
Abstract
Background:
Body packing is a frequently used method for drug trafficking. Local information about the clinical and radiological features of body packing is lacking.
Objectives:
To evaluate the radiological features of body packers presenting to a hospital near to the Hong Kong International Airport and to compare the radiological features of solid form versus liquid cocaine.
Methods:
This was a retrospective cohort study. Medical notes of 269 suspected body packers, presenting to the Accident and Emergency Department of North Lantau Hospital under the detention by the law enforcement personnel from 1st January 2015 to 28th February 2017, were reviewed. The radiological features of body packing were retrospectively evaluated.
Results:
Sixty-nine cases were confirmed body packers radiographically. Majority of them (81%, 56/69) were cocaine packers. Powder form cocaine (67%, 49/69) was the most popular drug packed, followed by liquid cocaine (15%, 10/69). There was a trend of increasing incidence of liquid cocaine packers. The classical ‘double condom’, ‘tic tac’ and ‘halo’ signs were present in 94%, 72.5% and 42% of cases with radiologically confirmed body packing respectively. The ‘rosette’ sign was only identified in 1 case. Three new radiological signs, the ‘bag of eggs’, ‘lucent triangle’ and ‘black crescent’ sign, were suggested to aid identification of drug packets. The classical ‘tic tac’ sign was absent in all liquid cocaine packing cases (p<0.05). The liquid cocaine packets appeared irregular with indistinct border in majority of cases (p<0.05). The solid form packets were mostly opaque to faeces while liquid cocaine had variable density (p<0.05). Most solid form packets had homogeneous content which was in contrast to the heterogeneous content in liquid cocaine (p<0.05).
Conclusion:
Failure in detecting drug body packing may result in medicolegal consequences. Emergency physicians need to be aware of subtle radiological signs of liquid cocaine packets in the plain abdominal radiography.
Introduction
Body packing refers to the concealing of illicit drugs in the abdominal or pelvic cavity of the human body 1 and was first described in literature in 1973 by Deitel and Syed, 2 who reported a 21-year-old developing small bowl obstruction after ingestion of a condom filled with hashish. It is a frequently used method for drug trafficking to avert detection at border crossings or airport customs. Body packers may ingest packets of varying sizes and containing various illicit drugs, including cocaine, 3 amphetamine, 4 3,4-methylenedioxymethamphetamine (‘ecstasy’), 5 marijuana, 6 and heroin. 7 Alternatively, body packers may introduce drug-filled packets into their bodies per rectally or per vaginally. They may present to the accident and emergency departments (AEDs) for complications from the body packing, including acute drug toxicity and surgical complications, for example, bowel obstruction, bowel perforation and peritonitis or most often for medical examination after custody by the customs officers and police. 8
Radiological evaluation by the plain abdominal radiography is a commonly adopted approach for screening and diagnosing body packing of illicit drugs. The reported sensitivity of plain abdominal radiography to detect intra-intestinal drug packets was up to 90%. 9 Several specific radiological signs in the plain abdominal radiography have been suggested for the presence of intra-intestinal drug packets including multiplicity (multiple radiopaque foreign bodies), the ‘double condom’ sign and the ‘rosette’ sign. 10 However, the sensitivity of detecting body packing by the plain abdominal radiography is influenced by various factors including the type and purity of drugs which determine the density, packet material, size and number of packets, location within intestines and also the experience of the reader. 1
Other radiological modality such as computed tomography (CT) has also been advocated for evaluating of suspected body packers for its superior sensitivity and specificity. However, there are legal restraints related to overexposure to radiation, and it is usually reserved for those with negative abdominal plain films but a high index of suspicion of package concealment. 11
North Lantau Hospital (NLTH) is a regional hospital located in central Tung Chung of Lantau Island in close proximity to the Hong Kong International Airport. Suspected body packers under detention by the customs officers and police in the airport are brought to the AED of NLTH for medical assessment. After history taking, physical examination and informed consent, plain abdominal radiography (abdominal X-ray (AXR) or kidney, ureter and bladder X-ray (KUB)) is arranged to detect the presence of body packing. CT of abdomen is arranged for those with unclear findings in the initial plain abdominal radiography or strong clinical suspicion. Confirmed asymptomatic body packers, detected either by body packing in plain abdominal radiography or CT abdomen, are transferred to the custodial ward in Queen Elizabeth Hospital (QEH) for further management. Local publication on the radiological features of these asymptomatic body packers is lacking and we reported our experience of roentgenographic findings of these body packers encountered in the AED of NLTH.
Methods and materials
Subjects
Medical notes of 269 suspected body packers, who were detained by the customs officers and police and were brought to the AED of NLTH for medical assessment from 1 January 2015 to 28 February 2017, were reviewed. Contents in the drug packets passed by the body packers were ascertained by the government laboratory of the Hong Kong Special Administrative Region and were provided by the Hong Kong Customs and Excise Department. The radiological findings of body packing in the plain abdominal radiography and CT were retrospectively evaluated.
Image acquisition
Abdominal plain films were performed with the suspected body packers in the supine position and by the standard anteroposterior view with a digital X-ray system (Discovery™ XR636; GE Medical Systems, Pittsburgh, PA, USA) with a tube voltage of 80 kVp, tube current by automatic exposure control and focus–film distance of 100 cm. Abdominal CT scans were performed with a 64-slice multidetector computed tomography (MDCT) system (LightSpeed™ VCT; GE Medical Systems) with collimation of 64 × 0.625 and a reconstruction section thickness of 5 mm. A voltage of 120 kV was used.
Radiological interpretation
The plain abdominal films (AXR or KUB) of all the 69 confirmed body packers were retrospectively interpreted by one independent radiologist and one independent emergency physician with professional experience more than 10 years. The radiological features and other specific radiological signs of body packing were recorded using standard checklist. The radiological features of liquid cocaine body packing were compared with those of solid form drugs body packing. New radiological signs of liquid cocaine body packing and intra-intestinal drug packets were also identified. Discrepancy in detecting individual radiological signs or features on the plain abdominal radiography was recorded and then discussed among the two doctors to arrive at a consensus. The radiological signs of body packing in the CT scan images were reviewed by the radiologist.
