
Abstract
Massive propranolol overdose may result in severe cardiotoxicity. A 48-year-old female had consumed more than 5000 mg of propranolol. Despite high-dose insulin, intravenous sodium bicarbonate, glucagon and inotropic support, she became hypotensive and subsequently arrested. Following cardiopulmonary resuscitation, she had a return of spontaneous circulation but continued to experience refractory hypotension. Resuscitation continued with veno-arterial extracorporeal life support. Therapeutic plasma exchange was initiated to shorten time on extracorporeal life support. Extracorporeal life support was weaned off within 67 h, and she survived without neurological deficits. This records the largest propranolol overdose in recent years. When traditional antidotes are insufficient to prevent collapse, extracorporeal life support is a salvage therapy to maintain perfusion and reduce vasopressor requirements. As drug clearance is significantly prolonged, therapeutic plasma exchange can enhance removal of propranolol and reduce the time to extracorporeal life support removal. With increasing expertise and availability, extracorporeal life support should be considered early in patients who have overdosed with significant cardiotoxicity.
Introduction
Cases of massive propranolol overdose are extremely difficult to manage and associated with high mortality. Owing to its rarity, much of the evidence is low grade and based on animal models or case reports. The American Association of Poison Control Centers’ National Poison Data System reported that in 2016, 1 beta-blockers (including propranolol) were responsible for 10,577 single exposures.
Propranolol is a lipophilic, non-cardioselective beta-blocker and is highly protein bound drug with large volume of distribution (Vd; 4 L/kg). It is rapidly metabolised via hepatic extraction, resulting in a short half-life of 3–6 h. It is postulated that with overdose, hepatic metabolism of propranolol would be saturated, leading to prolonged elimination and consequent elevated serum levels. At supra-therapeutic doses, inhibition of myocardial sodium channels would result in a widened QRS interval and further increase the risk of ventricular dysrhythmias. Beta-adrenergic blockade would lead to atrioventricular nodal blockade and reduced contractility. Its ability to cross the blood–brain barrier would induce seizure and delirium, further complicating resuscitation.2 –4
When standard therapies and specific antidotes do not prove to be effective in the management of refractory cardiac arrest and refractory shock, extracorporeal life support (ECLS) has been described in case reports to be an effective rescue therapy. 5 Therapeutic plasma exchange (TPE) has been suggested as a method to reduce the half-life of propranolol6,7 and thereby to reduce the length of time the patient experiences toxicity.
Reported doses of propranolol poisoning so far range from death following 1500 mg and survival following 8000 mg. 8 These reports reflect the wide individual variability and the efficacies of various therapies in an overdose.
We report the use of ECLS and TPE in a patient with a massive overdose of propranolol in which the usual antidotes were insufficient to prevent circulatory collapse. The patient survived without neurological sequelae and was successfully transferred to the inpatient psychiatric ward.
Case report
A 48-year-old Chinese female with a history of major depression and previous suicide attempts had missed her routine appointment with the social worker. The social worker decided to visit her in her home where she confessed to taking a single ingestant of 504 tablets of propranolol (10 mg each) that day at 13:50 h. She agreed to go to the hospital’s emergency department (ED) for treatment and arrived 1 h after ingestion of the pills.
Upon arrival, she was fully alert and oriented. Her vitals were as follows: blood pressure (BP) 98/51 mmHg, pulse rate (PR) 47 beats/min, temperature 37.2°C, SpO2 97% and a respiratory rate (RR) of 18 breaths/min. She had no complaints of discomfort, her physical examination was unremarkable and she appeared well at rest.
Her initial electrocardiogram (ECG) (Figure 1) showed sinus bradycardia with a heart rate of 44 beats/min and a mildly prolonged QRS at 104 ms. Initial blood results were unremarkable except for a lactate 1.9 mmol/L. Her venous blood gas on arrival was pH 7.44, pCO2 34.7 mmHg, pO2 63.5 mmHg, HCO3 25 mmol/L, base excess 0.6, sodium 139.6, potassium 4.7. Blood propranolol levels were not taken as this did not have any immediate impact on her management.
