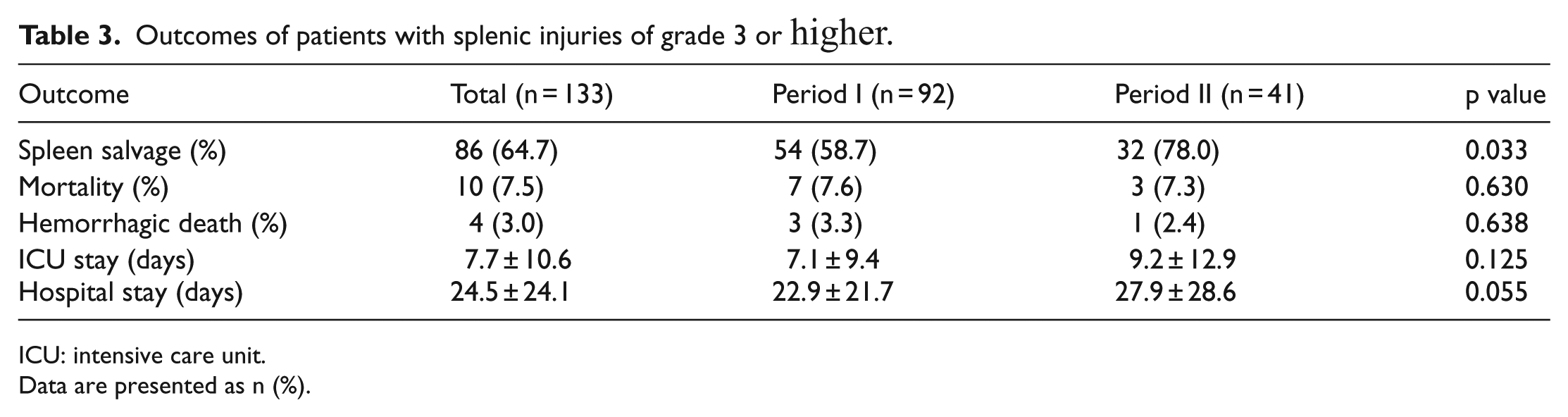
ICU: intensive care unit.
Data are presented as n (%).
Logistic regression analysis was used to examine factors that affected spleen salvage. Injury grade and number of packed RBC units transfused were identified as factors influencing splenectomy as an outcome. The risk of requiring a splenectomy increased with increasing injury grade (odds ratio, 5.29 (95% confidence interval, 2.29–12.23); p < 0.001) and number of packed RBC units transfused (odds ratio, 1.15 (95% confidence interval, 1.07–1.22); p < 0.001), as shown in Table 4.
Multivariable logistic regression for predictors of splenectomy.
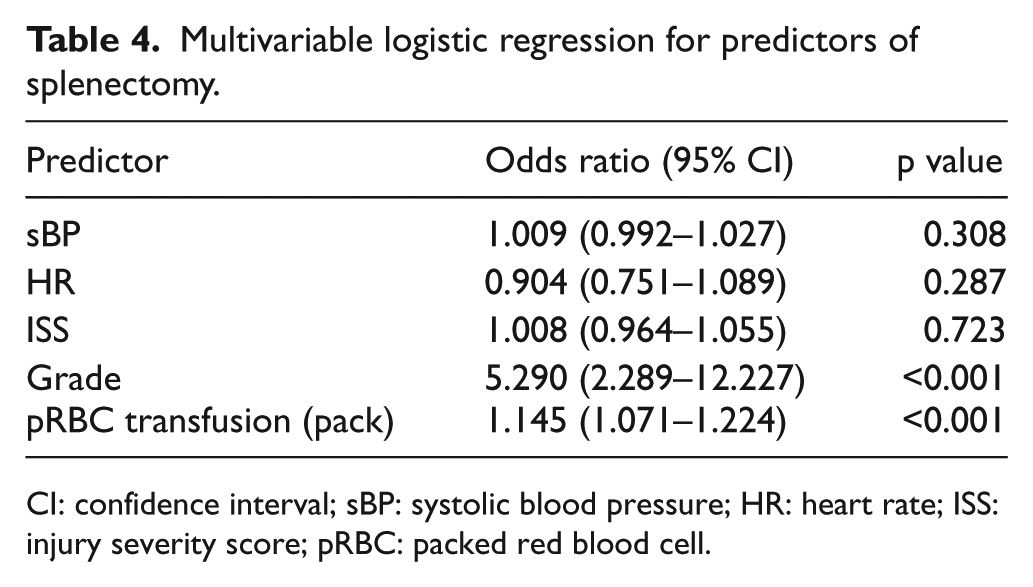
CI: confidence interval; sBP: systolic blood pressure; HR: heart rate; ISS: injury severity score; pRBC: packed red blood cell.