Radiological signs for intra-intestinal drug packets in the plain abdominal radiography
The ‘tic tac’ sign was used to describe the presence of multiple homogeneous radiopaque oval/round-shaped foreign bodies with sharp border and clear air–substance interface on the plain abdominal radiography. 10 The ‘bag of eggs’ sign addressed the non-uniform geometric shapes of packing in the plain abdominal radiography. Presence of the ‘tic tac’ sign or ‘bag of eggs’ signified a clear identification of intra-intestinal drug packets.
The ‘double condom’ sign was a radiolucent rim of air trapped between the multiple layers of packing surrounding each drug packet in a well-defined shape. 10
The ‘rosette’ sign was formed by air trapped in the knot where the packing was tied. 10
The ‘halo’ sign was a complete rim of blurred lucency around the drug packet. 10
The ‘black crescent’ sign was a new radiological sign of body packing identified in our study. It represented crescent of air around the drug packet.
The ‘lucent triangle’ sign was another newly identified sign representing air in the interface between drug packets or with bowel wall.
Apart from specific radiological signs of intra-intestinal drug packets on the plain abdominal radiography, the density (opaque to faeces or faeces-like), the geometric shape and the border of the drug packets and the presence of dilated bowel were also recorded.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) version 19.0 for Windows was used for analysis. Descriptive statistics were used to summarize the prevalence of radiological features and specific radiological signs of body packing in both plain abdominal films and the CT scan images. Kappa statistic was used to assess the inter-observer agreement for the detection of the radiological signs of body packing by the radiologist and the emergency physician. The radiological features of liquid cocaine were compared with those of solid form drug body packing. Univariate analysis was performed with chi-square test or Fisher’s exact test for comparison of proportion. The statistical significance was set at p < 0.05.
Ethical considerations
This study was approved by the clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority. The confidentiality of the patients was protected as all the study findings were presented anonymously and the personal information of the patients were stored in a locked cabinet which could only be opened by the relevant research personnel.
Results
During the period January 2015 to February 2017, 269 individuals (185 males and 84 females) were brought to the NLTH AED for suspected body packing. The mean age was 36.7 years (range: 19–74 years). All these suspected body packers were asymptomatic on arrival to the AED. Plain abdominal radiography (AXR or KUB) was done in 264 (98%) cases, while X-ray was not performed in five cases because of refusal or pregnant status. Out of the 264 cases with plain abdominal radiography, 60 cases were positive, 180 were negative and 24 were indeterminate after interpreted by the attending emergency physicians. The main reasons of inability to confirm drug body packing on the plain abdominal radiography were the absence of the typical appearance of intra-intestinal drug packets and the variable density of the drug packets resembling faeces in the bowel. CT scan was arranged to confirm the drug body packing in those 24 indeterminate individuals. Nine more cases were found to be positive after the CT imaging (Figure 1). Majority of confirmed body packers came from Africa or America (Central or South, including Colombian, Venezuelan and Peruvian). The most popular drug smuggled was cocaine (56/69, 81%), predominantly in the form of powder cocaine (46 cases) versus liquid cocaine (10 cases). The mean amount of liquid cocaine smuggled in the body packer was 1319 g, with range from 560 to 3672 g (vs the mean amount of 1148 g in other solid form drugs’ body packing). There was a trend of increasing incidence of liquid cocaine packing (one case in 2015 vs eight cases in 2016). There was one case of heroin body packer. Drug packet contents of 12 individuals were not available. Most cases of powder form cocaine packing (43/46, 93%) could be detected in the plain abdominal radiography by the attending emergency physicians, while about half of the liquid cocaine cases required CT for detection. All these body packers passed the drug packets uneventfully during their stay in the custodial ward in QEH.
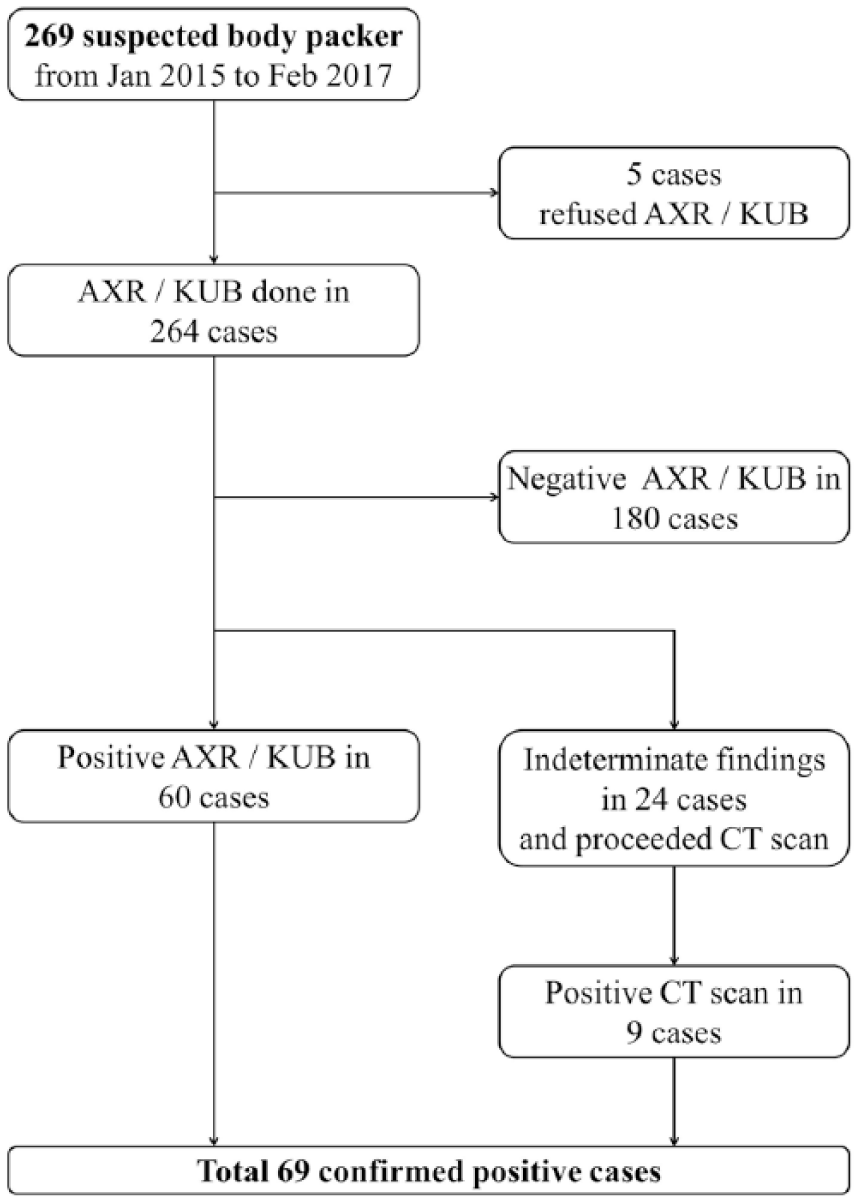
Flowchart for cases recruitment.