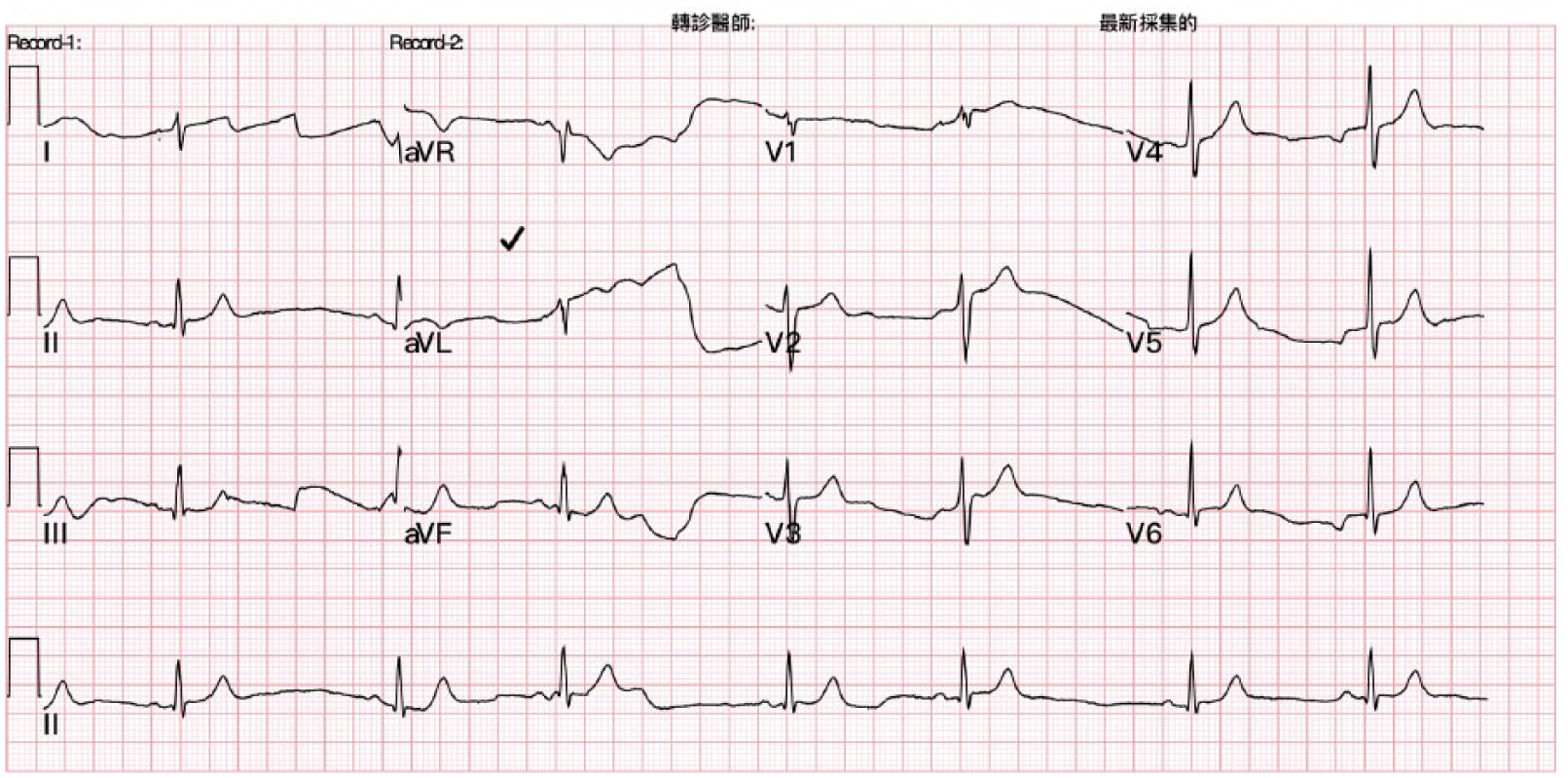
Initial electrocardiogram.
Within 45 min of arrival, the patient’s BP dropped to 70/50 mmHg, PR 40 beats/min, and she became progressively drowsier. She was treated with IV sodium bicarbonate 7% 120 mL, IV atropine 0.5 mg, IV adrenaline infusion, high-dose insulin therapy bolus of 60 U followed by 60 units/h and IV glucagon 5 mg bolus followed by further boluses of IV glucagon of 10 mg every 5–10 min with a combined dose of 90 mg. An infusion of 2 mg/h was also started lasting 4–5 h). Despite this treatment, she went into bradycardic pulseless electrical activity (PEA). Conventional cardiopulmonary resuscitation (CPR) for 2 min with IV adrenaline 1 mg push produced return of spontaneous circulation (ROSC). She was intubated during resuscitation.
