
Abstract
Introduction:
Refractory ventricular fibrillation is not uncommon and can be extremely difficult to abort. There is currently no standard guideline to effectively manage this electrical storm.
Case Presentation:
We hereby present the first successful reported use of dual simultaneous external defibrillation on a patient with refractory ventricular fibrillation in Hong Kong.
Conclusion:
Given the numerous successful cases with intact neurology in literature, dual simultaneous external defibrillation should be employed in indicated patients.
Keywords
Introduction
Between 1 August 2012 and 31 July 2013 in Hong Kong, there were more than 5000 cases of out of hospital cardiac arrest with only 2.3% of the cases surviving to hospital discharge 1. Current resuscitation guideline emphasizes on high quality cardiopulmonary resuscitation (CPR), administration of adrenaline and amiodarone, and early defibrillation on shockable rhythms. However, there are patients with ventricular fibrillation (VF) that remain refractory despite repeated attempts of standard practice. We hereby present the first successful reported use of dual simultaneous external defibrillation (DSED) on a patient with refractory ventricular fibrillation in Hong Kong.
Case presentation
A middle-aged obese smoker with no history of chronic illness presented to our emergency department with cardiac arrest. The patient complained of chest pain at 19:45 and the patient was found to be in ventricular fibrillation when the ambulance officer arrived at 20:00. In addition to intraosseous adrenaline, cardiopulmonary resuscitation (CPR) was started with four times of defibrillation given from Philips HeartStart FR3 (Philips Healthcare, Andover, Massachusetts). The patient was still in ventricular fibrillation upon arrival in our resuscitation room at 20:15 (Figure 1(a)). As a result, five boluses of adrenaline, two boluses of amiodarone, 70 mg of lignocaine, and four times of defibrillation ranging from 150 to 200 J biphasic by a Nihon Kohden TEC-5531K (Nihon Kohden Corporation, Shinjuku-ku, Tokyo) were provided. The patient’s ventricular fibrillation remained refractory. In view of this, dual simultaneous external defibrillation (DSED) was attempted with 200 J biphasic set on each Nihon Kohden TEC-5531K defibrillator (Nihon Kohden Corporation) at 20:28 (Figure 2). Rhythm was then converted out of ventricular fibrillation (VF) at 20:29 with blood pressure measurable (110/86 mmHg) by 20:33. Electrocardiogram showed an accelerated junctional rhythm with occasional ventricular ectopic beats (Figure 1(b)). Diffuse ST elevation was noted over lead I, aVR, aVL, and precordial leads with reciprocal ST depression over lead II, III, and aVF. The patient’s high sensitive troponin I, creatine kinase, and serum potassium levels were 28,777 ng/L, 1723 IU/L, and 2.9 mmol/L, respectively. All in all, this was suggestive of left main or triple-vessel occlusion.
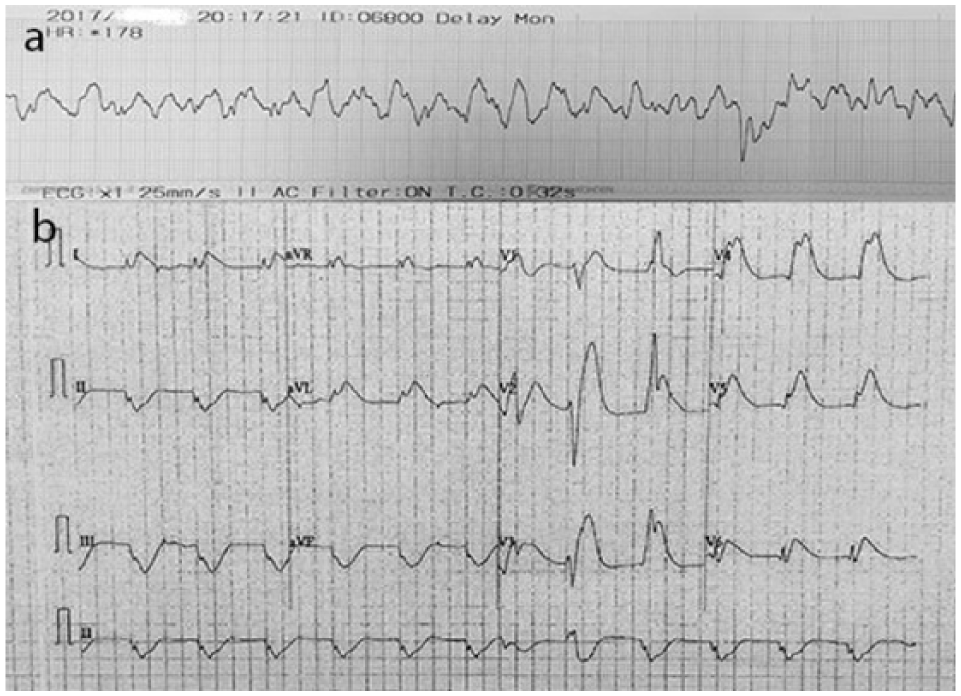
(a) Ventricular fibrillation was recorded on arrival to resuscitation room. (b) 12-Lead electrocardiogram after return of spontaneous circulation demonstrated an accelerated junctional rhythm with occasional ventricular ectopic beats. Diffuse ST elevation was noted over lead I, aVR, aVL, and precordial leads with reciprocal ST depression over lead II, III, and aVF, suggestive of left main or triple-vessel occlusion.

