
Abstract
Fracture and aspiration of tracheostomy tube is a rare late complication of the tracheostomized patient. We report a case of a 30-year-old male patient, who was tracheostomized 2 years ago for prolonged ventilation secondary to organophosphorus poisoning. He presented with history of minimal cough without any respiratory distress and was otherwise hemodynamically stable. The chest x-ray showed a metal tube lodged in the left main bronchus. The aspirated tracheostomy tube was removed by flexible bronchoscopy without any complications. Through this case, the authors highlight the need for proper care of a tracheostomy tube and also a rare complication of tracheostomy tube.
Introduction
A tracheostomy is defined as opening of the trachea and placing a tracheostomy tube to provide appropriate ventilation for patients 1 and is a common airway procedure done for life support. Although the procedure is safe with a mortality rate of less than 5%, 2 complications can occur, which can be categorized into early and late complications. Early complications are hemorrhage, pneumothorax, and obstruction of tracheostomy tube and wound infections. Late complications are granuloma formation, airway scarring, erosion of the innominate artery, and tracheoesophageal fistula. 3 While several complications have been reported, the most common complication resulting in an airway foreign body is fracture of the tube. Fracture of the metallic tracheostomy tube is, however, a rare occurrence. 4 Published reports of fractured tracheostomy tube presenting as foreign body in tracheobronchial tree are few.5–7
Here, we report the case of a 30-year-old male patient with accidental aspiration of tracheostomy tube, with no respiratory distress, which was removed using flexible bronchoscopy.
Case presentation
A 30-year-old male patient presented to the Emergency Medicine Department with a history of aspiration of the outer cuff of the tracheostomy tube accidentally while coughing. Patient was tracheostomized 2 years ago after organophosphorus consumption in view of prolonged ventilation. The patient was discharged from the hospital after 3 weeks of hospitalization with a metal tracheostomy tube. He was advised appropriate follow-up in the ENT clinic. The patient failed to follow-up for the next 2 years and was self-cleaning the tube as instructed by the ENT physician. After 1 year, patient changed the entire tracheostomy tube by himself. The current tracheostomy tube was 1 year old by the time of presentation.
On the day of presentation, the patient had removed the inner tube for cleaning. When the patient inhaled after coughing, the tube of the outer cannula broke from the neck plate and lodged itself into the left bronchus (Images 1 and 2).
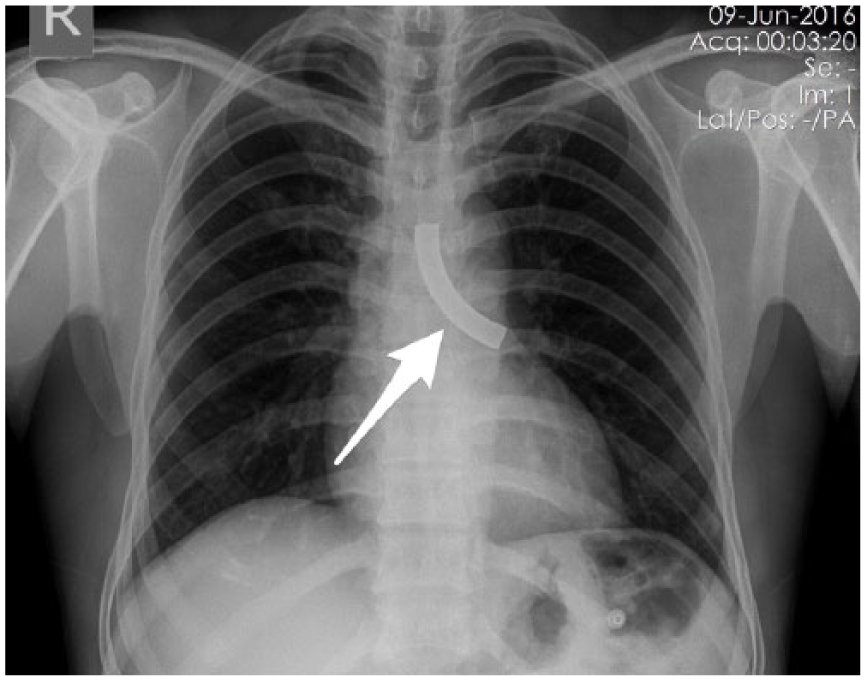
Plain chest x-ray PA view showing aspirated tracheostomy tube in the left main bronchus.