Post-ROSC, she had a PR of 48 beats/min, and while her pulse was weakly palpable, prior to measurement of her BP, she went into a second episode of PEA. While CPR was ongoing, the ECLS team was activated. She underwent another 3 min of CPR before ROSC. At this point, her BP 97/56 mmHg and PR was 86 beats/min. An IV adrenaline and IV dopamine infusion were set up.
Upon arrival of the ECLS team, the patient developed a seizure lasting less than 1 min which was rapidly aborted with IV lorazepam 2 mg. Her systolic blood pressure remained more than 90 mmHg. In view of her history of massive propranolol overdose and 2 collapses within the ED, veno-arterial ECLS was commenced.
ECLS was set up within 2 h of arrival in ED and 1 h following her initial collapse. Utilising an open cut-down method, the patient’s right femoral artery was cannulated with a 17 Fr Maquet cannula, and a 21 Fr Maquet cannula was used for her right femoral vein. As per hospital protocol, a hybrid ECLS system was used – Pump–Maquet’s Rotaflow Centrifugal Pump, Oxygenator–Medos 7000LT (Figure 2). The initial settings were 2500 rpm resulting in a 2.0 L/min blood flow, FiO2 100% with gas flow at 2 L/min. Following the commencement of ECLS, the patient’s blood pressure was 149/51 mmHg. Venous blood gas results showed pH 7.369 pCO2 37.7 mmHg, pO2 51.1 mmHg, HCO3 21.9 mmol/L, base excess −4.8 mmol/L and lactate of 9.1 mmol/L. She underwent gastric lavage and activated charcoal was administered via a nasogastric tube.
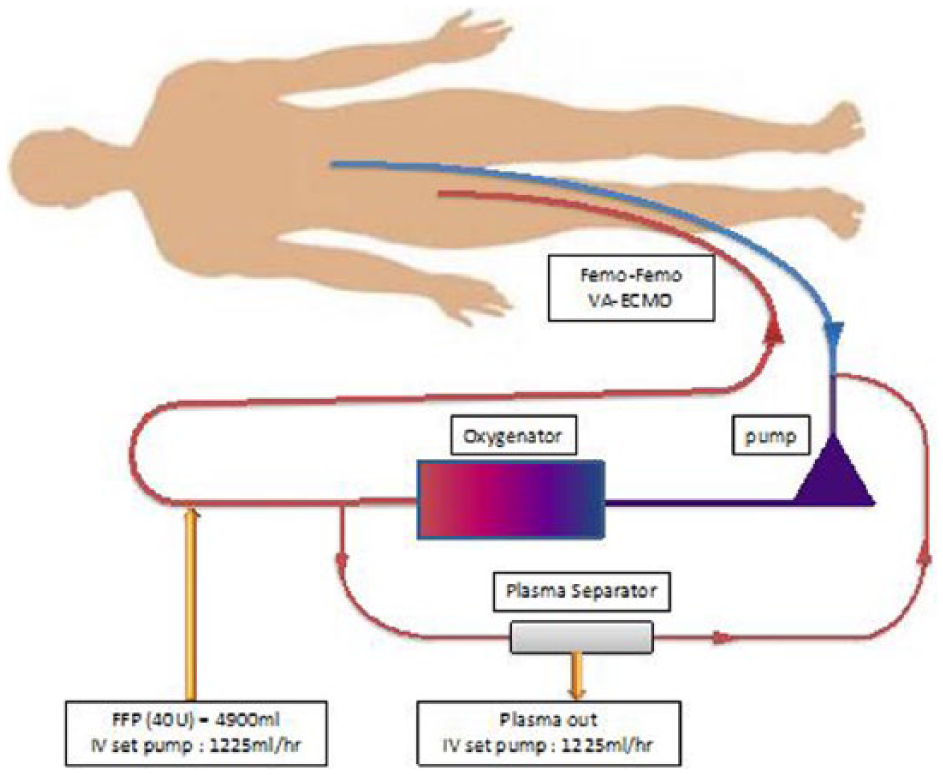
ECLS circuit with therapeutic plasma exchange.
