
Abstract
Introduction:
Long QT syndrome accompanied by a seizure episode is often misdiagnosed as primary epilepsy. Although patients with Long QT syndrome who are misdiagnosed and improperly managed are likely to result in fatality, their first clinical manifestations are seizure episodes in many cases.
Case presentation:
A 17-year-old boy visited the emergency department with poorly controlled seizure during epilepsy treatment was found to have been misdiagnosed with epilepsy when he was 7 years old. His electrocardiography showed a prolonged QT interval. After careful re-evaluation, he was finally diagnosed with Long QT syndrome and recovered without any seizure episodes in the absence of anti-epileptic agents.
Discussion and conclusion:
Careful initial assessment including repetitive electrocardiography, when abnormal, is required for those who visit the emergency department with a seizure or who show no definite abnormalities in diagnostic work up process.
Introduction
Arrhythmogenic syncope accompanied by a seizure episode is often misdiagnosed as primary epilepsy. Therefore, careful initial assessment is required for those who visit the emergency department (ED) with a seizure. However, patients previously diagnosed with epilepsy are often not adequately assessed when they come to the ED with a seizure episode, which in many cases is the first symptom of long QT syndrome (LQTS). Failure to consider LQTS has been reported as a major cause of delay from initial symptoms to diagnosis. LQTS can lead to fatal ventricular arrhythmia, which requires appropriate assessment by the emergency physicians. A correct diagnosis is also important to prevent sudden death at a young age as well as to identify the proband of congenital LQTS. This case report presents a 17-year-old boy who visited the ED with seizures that had been misdiagnosed as epilepsy when he was 7 years. Now, 10 years later, he was diagnosed with congenital LQTS. We discuss why there was a delay in the diagnosis of LQTS in this case.
Case report
A 17 year-old boy visited the ED after a seizure episode. Before 10 years, he was diagnosed with epilepsy and was on medication until the morning of his visit to the ED. His last seizure episode had been 3 years prior. The night before coming to the ED, he had a seizure for 2 min. The next morning, he was admitted to the ED with another seizure, which lasted approximately 15 s. He was alert but slightly confused. His blood pressure was 124/74 mm Hg, and his heart rate was 81/min. He had no fever or neurologic deficit. He reported having chest pain and dizziness before the morning seizure episode. The seizure was accompanied by cyanosis and upward eyeball deviation. A 12-lead electrocardiography (ECG) showed a prolonged QT interval with a U wave (Figure 1: arrowhead). The heart rate was 75, and the QT/QTc interval by the manual calculation was 600/667 ms. Automatic calculation by the EKG machine measured 400/448 ms (Figure 1). After about 10 min, he complained of chest pain and dizziness, and a seizure was soon under way. The ECG monitor showed torsades de pointes (TdP) (Figure 2). TdP was repeated for a few seconds every 5 min and was accompanied by seizure. Repeated unstable TdP was converted by defibrillation in the ED. After intravenous injection of magnesium, he was transferred to the intensive care unit (ICU).
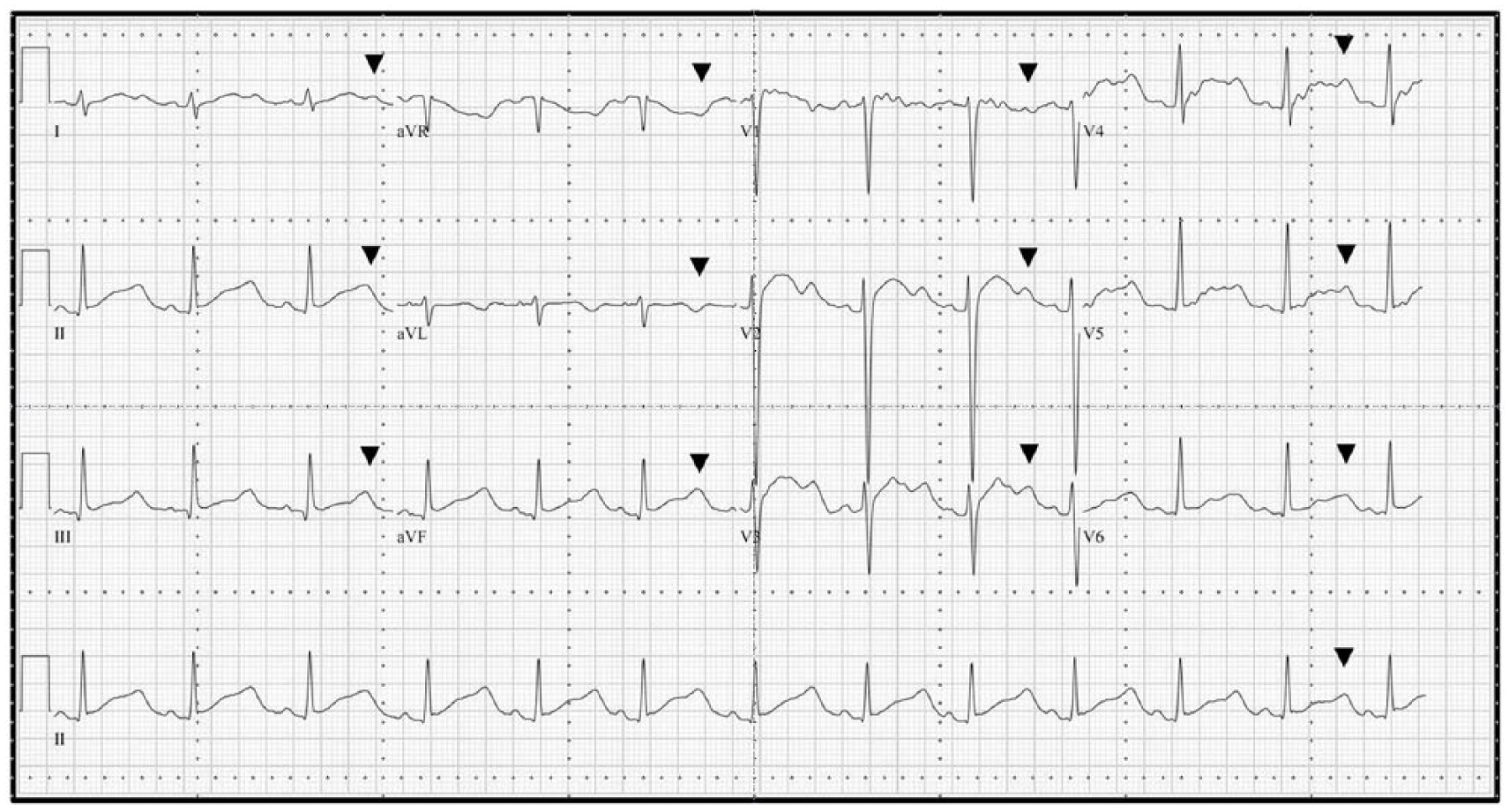
The 12-lead ECG before seizure in the ED; the arrowhead indicates a U wave.
