
Abstract
In attempted suicide, laryngotracheal rupture caused by hanging leads to rapid death at the scene or before arrival at hospital. The case presented here describes a patient with complete tracheal rupture from an attempted suicidal hanging who was successfully resuscitated. Pre-hospital providers transferred the patient to hospital without being aware of the possibility of airway damage. Cardiac arrest occurred shortly after arrival at hospital. During the cardiopulmonary resuscitation, endotracheal intubation was performed, and fortunately, the tracheal tube was located just below the ruptured trachea and thus enabled ventilation. For patients suspected of having airway damage at the pre-hospital stage, awareness of the patient’s condition and adequate airway management are important. The management of laryngotracheal rupture which suggests that for patients not adequately ventilated, immediate treatment with flexible fiberoptic intubation or tracheostomy is needed to secure the airway. Equipment and personnel at the receiving hospital need to be prepared for immediate treatment.
Introduction
In attempted suicide, laryngotracheal rupture caused by hanging leads to rapid death at the scene or before arrival at hospital. This injury is rarely encountered by medical practitioners; however, if laryngotracheal rupture has occurred and it is not possible to properly maintain the airway, the injury is fatal in more than 75% of cases.1,2 The literature recommends use of flexible fiberoptic intubation or immediate tracheostomy for patients with respiratory difficulty or damage to the respiratory tract after hanging.3,4 Because these devices are frequently unavailable at the pre-hospital stage, patients arrive at hospital with endotracheal tubes or supraglottic devices to secure the airway. The result can be false passage intubation or damage to anatomical structures. 5 This case describes a patient with complete tracheal rupture after hanging with successful recovery.
Case
A 70-year-old man was found hanging from a height of two stories with rope by his spouse. She immediately cut the rope and activated the emergency medical system. The emergency medical team (EMT) arrived approximately 10 min later. The patient lied down on the ground. The patient was unconscious, with initial vital signs were blood pressure 160/100 and heart rate 120 times. The rescue team removed the rope from the patient’s neck, placing him in a cervical collar. Bag-valve mask (BVM) ventilation for oxygenation was used; he was transported to the emergency medical center. Approximately 40 min after leaving the site of the incident, his vital signs were blood pressure 171/122, heart rate 115 times, respiratory rate 28, and respirations being assisted with a SpO2 of 98% on 15 L oxygen.
He arrived at the emergency medical center approximately 50 min post-incident. He had a rope mark on his neck, with subcutaneous emphysema found on his entire body including face and neck. The patient’s pulse was palpable; SpO2 was checked 96%. But he was comatose, and his Glasgow Coma Scale (GCS) score was E1V1M1. He was moved to the resuscitation room for immediate treatment.
Approximately 5 min after he arrived at hospital, carotid and femoral pulses were not detected. Cardiopulmonary resuscitation (CPR) was begun; initial rhythm was pulseless electrical activity (PEA). As Ambu bagging continued, there was an increase in subcutaneous emphysema toward the face and neck. The BVM was removed and an endotracheal tube inserted. Direct observation with laryngoscope showed no bleeding or edema near the glottic opening and a 7.5 cuffed endotracheal tube was inserted confirmed to have passed through the vocal cords. Following insertion of the tube, no further subcutaneous emphysema developed.
After two cycles of cardiac compressions, the return of spontaneous circulation (ROSC) was achieved. A contrast-enhanced computed tomography (CT) scan of the neck and chest areas was performed, and diffuse soft tissue emphysema, pneumothorax, pneumomediastinum, and ruptured trachea were found. Figure 1(a) shows the tip of the tube on the soft tissue and Murphy’s eye on the lower part of ruptured trachea. Figure 1(b) shows the completely ruptured trachea at the seventh cervical vertebra level. The patient was moved to the operating room where surgical treatment of the ruptured trachea and a tracheotomy were performed.