As per hospital protocol, she received a pan-computed tomography scan which showed no significant abnormalities in her brain, chest and abdomen. Echocardiography revealed a moderately reduced left ventricular systolic function with an ejection fraction of 41.4%.
She was transferred to the cardiac intensive care unit (ICU). In the ICU, her BP was 149/95 mmHg. However, she remained bradycardic with a HR of 31 beats/min. ECG showed atrial fibrillation with a slow ventricular response. A transvenous pacemaker set at a rate of 60 beats/min was inserted with intermittent capture. While in the ICU, she received daily boluses of IV lipid emulsion (Lipovenoes MCT 20%) 250 mL over 3 days. Consciousness was gradually regained over the next 12 h.
24 h following ingestion of propranolol, the patient had a period of hypotension lasting 1 h with her systolic BP dropping from 110 mmHg to 69 mmHg. Her lactate rose to 5.1 mmol/L. ECLS flow was increased to 2.8 L/min, and TPE was initiated. We utilised a separator (Kawasumi Laboratories Plasmacure PE Plasma Separator) that was connected to the ECLS circuit at the pre-pump and post-pump sites (Figure 2). The flow through the plasma exchange circuit was set at 500 mL/min for a period of 4 h. Simultaneously, 40 units of fresh frozen plasma (calculated to be two times her blood plasma volume) was transfused. Following TPE, her blood pressure stabilised at systolic BP 135/90 mmHg. Her HR remained pacemaker-dependent at 60 beats/min. The improvement in BP and the reduced lactate to 1.66 mmol/L allowed tapering of IV dopamine infusion. ECLS flow was decreased back to 2.0 L/min. Bedside echocardiography showed an improved ejection fraction at 57.8%.
36 h following drug ingestion, her lactate levels were noted to rise again to 5.3 mmol/L. There was another prolonged drop in her BP to 75/40 mmHg. She was restarted on a second round of plasma exchange with the same protocol. Following this, her BP stabilised and lactate dropped to 2.2 mmol/L. The patient continued to display improvement in her hemodynamics, and she was weaned off the pacemaker. ECLS was removed within 67 h following insertion.
On day 5 of admission, she was extubated uneventfully and transferred to an inpatient psychiatric ward (Figure 3).
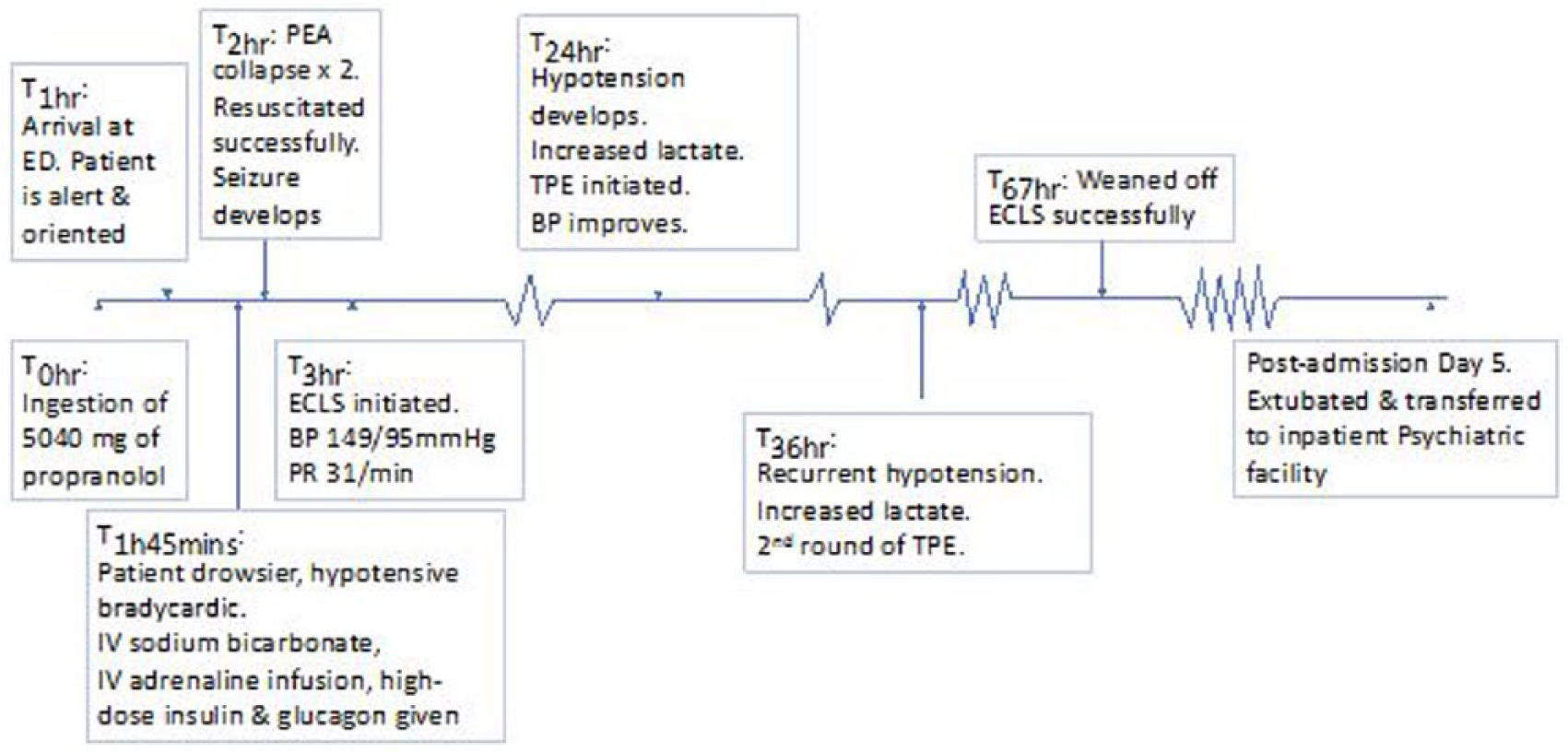
Events timeline.
Discussion