The result of the inter-observer agreement (kappa coefficient) between the radiologist and emergency physician is shown in Table 1. All radiological features and individual radiological signs had substantial and almost perfect inter-observer agreements 12 except the ‘rosette’ sign.
Inter-observer agreement between the radiologist and emergency physician on the radiological features and specific radiological signs in all the radiologically confirmed body packers (69 cases in total).
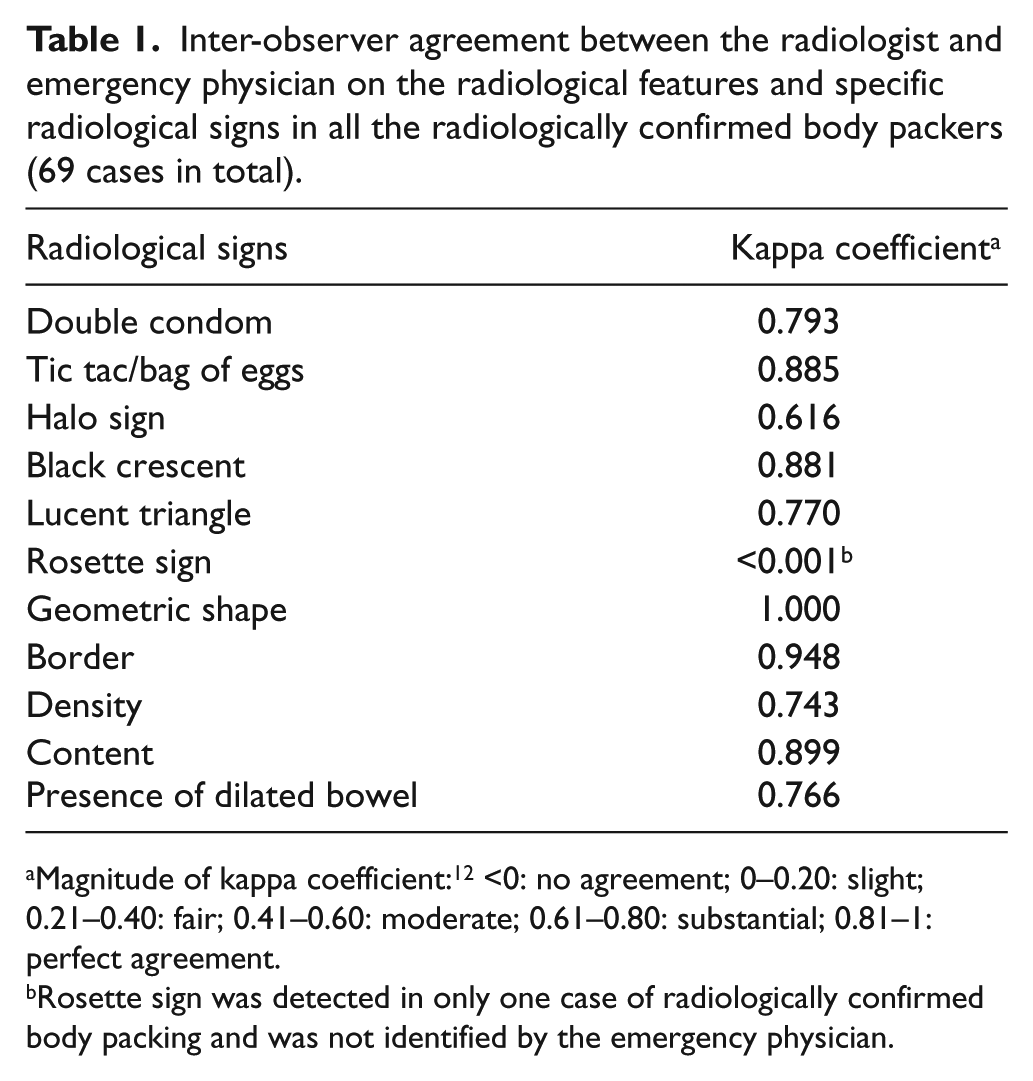
Magnitude of kappa coefficient: 12 <0: no agreement; 0–0.20: slight; 0.21–0.40: fair; 0.41–0.60: moderate; 0.61–0.80: substantial; 0.81–1: perfect agreement.
Rosette sign was detected in only one case of radiologically confirmed body packing and was not identified by the emergency physician.
The radiological features of all the cases with radiologically confirmed body packing are summarized in Table 2 and Figure 2. Overall, the classical ‘double condom’ (Figure 3(a)), ‘tic tac’ or ‘bag of eggs’ sign (Figure 3(b)) and ‘halo’ sign (Figure 3(c)) were present in 94% (65/69), 72.5% (50/69) and 42% (26/69) of the cases, respectively, while the ‘rosette’ sign was only identified in one case (Figure 4(a)). Two new radiological signs, the ‘lucent triangle’ sign (Figure 4(b)) and ‘black crescent’ sign (Figure 4(c)), were suggested to provide additional clues to identify the drug packets in the plain abdominal radiography. The ‘lucent triangle’ and ‘black crescent’ signs were present in 82.6% (57/69) and 75.4% (52/69) cases with radiologically confirmed body packing, respectively.
