
Abstract
Objective:
Gossypiboma is a cotton matrix mass that is left behind in the body during the surgical operation. A retained surgical swab (gossypiboma) is a rare but an important complication of an intrathoracic surgery.
Case Presentation:
Intrathoracic gossypiboma was reported with cough and dyspnea, 7 years after coronary artery bypass surgery. Chest radiography and thorax computed tomography images’ findings are discussed. The patient was operated in the hospital where he had undergone coronary artery bypass surgery. The patient recovered uneventfully with complete resolution of all clinical symptoms on follow-up.
Discussion:
The patients may be symptomatic for a long period after the operation and the clinical presentation of gossypibomas may be acute or delayed. Radiological methods, especially computerized tomography, are very helpful in diagnosis.
Conclusion:
The use of radiopaque marked sponges in surgical procedures may prevent the formation of gossypiboma.
Introduction
Gossypiboma (textiloma) is a term used to describe a mass in the body that is composed of a cotton matrix surrounded by a foreign body reaction. The word gossypiboma derives from the gossypium, it means cotton in Latin. The real incidence is difficult to determine from the reviewed literature because some cases remain asymptomatic and some are not reported because of the medical and legal implications.
The patients are usually asymptomatic for a long period after the initial operation. Radiological manifestations varied according to the locations and chronicities of the gauze sponges. The incidence has been estimated as between 1 in 1000 and 1 in 3000 procedures. 1 We report a case of an intrathoracic gossypiboma resulting in cough and dyspnea, 7 years after coronary artery bypass surgery.