Case reports from more than a decade ago reported massive overdoses of propranolol up to 8000 mg. 8 We believe that this is the highest reported propranolol overdose in recent literature. Over the last decade, with advances in technology and expertise, ECLS has emerged as an exciting option of treating drug overdoses with cardiovascular collapse. 9
The lack of response to current antidotes
Both high-dose insulin euglycemia (HIE) therapy 10 and sodium bicarbonate 11 have been described in case reports to be useful in treatment of propranolol-induced cardiotoxicity. Insulin causes direct myocyte uptake of carbohydrates which increases inotropy, and it produces vasodilation which improves local microcirculation aiding systemic perfusion. 10 The extracellular sodium load from sodium bicarbonate contributes to directly overcome the sodium channel blockade. 12 Both these therapies were ineffective in our patient. In a canine model of propranolol toxicity, sodium bicarbonate failed to improve heart rate, mean arterial pressure and could not shorten the QRS interval. 13 Our patient’s ejection fraction was only moderately reduced and increasing inotropy with HIE thus had little effect. There are no official guidelines on insulin dosing in poison-induced cardiogenic shock and wide practice variation exists. 10 HIE is also labour intensive, requiring frequent checks of glucose and potassium. Beta-blocker overdoses are also more prone to hypoglycaemia than calcium channel overdoses, making HIE more dangerous. On arrival in our ED, our patient did not have evidence of hyponatremia, acidosis or a prolonged QRS complex which would indicate significant sodium-channel blockade. Ultimately, administration of HIE and sodium bicarbonate failed to prevent cardiovascular collapse.
The use of IV glucagon is controversial. Some studies have declared that it is ineffective, 14 while others continue to advocate the use of glucagon. 15 It acts by increasing cardiac inotropy by activating adenyl cyclase by a pathway separate from that of catecholamines, bypassing the beta-blockade. Most case reports used doses between 4 mg and 80 mg. 14 We had administered a massive dose of IV glucagon (total 100 mg in separate boluses), in the process, depleting our hospital’s stock. Likewise, this treatment proved ineffective in preventing PEA arrest.
The myriad of options available for propranolol overdose could risk causing an unnecessary distraction from early utilisation of ECLS. Many of these treatment regimens are unfamiliar to both ED and ICU staff leading to practical difficulties and unease in administration.