Prevalence of individual radiological signs and other radiological features of the confirmed body packers.

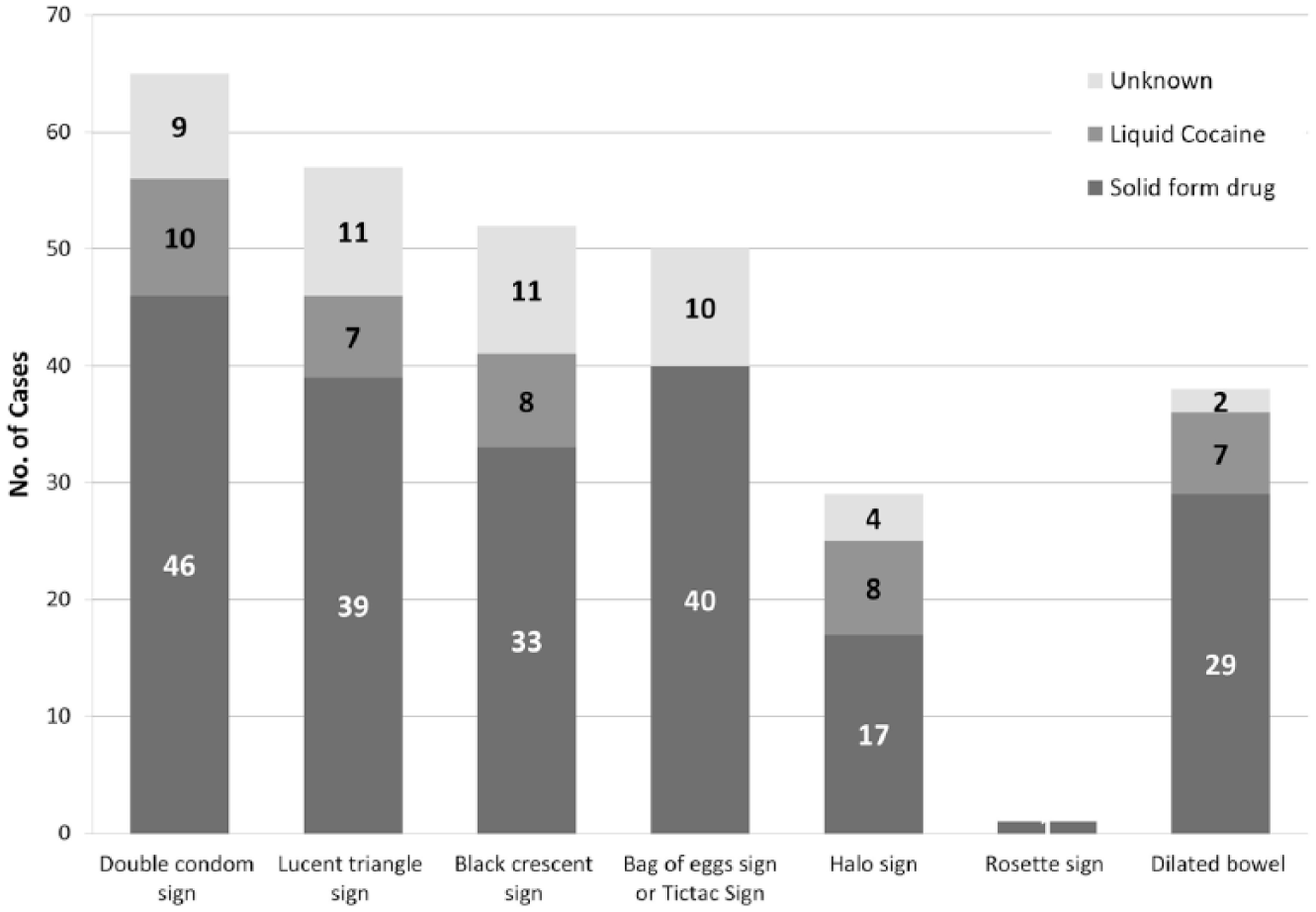
Radiological features in the studied population with radiologically confirmed body packers (69 cases in total).
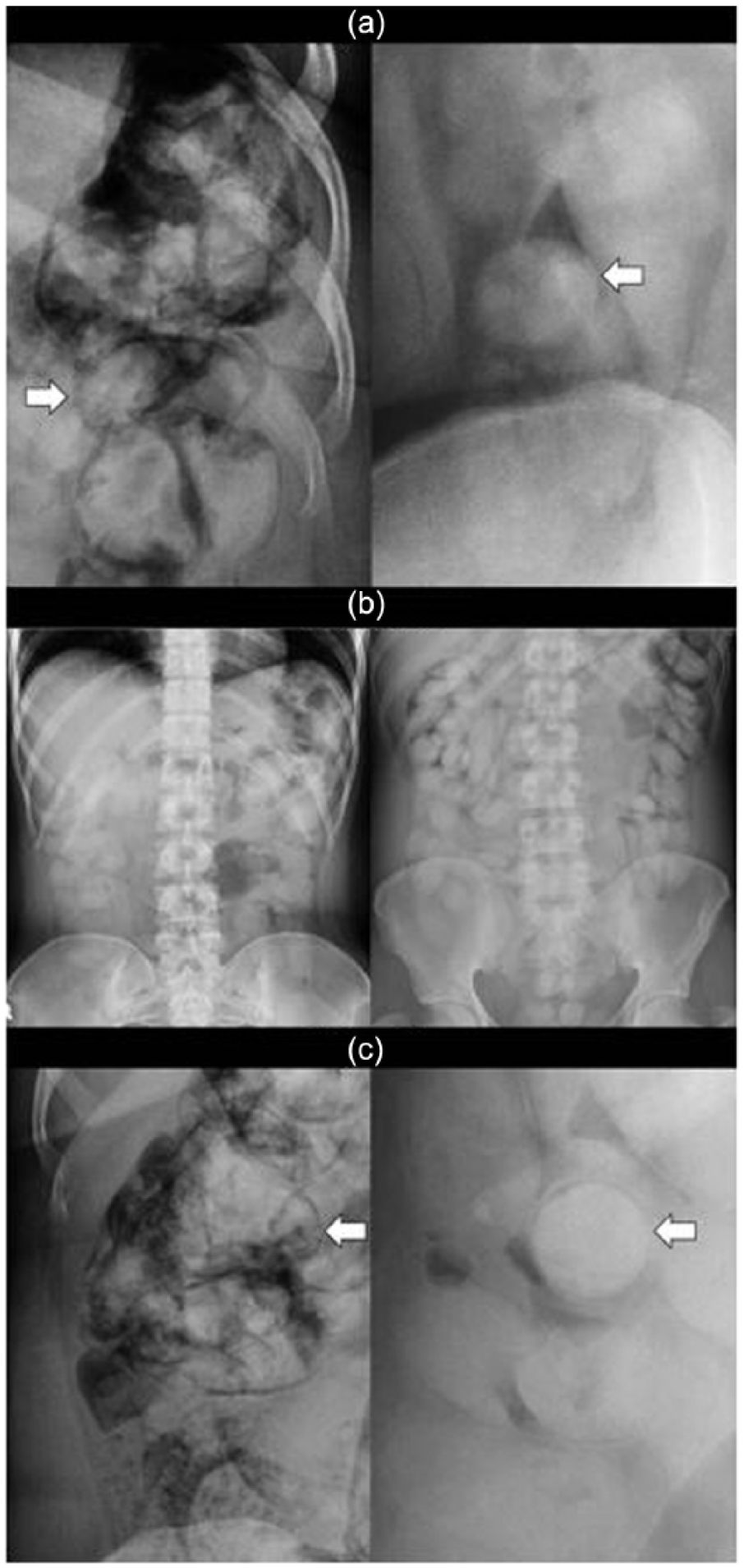
(a) ‘Double condom’ sign (rim of air trapped between multiple layers of packing surrounding each packet): liquid cocaine body packing (left) and powder form cocaine body packing (right). (b) ‘Bag of eggs’ or ‘tic tac’ sign (presence of multiple homogeneous radiopaque round-shaped foreign bodies with sharp border and clear air-substance interface): absent in