
Abstract
Introduction:
Neutropenic enterocolitis is a life-threatening gastrointestinal complication of neutropenia that is rarely seen in adults. Neutropenic enterocolitis is more common in oncology patients, especially in those with leukemia. Antithyroid drugs are widely used to treat hyperthyroidism, but they can rarely cause agranulocytosis. Although the pathophysiology is not well understood, high clinical suspicion and immediate and appropriate treatment responses are essential to reduce the mortality rate of neutropenic enterocolitis.
Case presentation:
We present a case of a 57-year-old male patient who developed neutropenic enterocolitis as a result of agranulocytosis caused by the use of propylthiouracil. He had history of hyperthyroidism and was on propylthiouracil. He presented to the emergency department with abdominal pain but eventually died due to rapid deterioration of sepsis and multiple organ failure despite medical and surgical treatment.
Discussion:
Thioamides can cause agranulocytosis which can result in serious complication including neutropenic enterocolitis. Complete blood count must be monitored in patients receiving thioamides, and these patients should be educated on symptoms of agranulocytosis.
Conclusion:
Since patients with neutropenic enterocolitis are often evaluated first by emergency physicians, emergency physicians must be vigilant for neutropenic enterocolitis in patients with neutropenia and abdominal pain.
Introduction
Neutropenic enterocolitis (NE)/typhlitis/necrotizing enterocolitis/ileocecal syndrome is a serious and potentially fatal inflammatory gastrointestinal complication that is rarely seen in neutropenic patients. This condition involves cecum, ascending colon, and terminal ileum, and is characterized by edema, ulceration, focal hemorrhage, and the development of necrosis and perforation in the affected bowel segment.1–3 Patients can present with nonspecific gastrointestinal symptoms or specific symptoms that may quickly progress to sepsis and multiple organ failure.2,4 NE is common in the pediatric age group but is rare in adults. It is more commonly observed in patients receiving immunosuppressive therapy due to aplastic anemia, lymphoma, human immunodeficiency virus infection, leukemia, drugs causing granulocytopenia, solid organ tumors, and transplant.2,5–7 Treatment of NE is uncertain and controversial, although its early diagnosis and treatment are crucial for survival. The mortality and morbidity rates of this condition are very high,2,8 in fact, mortality rates have been reported to vary between 0.8% and 26% or between 50% and 100%.4,5,8 Antithyroid drugs are widely used in hyperthyroidism, and leukopenia may develop in 1%–5% of patients using these drugs. However, this adverse effect is usually benign, and the presence of leukopenia does not increase the risk of agranulocytosis and infection. It has been reported that agranulocytosis (absolute neutrophil count (ANC) < 500/mm3) is rare and is present in 0.2%–0.5% of patients using antithyroid drugs.9,10
In this report, we present a case of a male patient, with history of hyperthyroidism and was treated with propylthiouracil (PTU), developed agranulocytosis, and NE. He deteriorated quickly and died despite medical and surgical treatments. This case is very rare and is almost never seen in the literature.
Case presentation
A 57-year-old male patient presented to our emergency department with 2-day history of abdominal pain. The patient’s history revealed that he used 800 mg PTU three times a day for hyperthyroidism, which was stopped by the physician and replaced with levothyroxine 5 days before he attended our department due to hypothyroidism. His latest blood tests, which were performed 1 month before the day of attendance, showed normal white blood cell (WBC) count and ANC.
On physical examination, his general condition was good. His vitals were stable, and he was cooperative and oriented. However, he was anxious, weak, and had bilateral exophthalmos. There was tenderness in all quadrants of his abdomen, especially in the epigastric region; but there were no guarding and no rebound tenderness. Other systemic examinations were normal. WBC was 1300/mm3 (normal range: 4300–10,300/mm3) and ANC was 100/mm3 (normal range: 2100–6100/mm3). Chest and abdominal x-rays were normal. Fluid infusion was given, and nasogastric and foley catheters were inserted. Since ultrasonography (US) showed bowel wall thickening involving several segments of the bowel, intravenous (IV) contrast abdominal computed tomography (CT) was performed. It revealed thickening of the wall of the cecum, ileum, and ascending colon, and an increase in contamination in the pericecal mesenteric adipose tissue (Figures 1 and 2). After 6 h, the patient developed shock, with blood pressure 74/56 mm Hg, heart rate 130/min, respiratory rate 40/min, and desaturation with oxygen saturation 92% on room air. He was taken to the intensive care unit. Rapid fluid infusion and IV pressor support were initiated, and broad spectrum IV antibiotic was given. After 1 h, his breathing became very shallow, and he was intubated. He also developed acute abdomen, and emergency operation was performed. Exploration during surgery revealed a necrotizing intestinal segment starting approximately 15 cm proximal to the ileocecal valve and extending to the medial transverse colon. Right hemicolectomy and ileocolostomy were performed. Histology revealed multiple ulcerations in the cecum, intestinal wall necrosis, submucosal hemorrhage, and vascular congestion. The patient died 6 h after the surgery due to sepsis and multiple organ failure.