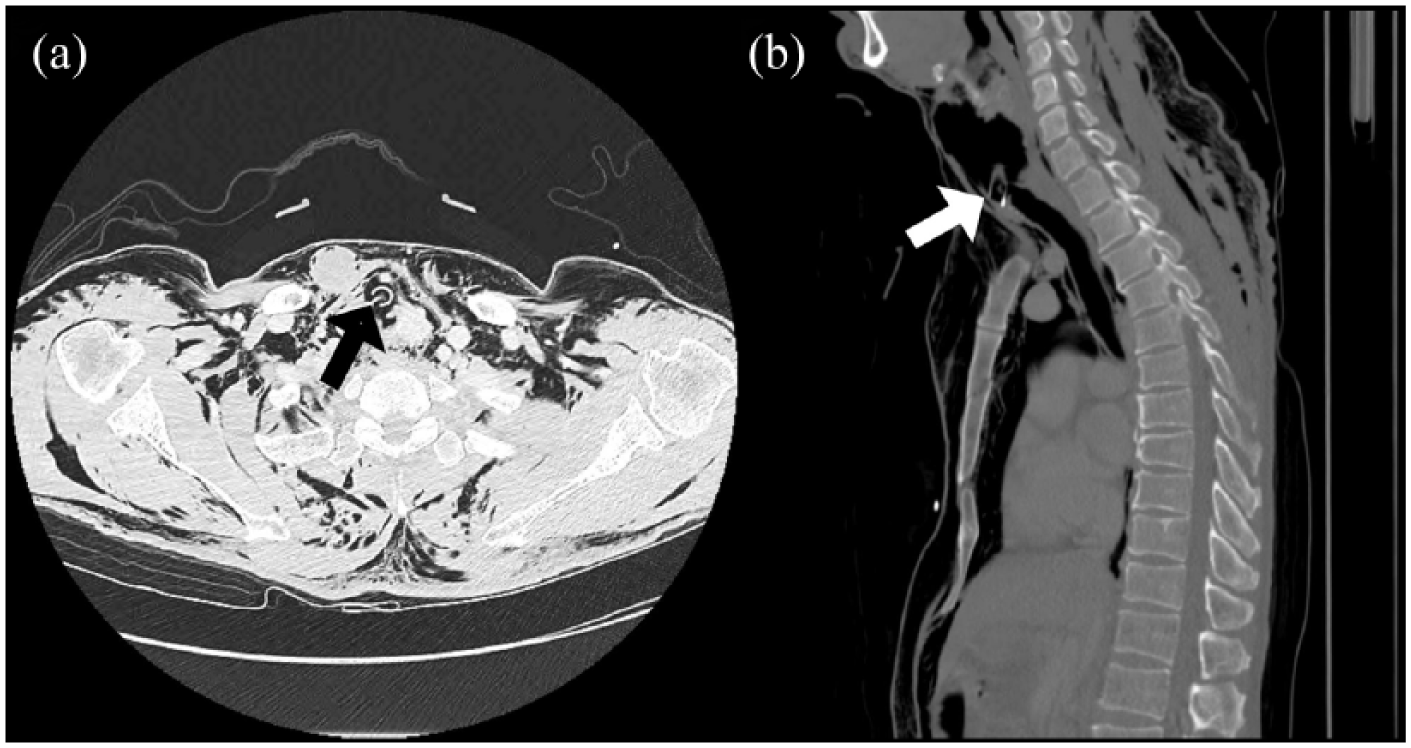
CT scan of the chest with lung windows (a) shows a ruptured tracheal wall anchoring the Murphy’s eye of the endotracheal tube (black arrow). CT scan with bone windows (b) shows complete tracheal rupture at the seventh cervical vertebra level (white arrow).
Postoperative recovery in the intensive care unit was uneventful and neuropsychological evaluation was performed. On the 8th hospital day, the patient was discharged to rehabilitation center without neurological deficit.