cases of liquid cocaine body packing (left) and much clearer in powder form cocaine packing (right). (c) ‘Halo’ sign (complete rim of blurred lucency around drug packet): liquid cocaine body packing (left) and powder form cocaine body packing (right).
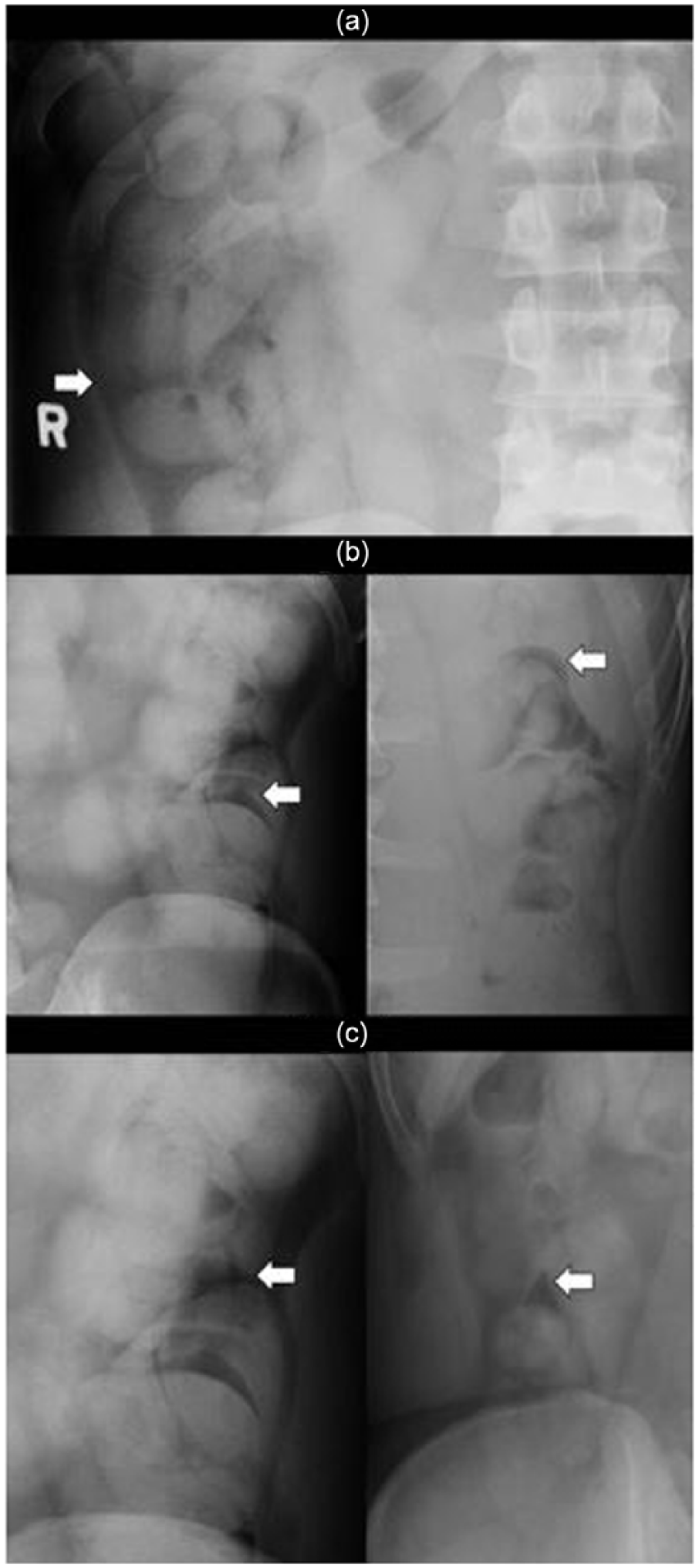
(a) ‘Rosette’ sign (air trapped in the knot where the packing is tied), (b) ‘black crescent’ sign (crescent of air around drug packet): in liquid cocaine (left) and powder form cocaine body packing (right), (c) ‘lucent triangle’ sign (air in the interface between drug packets or with bowel wall): in liquid cocaine (left) and powder form cocaine body packing (right).