Early initiation of extracorporeal life support
In centres that are ECLS-competent, we believe that for patients in whom there is a given history of massive overdose and evidence of significant cardiotoxicity, ECLS should be considered early as one of the rescue therapies.
From other case reports, we note that ECLS is often initiated later in the patient’s time course in hospital, usually in the ICU instead of the ED.5,16 These patients may suffer from repeated arrests prior to ECLS. The reluctance to initiate ECLS may be related to the high complication rate or the huge resources needed.16 –18 Late initiation of ECLS often means increased stress during insertion of the vascular cannulas. Resuscitation scenarios have been shown to be associated with a higher failure rate of cannula insertion. 19 In a retrospective French study of 17 patients with cardiac arrest from drug overdose, 59% had significant vascular complications. 9
In a patient with multidrug overdose including beta-blockers who had collapsed, 5 ECLS had been initiated only much later in the ICU when all other treatment options had been exhausted. Although the patient survived to discharge, he was significantly neurologically impaired. In another case report, Kolcz et al. 7 reported commencing ECLS for a patient with propranolol and verapamil poisoning after 120 min of CPR when the patient had fixed and dilated pupils. While using ECLS has produced incredible results even in apparently moribund patients, 18 delayed initiation of ECLS would have definite implications on neurological outcomes. Nowhere is this better seen than in the overall more favourable neurological outcomes for in-hospital cardiac arrests when compared to out-of-hospital cardiac arrests 20 as the former usually has ECLS initiated earlier.
The expertise in utilising ECLS while CPR is ongoing is increasing. A recently published study reported a prevalence of 10% of cannulation-related vascular injury 21 where the large majority of these injuries were salvageable and did not require amputation. The placement of an antegrade reperfusion catheter further serves to reduce the chance of distal limb ischaemia. In centres with sufficient expertise, we believe that it is prime-time for ECLS to be first line therapy for massive overdoses with cardiotoxic drugs. Once the patient is deemed to have severe cardiotoxicity as evidenced by cardiovascular collapse or refractory hypotension, we believe ECLS should be initiated as soon as possible, prior to further transfer of the patient to another location within the hospital.
Decreasing time on ECLS: therapeutic plasma exchange
Kolcz et al. 7 had shown that TPE could decrease the time to eliminate propranolol. We implemented TPE because of the high plasma protein-binding capabilities (>80%) and high volume of distribution (>0.2 L/kg body weight) of propranolol. Moreover, lowering of plasma levels provided by the TPE could limit cardiotoxicity and provide good conditions for cardiac function recovery.
In massive overdose, it is likely that clearance of propranolol no longer obeys first order kinetics. Kolcz et al. 7 had reported time to off ECLS was 70 h – also utilising plasma exchange. In our case, aided by plasma exchange, we managed to wean off ECLS within 67 h. The prolonged requirement of ECLS was likely to be due to the effect of propranolol or its active metabolite. Myocardial stunning was a less likely possibility as the patient had regained good ejection fraction within 24 h of drug ingestion, and yet she suffered from bouts of hypotension. In animal experiments, propranolol was shown to cause arterial dilatation and venodilatation, 22 this decrease in peripheral vascular resistance and the decrease in afterload could explain the prolonged hypotension that the patient experienced despite good cardiac function.
It should be noted that most studies conducted on propranolol’s clinical properties are more than 30 years old at therapeutic doses, and little is known the toxico-kinetics of this drug. Given the current widespread use of this drug and its highly toxic effects, urgent research is required to update our understanding of propranolol’s toxico-kinetics.
Conclusion
In institutions where ECLS can be initiated quickly and safely, patients with significant drug-induced cardiac toxicity should be started early on ECLS.
ECLS is an essential component of salvage therapy in massive propranolol poisoning. TPE can be used in the treatment of refractory shock to lower the duration of time on ECLS.
Footnotes
Acknowledgements
We would like to acknowledge the contributions from Dr Huang Tao-Ming for his input into this case report.Both CLW and DMRH prepared and edited the first draft and obtained the figures. CYS reviewed the first draft and gave inputs which were incorporated into later editions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Human rights
This is an anonymised case report that does not violate human rights.
Availability of data and materials
The patient’s clinical information was largely obtained from computer records. Where records were not clear, clarification was sought with treating physicians.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethical approval
This is an anonymised case report that does not require ethics approval.