Case report
A 72-year-old male patient admitted to our hospital emergency service with dyspnea and recurrent cough without sputum, hemoptysis, or fever. He had undergone coronary artery bypass surgery 7 years ago. He was normotensive, nondiabetic, and non-smoking. General physical examination revealed a sternotomy scar. Physical examination of the chest revealed diminished breath sounds. Routine hematological, biochemical investigations, and pulmonary function test were within normal limits. Serum inflammatory markers were normal, and the patient’s symptoms were not consistent with infection.
In echocardiograpic examination, left ventricle function was normal, and external pressure to the left ventricle wall was determined.
Chest radiographs revealed that increasing of cardiothoracic ratio, and there was a round soft tissue density in 9.5 cm in diameter adjacent to the left ventricle. Also there were linear densities in string shape in the mass (Figure 1). Thorax computed tomography (CT) scan confirmed the findings. Linear strings were in metallic density. Internal density of the mass was 14 HU (fluid) (Figures 2 and 3). The mass was dissected and removed in hospital where he had undergone coronary artery bypass surgery. The patient recovered uneventfully with complete resolution of all clinical symptoms on follow-up.
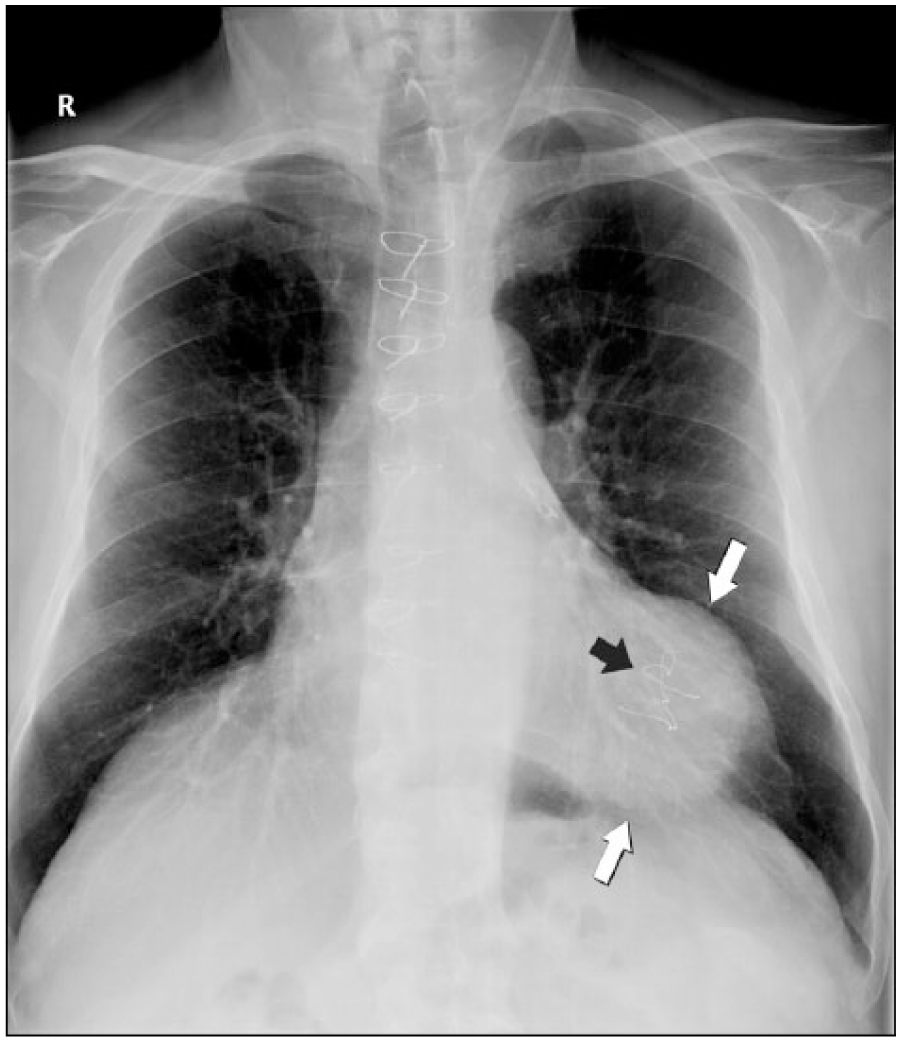
Increasing cardiothoracic ratio, round mass of 9.5 cm in diameter adjacent to the left ventricle (between white arrows) and linear densities in the mass (black arrow) are seen in the chest radiogram.
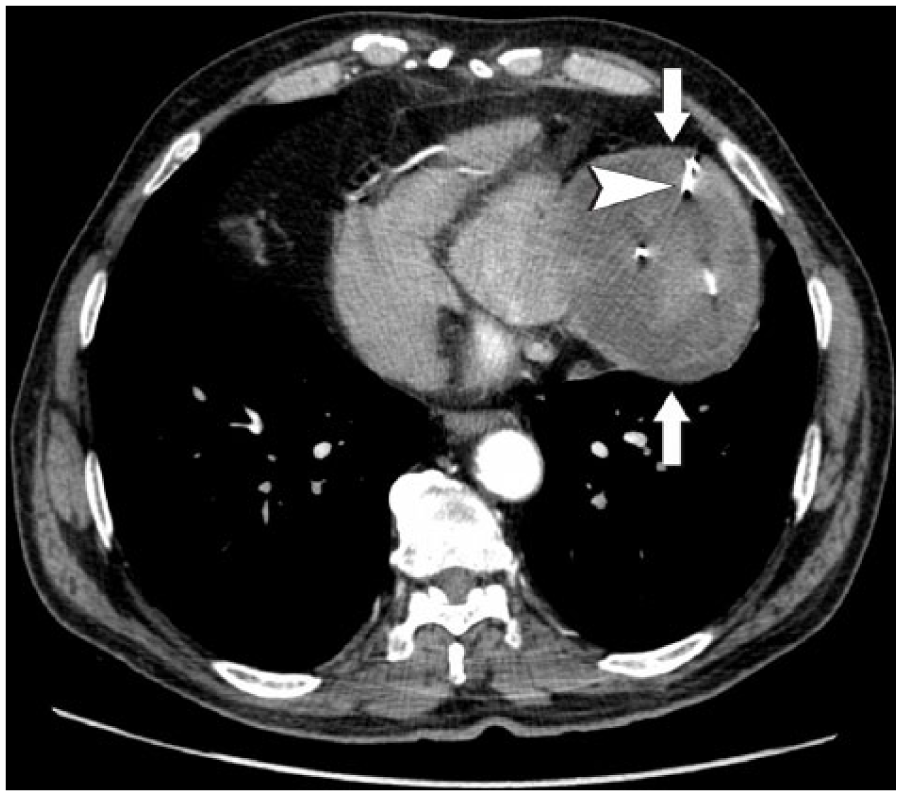
Metallic strings in fluid density mass are seen in thorax CT and reconstructed CT images. Arrow head shows metallic strings in the fluid collection and white arrows show border of the mass.