The radiological features of solid form drug body packing were compared with those of liquid cocaine body packing. The 12 cases of unknown drug packet contents were excluded in the analysis. The results are shown in Table 3 (57 cases in total). Compared with solid form drug packing, the ‘tic tac’ sign was absent in all the cases of liquid cocaine body packing (p < 0.05). The liquid cocaine drug packets appeared to be irregular with indistinct border in majority of cases (p < 0.05). The solid form drug packets were mostly opaque to faeces, while liquid cocaine had variable density (p < 0.05). Most solid form drug packets had homogeneous content (Figure 5(a) and (b)) which was in contrast to the heterogeneous content in liquid cocaine packing (Figure 5(c)) (p < 0.05).
Comparison of specific radiological signs and other radiological features of liquid cocaine body packing and other solid form drugs body packing (57 cases in total).
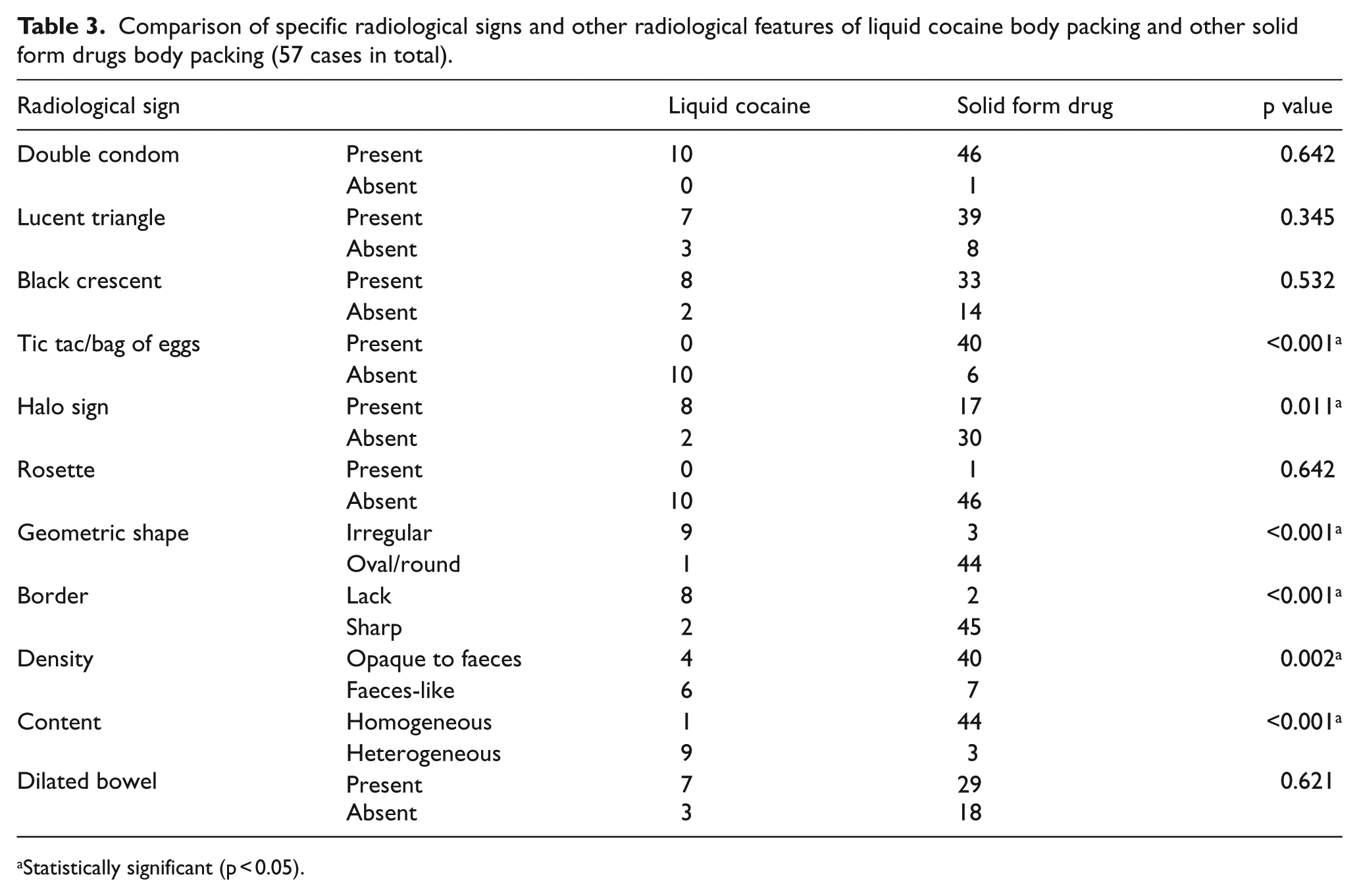
Statistically significant (p < 0.05).