Lateral chest x-ray showing aspirated tracheostomy tube.
The patient presented to the Emergency Medicine Department with a mild productive cough with minimal sputum production and was not in respiratory distress. On examination, the patient was found to be conscious, oriented, and obeying commands. The heart rate was 98/min, respiratory rate 20/min, a room air saturation of 98%, blood pressure of 110/70 mm Hg, and was afebrile. The systemic examination revealed no abnormality. A lateral and anteroposterior (AP) chest x-ray was taken, which revealed the aspirated tracheostomy tube in the left main bronchus. A chest medicine consult was taken, and the patient was shifted for flexible bronchoscopy, under local lidocaine spray and minimal procedural sedation. The aspirated tube was removed through stoma (Image 3).

Image showing the broken neck plate.
Post procedure, the patient was hemodynamically stable and a new metal tracheostomy tube was inserted and the patient was admitted for observation observed for 2 days. The patient had an uncomplicated inpatient stay and was discharged from the hospital on the third day.
Discussion
Tracheobronchial foreign body complications related to tracheostomy tube are infrequent. Tracheostomy tube fracture can be a life-threatening emergency requiring precise and prompt management. The first case report of a fractured tracheostomy tube was in 1960 by Bassoe and Boe 5 and since then this complication has been published in medical literature from time to time. The largest series of fractured tracheostomy tubes reported to date by Gupta in 1987 was of nine cases reported over a period of about 8 years. 6 Patients are usually misdiagnosed as having chronic respiratory ailments before the definite diagnosis is made.
Tracheostomy tubes are made from metal, polyvinyl chloride (PVC), and silicone. Most portex tracheostomy tubes are disposable and cannot be reused. Metallic tubes are more suitable and reliable for prolonged use as they can be washed, boiled, and are unlikely to fracture. Traditional metallic tracheostomy tubes are made from silver, steel, copper, or zinc, all of which are prone to corrosion by alkaline tracheal secretions. In the present modern era, metallic tracheostomy tubes are made from stainless steel which contains steel and chromium. Stainless steel does not stain, corrode, or rust as easily as ordinary steel. Despite this, a majority of the cases of fractured tracheostomy tubes reported in literature have been metallic. 1
In this case, the fracture was between neck plate and the tube, the reasons for which could be lack of proper cleaning, no follow-up with primary ENT physician which led to not able to recognize the rusting of the tube parts. The management requires an AP view chest x-ray and bronchoscopy for removal of the tube. In this case, the tube was extracted with flexible bronchoscopy without any complications; however, literature points to the use of rigid bronchoscope also.
When aspirated patient can present with choking or/and respiratory distress in acute conditions and in chronic cases, they might present with prolonged cough, pneumonia, and bronchiectasis. In our case, patient neither had respiratory distress nor choking symptoms.
There are no adequate guidelines regarding the tracheostomy tube care, based on the case reports and literature review, we advise following recommendations:
Clean the inner cannula daily or every other day. More frequent cleaning may be required depending upon the amount and nature of the patient’s secretions.9,10
Patients should be provided with two sets of inner tracheostomy tubes at home. Alternative use of these sets may reduce wear and tear of the tube.
Regular checkups are important. Follow-up systems should be established in any hospital that is involved in caring for patients who undergo a tracheostomy. 8
Patients and caregivers should be properly trained in the care of tracheostomy patients and the complications that could occur. A periodic review of the techniques may be helpful. 8
In the case of an emergency, immediate hospital contact and a good referral system are critical for the early detection and management of these complications. 8
Family should be told during cardiopulmonary resuscitation (CPR), breathing must be performed mouth to tracheostomy tube not mouth to mouth.
Conclusion
Fracture of the tracheostomy tube is rare, but if it happens, it can lead to serious complications. Mortality related to tracheostomy tube is less than 5%. Patient may present with symptoms like minimal productive cough and not always present with respiratory distress. Flexible bronchoscopy is a good initial modality to remove the aspirated tube with minimal sedation. Regular follow-up, appropriate cleaning, and scheduled replacement of the tracheostomy tube can prevent this complication.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All the required data have been shared with the reviewers. No information has been withheld.
Informed consent
The case report at no point divulges any personal information of the patient/sex/religion or any other sensitive which may compromise the patient or the treatment.