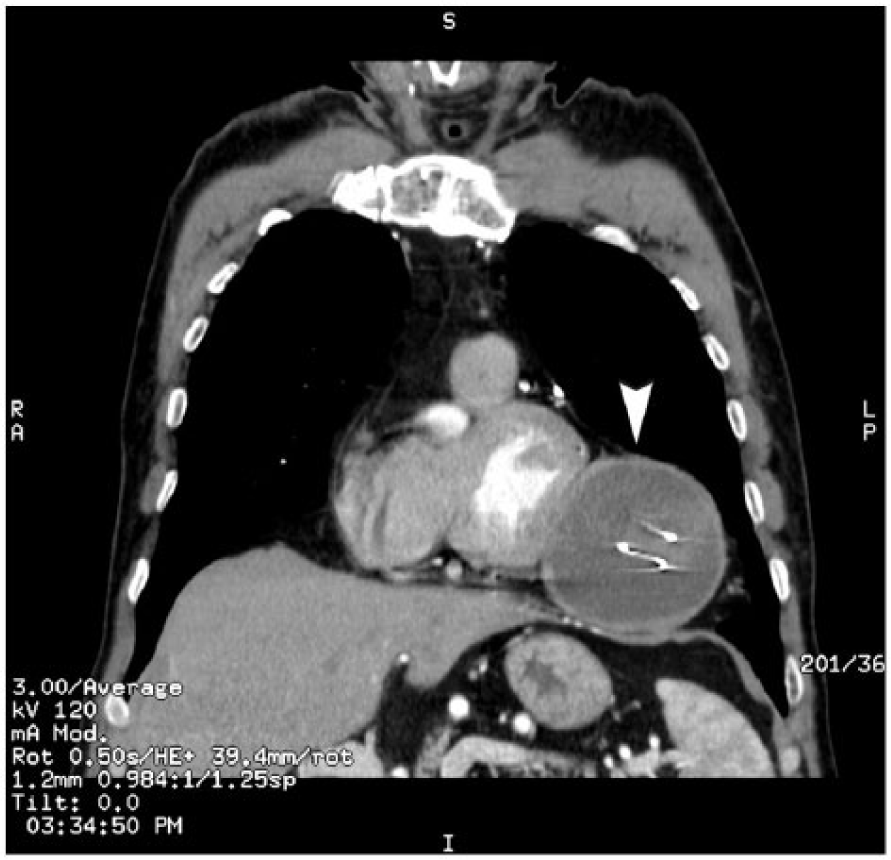
Metallic strings in fluid density mass are seen in thorax CT and reconstructed CT images. Arrow head shows the mass.
Discussion
The diagnosis of an intrathoracic gossypiboma can be easily missed because of its rare occurrence and low index of suspicion. 2 The clinical presentation of gossypibomas may be acute or delayed. Patients are usually asymptomatic for a long period after the operation. Gossypibomas are generally reported after abdominal laparotomy; however, it can occur following any surgical procedure. Gossypibomas were most commonly found in the abdomen (56%), pelvis (18%), and thorax (11%) with an average discovery time of 6–9 years after the procedure. 3 CT is the best method for diagnosis and evaluating complications. The manifestations of textilomas on CT change according to the locations and chronicities of the gauze sponges and the types of reactions that they cause in the body. The typical radiologic finding on CT is a predominantly high attenuation central mass with a spongiform pattern of air bubble and a hyperdense, well-enhancing rim in the early diagnosis. If diagnosis is late, radiographic findings may change, as in our case internal densities may transform to fluid image. In the early postoperative period, CT characteristically shows a well-defined intrathoracic soft tissue mass with a hyperdense rim, air bubbles, and high-density stripes. A differential diagnosis of gossypiboma in the early postoperative period includes hematoma and abscess. Differentiation from other masses, such as neoplasms or degenerated hydatid cysts, is difficult at this stage, even with the knowledge of the prior operation.
Exudative and aseptic fibrous reactions could be seen with gossypibomas. Adhesions, encapsulation, and a foreign body granuloma formation define the sequence of events seen in aseptic gossypiboma cases. In exudative gossypiboma, however, symptoms usually occur in early postoperative period, and infection findings may be due to secondary bacterial contamination. In our case, findings were found in late postoperative period pointing out aseptic fibrous reaction. Symptoms were seen according to the localization and size of gossypiboma. We believe that use of radiopaque marked sponges in surgical procedures, and a postoperative radiographic imaging could possibly detect the presence of the sponges, so gossypiboma formation may be prevented.
This case emphasizes consideration of gossypiboma in patients presenting with respiratory symptoms following thoracic surgery. The most important factor for preventing these events is the exact counting of sponges. During operations, all surgeons and assistants should check for retained surgical gauzes and count the number of gauzes used. With those efforts of regular counting of all instruments and use of radioopaque swabs, this avoidable error could be completely eradicated.
Footnotes
Acknowledgements
The authors like to thank to their patient for giving them opportunity to take him as their subject for their case study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was obtained from the patient for publication of this case.
Ethical approval
Ethical approval was taken from our hospital ethical committee.
Human rights
This case report was prepared in accordance with human rights.