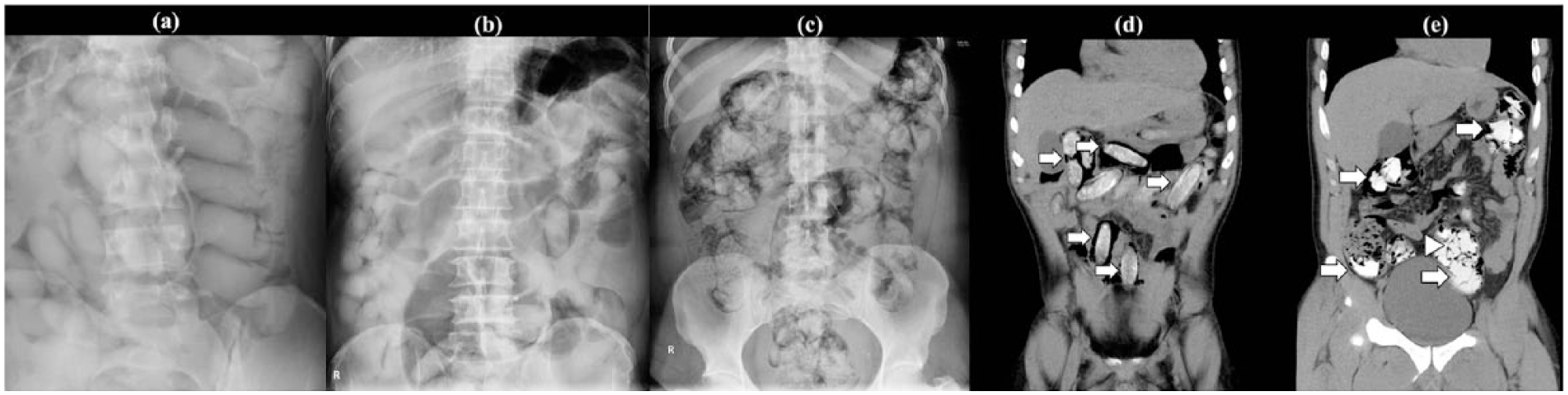
(a) X-ray showing homogeneous powder form cocaine with sharp border, oval shape and are opaque to soft tissue; (b) X-ray showing dilated colon in a powder form cocaine body packer; (c) X-ray showing gaseous dilated bowel in a liquid cocaine body packer; (d) CT showing solid form cocaine drug packets (arrows) with ‘double condom’ and ‘halo’ signs; and (e) CT showing liquid cocaine drug packets (arrows) which conform to the contour of intestinal lumen; jigsaw sign of drug packets was shown (arrow head).
CT scan was arranged in 24 indeterminate individuals and 9 cases were found to be positive including 5 cases of liquid cocaine, 3 cases of powder form cocaine and 1 case of unknown content. Body packing appeared as multiple hyperdense intra-intestinal foreign bodies in the CT images with density ranging from 70 to 250 Hounsfield unit (HU) (Figure 5(d) and (e)). Five cases showed dilated bowels and none demonstrated pneumoperitoneum.
Discussion
Heroin used to be the most often smuggled drugs by the body packers worldwide 3 but its abuse has been reducing both internationally and locally. According to the Customs and Excise Department Departmental Review, a decreasing trend of heroin confiscation was observed in recent years with only 4.2 kg of heroin captured and 13 persons arrested in 2016 (vs 10.8 kg of heroin captured with 24 persons arrested in 2015). On the other hand, cocaine is gaining popularity with 150 persons arrested and 244.6 kg of cocaine seized in 2016, which is a 7% increase when compared with 2015. Among the confiscations, 171.8 kg were intercepted with 104 persons arrested at the Hong Kong International Airport. 13 Plain abdominal radiography, for its wide availability, is the traditionally employed method to screen and diagnose drug body packing in the local AEDs. 14 However, the sensitivity for detecting drug body packing by the initial plain abdominal radiography varied widely from 40% to 90% in the published literature.9,11 Several radiological signs of solid form drugs body packing have been described in the literature.1,9 Niewiarowski et al. retrospectively reviewed the plain abdominal radiography of 285 suspected body packers presenting to the Hillingdon Hospital, the neighbouring hospital next to Heathrow Airport. Among the 59 positive cases of body packing, the reported frequency of several specific radiological signs, namely, the ‘tic tac’ sign, the ‘double condom’ sign and the ‘dense surrounding wrapping material’ signs, was 93%, 73% and 36%, respectively. They described a new radiological sign of drug body packing, the ‘parallelism’ sign, which described intra-intestinal drug packets lying in parallel in the bowel lumen. This ‘parallelism’ sign, though only identified in 27% of the positive cases, was found to be highly specific. Another classical sign, the ‘rosette’ sign, was absent in all the positive cases. 10 Similar to the their findings, 10 the ‘rosette’ sign was present in only one case of solid form drugs packing in our series (Figure 4(a)) and was also missed by the emergency physician reviewing the film independently. This radiological sign is difficult to recognize and is not useful to detect drug body packing. The ‘tic tac’ sign was originally used to describe the presence of multiple oblong, uniformly shaped intra-intestinal drug packets on the plain abdominal radiography. 10 However, this uniformity is not universal, and a more appropriate descriptive term, ‘bag of eggs’ sign, was suggested in our study to address the non-uniformly geometric shaped packets in the plain abdominal radiography. Presence of the ‘bag of eggs’ sign signified a clear identification of intra-intestinal drug packets on the plain abdominal radiography. Although the ‘tic tac’ sign or ‘bag of eggs’ sign was highly specific for solid form drugs body packing, they were absent in six cases of the solid form drugs body packing cases in our case series. It was because only a few (instead of multiple drug packets as in the definition) radiopaque oval/round-shaped foreign bodies were identified in the plain abdominal radiography in those six cases. Owing to the variable geometric shapes and density of the liquid cocaine packets, the ‘bag of eggs’ or ‘tic tac’ sign was not detected in all the liquid cocaine body packers.
Liquid cocaine body packing is a novel method for smuggling drugs by the drug traffickers and it poses great difficulty for the emergency physicians to detect in the plain abdominal radiography since it has irregular shapes that conform to the intestinal contour 15 (Figure 5(c)). The liquid cocaine is prepared by dissolving solid cocaine powder in a variety of solvents, which allows subsequent conversion back to the powder form. The radiological properties of liquid cocaine are different from those of powder form cocaine and other solid form illicit drugs, making the liquid cocaine packets more difficult to be detected on the plain abdominal radiography. The ‘double condom’ sign and ‘halo’ sign, traditionally used to detect solid form packing, are still useful for detection of liquid cocaine. Mozes et al. suggested a subtle radiological feature of liquid cocaine body packing, ‘thin lucent lines’, in the plain abdominal radiography. The ‘thin lucent lines’ are formed by the thin layers of intestinal gas trapped in the interfaces between the adjacent packets. 16 However, this radiological sign is difficult to be identified, particularly by inexperienced readers. This sign was also not common in our series. Two new radiological signs, the ‘lucent triangle’ sign and the ‘black crescent’ signs, were suggested to offer additional hints for identification of drug packets in the plain abdominal radiography. These two signs were even more prevalent than other classical signs of body packing in our series and they also remained discernible in both liquid and solid form drugs’ body packing. Burillo-Putze et al. 15 reported that liquid cocaine had lower radiological density and diffuse borders resembling faeces in the bowel. In our series, liquid cocaine had variable density with 40% opaque to faeces and 60% being faeces-like. The variation can be due to the composition with other substances or the grade of purity. The presence of dilated bowel was also a common finding in both liquid cocaine and solid form drug packers (Figure 5(b) and (c)). Early surgical assessment was suggested for those with mechanical complication from body packing.