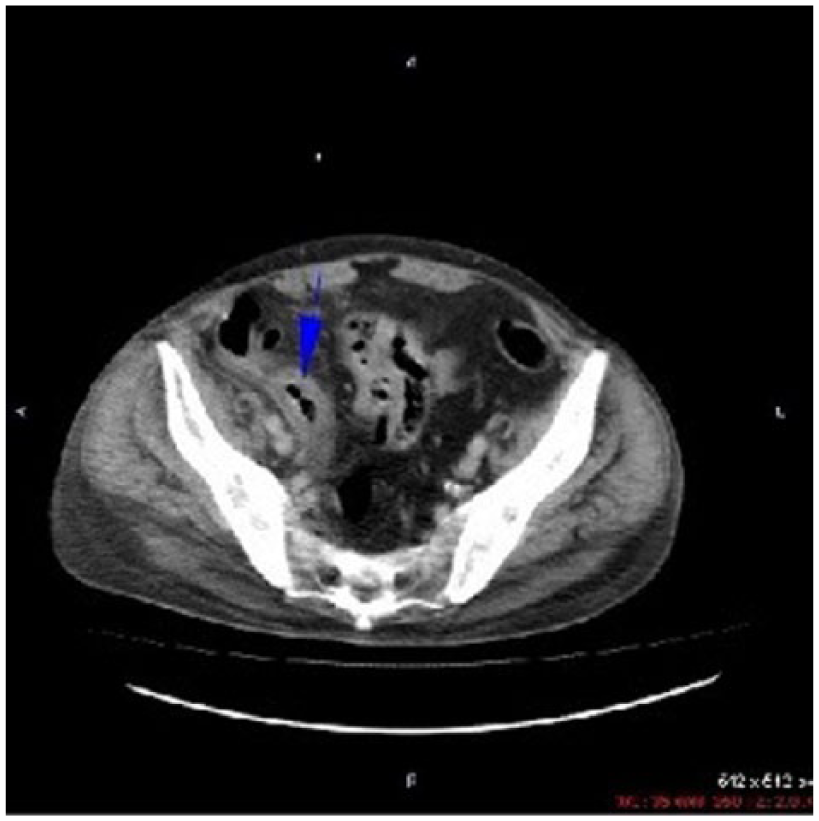
Contrast-enhanced CT of the abdomen demonstrated marked bowel wall thickening of the cecum and terminal ileum with obliteration of the lumen (blue arrow). In addition, inflammation of the pericecal fat tissue was observed (white arrow).
Increase in density around pericecal mesenteric fat tissue, and wall thickening around cecum were also shown on contrast-enhanced CT of the abdomen (blue arrow).