Examples of placing the defibrillator pads for dual simultaneous external defibrillation. (a) Method 1: without overlapping the pads, place the second set of external defibrillator pads right next to the first anteroapical set. This is also the placement we used for our patient. (b) Method 2: place one set of defibrillator pads anteroapically, and the second set anteroposteriorly.
An intensivist was consulted and emergency coronary angiogram and percutaneous coronary intervention (PCI) were performed. Coronary angiogram illustrated three-vessel disease; emergency PCI to the culprit left anterior descending artery was performed subsequently. Multiple CPR and defibrillation were required due to very frequent intraoperative VF arrest. High sensitive troponin I level was raised to 382,496 ng/L after PCI. The patient’s post-PCI blood pressure remained low and intra-aortic balloon bump (IABP) was inserted.
The patient was later able to wean off inotrope and IABP, and targeted temperature management was provided. Nevertheless, the patient’s Glasgow Coma Score remained 3/15 and finally succumbed on day 5 due to refractory pulseless ventricular tachycardia.
Discussion
Dual simultaneous or sequential external defibrillation was first mentioned in human in a case series in 1994. 2 All five patients of 2990 consecutive patients in routine electrophysiologic studies who experienced refractory VF were successfully resuscitated using DSED after unsuccessful standard defibrillation. Thereafter, there are numerous case reports worldwide demonstrating the success of this technique with neurologically intact survival;3–5 and as a result, several emergency medical services systems have begun to implement DSED.6–8 In Cabañas et al.’s case series, 6 return of spontaneous circulation was achieved in 7 out of 10 patients, but no survivors at the end. However, this study was criticized by Merlin et al. 7 of the delayed application of DSED (DSED was only initiated after 6.5 single shocks, or 35 minutes or more of CPR in patients with refractory ventricular fibrillation). In Merlin et al.’s case series, five out of seven patients with refractory VF were converted after DSED and three survived to discharge with no or minimal neurological disability. Its resuscitation mean time was 34.3 min before first DSED, mean number of single shocks was 5.4 prior to DSED, and a mean of 2 DSED shocks was delivered. However, a later retrospective cohort analysis showed no statistically significant difference in the primary outcome of neurologically intact survival between the DSED group and the standard defibrillation group. 8 In the presence of conflicting data of only case reports and case series, the true effect of DSED remains unknown without a properly designed prospective study.
Various mechanisms were hypothesized for the improved conversion of VF by DSED. In reality, the two defibrillators are discharged asynchronously or sequentially despite our best attempt to synchronize their actions. This prolongs the defibrillation duration through the fibrillating myocardium. In turn, the first shock lowers the threshold for the second shock to successfully depolarize the already sensitized myocardial cells. 9 Another theory is that the total energy delivered may be increased when the two defibrillators are discharged nearly at the same time, which may overcome limiting factors such as a larger BMI, poorly placed electrodes, and air in the lungs,10,11 and convert VF. Finally, an emerging theory is that a second set of pads may provide an improved vector of the energy discharge compared to the traditional placement. Shock vector aligning with the ventricular septum has a higher defibrillation success rate; hence, placing another set of pads increases the chance of optimal orientation. 12
Putting together, DSED bears functional resemblance to a multiphasic defibrillator, which is currently available, but uncommon, in the market. It was demonstrated that quadriphasic waveform was superior to triphasic waveform, and in turn, triphasic waveform was superior to biphasic waveform for transthoracic defibrillation in porcine model especially on those simulated with high impedances. 13 In a biphasic defibrillator, the addition of a negative phase removes the residual membrane potential and results in less refibrillation. Thus, the additional phases could remove residual membrane charge and stabilize postshock membrane potential more effectively, resulting in higher defibrillation success.
In our case, it took us 13 min before initiating DSED (28 min if timed from first VF recorded by ambulance officer). There were eight standard shocks delivered prior to the use of DSED, thus prolonging the total downtime to around 33 min (four standard shocks and 18 min of downtime in resuscitation room). Compared to the literature, if we only include the time the patient was in resuscitation room, our team was extremely decisive to initiate DSED. Nevertheless, as refractory VF is rare, it took us time to bring in another defibrillator and set up an extra set of pads on our patient.
The use of DSED is definitely novel in our locality. To this date, its utility is still questioned due to the lack of a proper study, and the possibility of damaging the defibrillator exists. 14 However, indicated patients definitely deserve one last try with this technique given numerous successful case reports. Despite successful return of spontaneous circulation in our case, areas such as effectiveness, timing, pads placement, and compatibility of defibrillators remain to be explored.
Footnotes
Acknowledgements
The authors would like to thank all the nurses and supporting staff for the complex resuscitation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
It was not possible to obtain informed consent from the patient because they are deceased, and every effort was made to obtain informed consent from the patient’s relatives. The case report has therefore been anonymised as far as possible.