Kappa analysis suggested substantial to almost perfect agreement in identifying most radiological signs in body packers between the emergency physician and the radiologist. This is reassuring that frontline emergency physicians, after adequate training and accumulation of experience, are able to detect the radiological features of body packers, thus minimizing the medicolegal consequence of missing a case of body packers.
Abdominal CT scan is superior to plain abdominal radiography in detecting drug packets for both solid form drugs and liquid cocaine. 16 Abdominal CT scan without contrast is usually adequate to serve the purpose of detecting body packing. On the contrary, oral or rectal contrast may obscure concealed packets due to the similarities in density. 17 Oral contrast also stimulates osmotic intestinal inflow which could exacerbate intestinal obstruction. Intravenous contrast agent should be considered for assessing surgical complications (e.g. bowel obstruction, perforation or ischaemia). For the interpretation of CT images, the use of conventional abdominal window together with lung window can enhance the detection of body packing. The classical radiological signs of body packing in plain abdominal radiography, for example, the double condom sign, tic tac sign and parallelism, could also be recognized in the CT images (Figure 5(d)). The use of Hounsfield unit (HU) has been advocated to help differentiate the contents in the drug packets. Wackerle et al. 18 demonstrated the differences in the density of different drug packets: density of cannabis similar to bone (700 HU), density of cocaine less than fat (−219 HU) and density of heroin between the fat and air (−520 HU). However, these findings are not consistent as the densities of the drug packets vary with the presence of impurities. Flach et al. reported the density of pure cocaine to be −200 HU. However, the density changed up to 300 HU after mixing with other cutting agents. 19 One of the major concerns of CT scan is the radiation exposure risk. The ionizing radiation energy of abdominal CT scan can be up to 10 mSv. The use of low-dose CT scan for better delineation of drug packets has been reported. 20 However, the dosage of radiation exposure of CT scan is still significantly higher than conventional radiography and it should be reserved for assessing inconclusive plain abdominal radiography results.
Ultrasound imaging technique has been developed as an invaluable bedside tool providing important clinical information with a major impact on acute patient care in the AED. Benefits of ultrasonography (USG) include widespread availability and lack of ionizing radiation. The sensitivities of using USG to detect drug body packing in an airport screening setup were reported to be over 90%. 21 With the identification of special sonographic features, liquid form drug packets can also be differentiated from solid form drug packets by USG. 22 However, the technique requires skill and is operator dependent. With the advanced development of USG training for the emergency physicians, USG could be an alternative screening tool for drug body packing with comparable sensitivity to plain abdominal radiography. In addition, it has a particular advantage over plain abdominal radiography in screening drug body packing in pregnant women.
Being the AED nearest to the Hong Kong International Airport, NLTH AED probably has the largest series of AXRs of body packers in Hong Kong. The authors believed that this publication can provide valuable reference for frontline emergency physicians to pick up subtle radiological features of body packing, thus reducing the medicolegal risks of managing body packers in Hong Kong.
Limitations
There were several limitations in our study. First, the diagnostic accuracies and the true prevalence of the individual radiological signs of body packing in the plain abdominal radiography, including sensitivity, specificity, positive predictive value, negative predictive value, positive and negative likelihood ratios, were not able to be evaluated in our study as there was lack of standard definition for the ‘negative’ cases. According to the policy of our unit, plain abdominal radiography was used as the screening tool for all the suspected body packers. Although there was known limitation of the accuracy of plain abdominal radiography to detect body packing, most of the ‘negative’ cases in our series were defined by the negative plain abdominal radiography findings from the attending emergency physicians. CT scan was more reliable to rule out body packing. However, it was only performed in a few cases with indeterminate findings in the plain abdominal radiography or high clinical suspicion in view of limited resources and the consideration of radiation exposure risk. Second, only the plain abdominal radiography films of the positive cases were reviewed by the two doctors. Therefore, they were not blinded to the results which might affect their interpretation. Third, the diagnostic accuracies of the two new radiological signs, ‘black crescent’ sign and ‘lucent triangle’ sign, were not evaluated in this study. The sensitivity and specificity of these two signs might be limited but they could act as useful ancillary radiological signs to detect body packing particularly when the other radiological findings were indeterminate. Further study to validate the newly discovered radiological signs is required. Finally, there was limited sample size for the cases with confirmed packet content which might affect the analysis for the comparison of radiological features of liquid cocaine and solid form drug packet.
Conclusion
Plain abdominal radiography is a currently adopted screening tool to detect drug body packing in the routine practice. Liquid cocaine body packing, as a novel method of drug smuggling, is often difficult to be identified on the plain abdominal radiography. Emergency physicians have to be aware of the radiological signs that may aid in detecting liquid cocaine body packing on the plain abdominal radiography. The use of CT and USG as adjuncts can help to increase the detection rate of body packing.
Footnotes
Acknowledgements
The authors would like to thank the Hong Kong Customs and Excise Department for providing the data of the contents in the drug packets from the body packers and Mr Lee Wing Chung, Secretary of AED NLTH, for the clerical support of this publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
All patients’ identifications were removed before storage. The master data set was kept by the investigators in computer and password was required to open the file. Access to the data would be limited to the investigators and clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact principal investigator should further information of the data is required.
Informed consent
Informed consent was waived by the clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Ethical approval
This study was approved by the clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.