Discussion
We compared data on the management and clinical outcomes of patients with blunt traumatic splenic injury in the period before and after the establishment of a regional trauma center. The severity of spleen injury did not change, but the rate of spleen salvage improved. One of the most influential factors in successful NOM is the active use of angioembolization. We did not perform angioembolization for splenic injury until 2008. Since the establishment of our trauma center in 2014, many management protocols have been applied. Included in these is a protocol for the treatment of solid organ injuries, such as injuries to the spleen. Systematic management of splenic injuries was conducted based on this guideline. In accordance with the guideline, angioembolization was chosen as first-line management for hemodynamically stable patients; the equipment and manpower required for angioembolization, reserved for trauma patients, was made available.
In terms of surgery, there is almost no disagreement about performing an exploratory laparotomy in a hemodynamically unstable patient. However, indications for angioembolization remain controversial. For patients with lower-grade injuries (grades 1–2), non-angiographic observation is performed, and there is no difference in outcome whether angioembolization is performed. 8 However, there are several opinions regarding the cut-offs for performing angioembolization for patients with high-grade injuries. 9 Miller et al. reported that the NOM success rate was increased by applying an angioembolization protocol to patients with grades 3–5 injuries. 10 In other study, embolization was performed in patients with grades 4–5 injuries by modifying the protocol used for embolization in grades 3–5. This change led to a decrease in performing angioembolization in grade 3 (from 68% to 32%), but no changes were observed in terms of complication rate or outcomes. 11
Opinions vary regarding whether contrast blush on CT is an indication for angioembolization. Even with contrast blush, often no active bleeding is found at angiography.12 Hence, contrast blush might not indicate active bleeding, but may be indicative of a parenchymal pseudoaneurysm or arteriovenous fistula.10 Therefore, approximately 30% of centers do not use angioembolization as first-line treatment for patients with contrast blush demonstrated on CT. 12 However, other studies suggest that evidence of extravasation on CT is a significant risk factor for bleeding,13–16 and that vascular abnormalities such as pseudoaneurysms and arteriovenous fistulae are also a factor causing delayed bleeding. 17 The literature indicates that both active bleeding and non-bleeding vascular injuries require splenic surgery or splenic artery embolization for optimal treatment.18,19 We performed angioembolization in patients with contrast blush on CT and a change in hemoglobin level.
Protocol-based selective angioembolization in high-risk patients is a recent trend in the NOM of blunt splenic injury. 20 Miller et al. reported that the higher the protocol compliance, the lower the NOM failure rate. 10 In our center, the protocol compliance was 90.2%. As the management of solid organ injuries has been protocolized and standardized, the decision-making time has become shorter, the difference in treatment due to the differences in individual ability has decreased, and all patients have received standardized treatment. As protocol compliance increased, the rate of angioembolization increased, the frequency of performing of splenectomy decreased, and the time required to make a treatment decision and to implement an intervention reduced. In terms of emergency surgery, the time from arrival in the trauma center to undergoing surgery became significantly shorter (from 302.3 to 68.9 min) because the attending trauma surgeon—resident in the hospital—treated the patient from the outset and decided to operate immediately. Performing angioembolization was also associated with a decrease in the interval from arrival to intervention, because once the trauma center was established, this intervention was actively used, even at night and on weekends. Although there was a significant reduction in the interval from trauma center arrival to undergoing the appropriate procedure, this had no significant effect on splenic salvage or mortality.
Although not statistically significant, the volume of RBC transfused in the first 24 h after admission in period II was lower than it was in period I. This is likely because hemostasis was achieved more rapidly during the latter period. In general, the amount of transfusion of each blood component decreased. With the developed concept of hemostatic resuscitation, the RBC:FFP ratio is being corrected close to 1:1.
In the logistic regression analysis, RBC transfusion volume was identified as a factor affecting splenectomy. Smith et al. 21 reported that mass transfusion is associated with NOM failure. NOM was performed in 85% of all-grade blunt splenic injury patients in period II. In patients with grades 3–5 injuries, 78% underwent NOM. The overall success rate of the NOM of blunt splenic injuries is reported to range between 60% and 90%.22–25 In the present study, we did not observe any difference in mortality between the two groups. This is because the subgroups were too small and the ISS was different in each patient group. After establishment of the trauma center, severe polytrauma patients were concentrated in the center for management, which contributed to the increase in ISS.
This study has some limitations: It was a retrospective, single-center study that included a small number of patients. Hence, it was underpowered to detect significant differences in terms of some potential outcomes.
Conclusion
After the establishment of a trauma center, the rates of spleen preservation and NOM success improved significantly. This may be due to the participation of trauma surgeon from the outset of patient treatment, expansion of angioembolization facilities and resources, and the introduction and application of a standard protocol for managing patients with blunt traumatic injuries of the spleen.
Footnotes
Authors’ contributions
B.Y., J.L., and K.K.C. wrote the study protocol, and all authors contributed important revisions of the protocol. G.J.L. and M.A.L. contributed to the study design, analysis, and interpretation of the results. They wrote and revised the manuscript. J.J.P., Y.P., A.H., and J.G. contributed to the acquisition of data, analysis, and interpretation of the results. All authors read and approved the final manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Informed consent
The patients’ concern has not been needed because of retrospective nature of the study.
Ethical approval
Ethical approval was obtained from Gachon University Gil Medical Center Institutional Review Board (GUGMCIRB) (IRB No. GCIRB2017-388).