Discussion
NE is a rare inflammatory disease of the gastrointestinal tract with an extremely mortal prognosis. However, it occurs more frequently in recent years due to the increased use of aggressive chemotherapy (especially in patients with leukemia).1,5,7 In addition to aggressive chemotherapy, prolonged neutropenia is also an important risk factor for NE.3,11
The pathophysiology of NE has not been fully elucidated, and there are no clear diagnostic criteria and no definitive treatment. It is believed to be caused by an impaired host defense against mucosal injury and intestinal organisms, and is classified as a syndrome rather than as a specific disease. 12 The cecum is almost always affected, but the disease may also spread to the terminal ileum and the colon. It is believed that the disease first affects the cecum because of its spreading capacity and its limited blood supply. Intestinal wall or mucosal edema, mucosal ulcerations, focal hemorrhage, and mucosal or transmural necrosis may be seen in its pathology.5,7 There were numerous case reports and case series illustrated cases of NE across a spectrum of patients with or without cancer. 4 The clinical findings and symptoms of NE vary greatly, and therefore, its diagnosis may be difficult. 2 NE should be suspected in any neutropenic patient presenting with fever and abdominal pain. The most common presenting symptom is vague cramp-like abdominal pain, which was seen in our case.2,13 Other presenting symptoms include abdominal distension, nausea, vomiting, and watery or bloody diarrhea. Pseudomembranous colitis, colonic pseudoobstruction, acute appendicitis, ischemic colitis, inflammatory bowel disease, and infectious colitis should also be considered in the differential diagnosis. 5
Imaging may be useful in the diagnosis of NE.4,5 Plain radiography is usually normal or nonspecific,4,5,13,14 while barium enema and colonoscopy are not recommended, since they may lead to perforation. 5 US and CT are the best imaging methods to diagnose NE. US is usually the first choice in patients who are hemodynamically unstable since it is fast and can be performed at the bedside. 4 Abdominal CT findings in NE include a greater than 4 mm increase in bowel wall thickness, fluid-filled dilated cecum, paracolic fluid accumulation, and inflammation in the peripheral mesenteric adipose tissue. Abdominal CT is also useful for determining complications, such as pneumatosis intestinalis, pneumoperitoneum, intra-abdominal free fluid, and abscess, and evaluating the response to treatment.4,5
Antithyroid drugs are widely used to treat hyperthyroidism. However, the thioamide group of antithyroid drugs, including PTU, methimazole, and carbimazole, can cause hematologic side effects ranging from mild leukopenia to agranulocytosis and aplastic anemia. Agranulocytosis is a rare but a very serious and life-threatening complication, and may arise suddenly and severely. It has been reported that 0.37% of patients using PTU and 0.35% of patients using methimazole have severe agranulocytosis.15,16 While agranulocytosis occurs most frequently in the first 2–3 months of drug use, it can also be observed after a year of drug use or even longer. 17 Direct toxic effects of the drugs and a series of mechanisms caused by immunological reactions are considered to be responsible in antithyroid drug-induced agranulocytosis. 18 The risk of fatal complications and susceptibility to infection is higher in NE patients with ANC < 100/mm3 than in patients with ANC > 100/mm3. 16 In our case, the ANC was 100/mm3.
Prospective randomized studies or high-quality retrospective studies regarding the treatment of NE are not present in the literature. For this reason, the treatment is controversial, and there is no specific treatment algorithm. Because of the wide range of clinical presentations, the best treatment approach is patient-specific, individualized treatment. 5 Primary treatment for patients with NE should not be different from the treatment for patients with acute sepsis and hemodynamic disturbance. Conservative approaches, including appropriate vascular access, broad spectrum IV antibiotics including antipseudomonal antibiotics, bowel rest, nasogastric drainage, total parenteral nutrition, and neutrophil count normalization, should be applied without delay.1,4,5,14 In patients with antithyroid-induced agranulocytosis, antithyroid drugs should be stopped immediately, and patients should be hospitalized. The granulocyte count usually returns to normal within 2 weeks of drug discontinuation. Physicians should be careful when prescribing antithyroid drugs, since cross-reaction between thioamides is frequent after the improvement of agranulocytosis.2,9,16 Moreover, several clinical studies have indicated that recombinant granulocyte colony–stimulating factor accelerates healing and infection control. 19 Despite aggressive supportive therapy, surgical treatment for NE is necessary in cases with worsening clinical picture, resistant gastrointestinal hemorrhage, intra-abdominal perforation, and peritonitis.2,4,5,8,14 Our patient underwent surgical treatment since his clinical picture progressed rapidly from mild abdominal pain to septic shock, despite the early conservative approach.
Conclusion
Thioamides can cause agranulocytosis which can result in serious complication including NE. Complete blood count must be monitored in patients receiving thioamides and these patients should be educated on symptoms of agranulocytosis. Since patients with NE are often evaluated first by emergency physicians, emergency physicians must be vigilant for NE in patients with neutropenia and abdominal pain.
Footnotes
Acknowledgements
The authors wish to thank Tanzer Korkmaz, MD, who assisted with obtaining reference materials and editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials can be accessed from hospital data processing system.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Ethical approval
This case study was carried out in accordance with ethical guidelines and WMA declaration of Helsinki.
Human rights
Written informed consent was obtained from patient’s son.