Discussion
Significant laryngotracheal trauma is rarely encountered because of the protected anatomical position of the larynx and trachea. With hangings, most victims die before reaching hospital; therefore, it is not possible to know the true occurrence rate of laryngotracheal injury. Autopsies have revealed that 35%–45% of hanging victims have significant laryngeal injuries.1,6
The laryngotracheal injury mechanism due to hanging appears to be the direct, upward pressure on the larynx, causing the larynx to lift and a shearing force to separate larynx and trachea. 7 Trachea, nerve, blood vessels, and esophagus may be damaged. Symptoms of laryngotracheal injury include dyspnea, subcutaneous emphysema, and hemoptysis as well as hoarseness. 8
At the pre-hospital stage, patient care should focus on acquisition of airway, supply of oxygen, and appropriate ventilation. To prevent further damage, it is necessary to protect the cervical vertebrae. If patients experience respiratory difficulty or suffer from subcutaneous emphysema, on-the-scene rescuers must recognize the possibility of damage to the airway, provide first-aid, and transport the patient to hospital. If there are any suspicious symptoms of airway damage, according to the literature, early fiberoptic intubation or emergency tracheostomy should be performed.3,4,9
As these techniques are rarely familiar to pre-hospital rescuers in the field, rescuers must present a detailed description of the patient`s condition upon arrival at hospital to assure that fiberoptic endoscopy or emergency tracheostomy is prepared to promptly secure the patient’s airway. In the case reported here, the patient with suspected tracheal damage arrived without enough preparation for emergency surgical airway, and Ambu bagging was started. Subcutaneous emphysema worsened over time, and cardiac arrest occurred.
During the breathing phase of bagging, pressure sufficient to raise the chest wall must be maintained. If air leaks out when the trachea is ruptured, pneumomediastinum, pneumothorax, and subcutaneous emphysema may be exacerbated. An increase in pressure on the thoracic cage can reduce venous return as well as ventilation and cause diastolic filling, resulting in phenomena such as cardiac tamponade. 10
In the case reported here, the immediate blind endotracheal intubation was performed using laryngoscopy during CPR, and fortunately, endotracheal intubation was successful, avoiding false passage. On follow-up CT images, the tip of the tube was located above the ruptured trachea, and the Murphy`s eye formed a passageway where air flowed through the lower part of the ruptured trachea. In the literature, blind endotracheal intubation is to be avoided. Such procedures can result in false passage, which can accelerate tracheal damage.5,8 In patients with laryngotracheal injury with respiratory distress, if tracheal intubation is necessary, a fiberoptic endoscopy should be performed. If tracheal intubation is not possible, emergency tracheostomy should be performed.
If the rupture area of the trachea may be large or completely separated, cardiac arrest may occur as in this case. Endotracheal intubation by direct laryngoscopy or video-assisted laryngoscopy should be avoided if the trachea is completely ruptured. It is less likely to be successful and may cause more damage. In a situation where a cardiac arrest occurs, it is considered that a tracheotomy, directly accessible to the lower part of the damaged trachea, is more effective than the fiberoptic intubation.
Conclusion
With laryngotracheal injury, it is important to immediately identify the condition of patients at the scene and promptly transport patients to hospital. Patients with such damage frequently suffer from difficulty in respiration and subcutaneous emphysema. At the pre-hospital level, based on the symptoms, EMT needs to focus on fast recognition of airway damage and transfer to a hospital where there are appropriate medical personnel and devices. The patient’s condition may deteriorate rapidly. At the hospital level, focus should be on securing the airway. Various approaches are available to accomplish this, such as the use of endoscope devices or emergency tracheostomy. In conclusion, it is necessary to have seamless communication and proper preparation at the pre-hospital and hospital levels.
Footnotes
Acknowledgements
H.H.J. made contributions to conception, design, and participate in drafting the article. J.T.P. acquired and interpreted data. J.S.O., S.M.C., Y.Y.K., and Y.M.O. participated in revising it critically for important intellectual content. K.H.C. gave final approval of the version to be submitted and any revised version. All authors read and approved final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data supporting the conclusions of this article are included within the article. Any queries regarding these data may be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymised patient information to be published in this article.