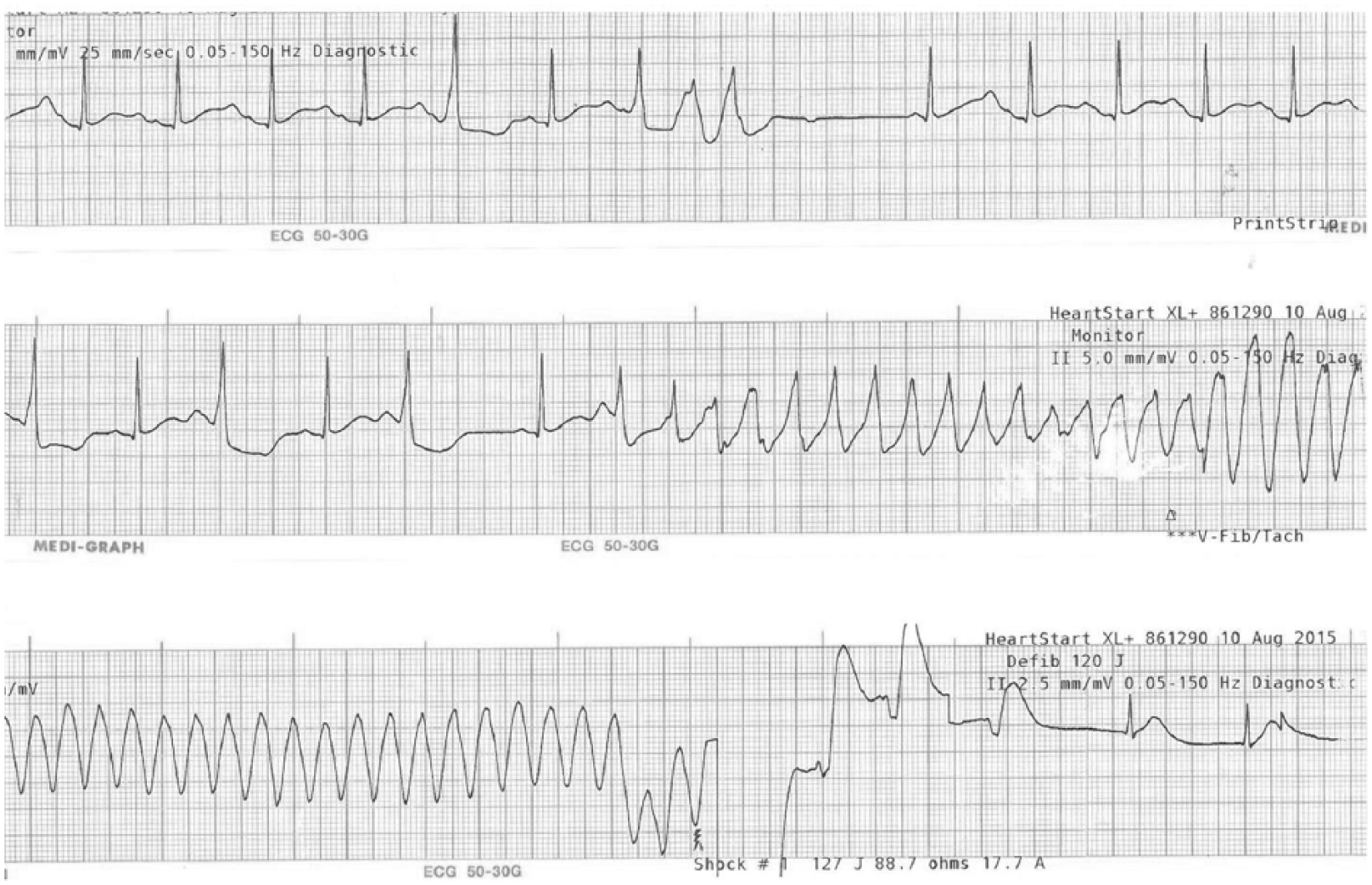
ECG monitoring during seizure in the ED.
In the ICU, the heart rate decreased after administration of oral propranolol, and TdP recurred frequently. The patient was started on intravenous isoproterenol and lidocaine; however, the TdP recurred intermittently. TdP stopped after a temporal pacemaker lead was inserted and paced at a rate of 80/min. After 2 weeks, the temporal pacemaker was removed. TdP was well controlled by oral propranolol without complications. A KCNH2 mutation was found in his genetic study, and he was diagnosed with genotype LQT2 congenital LQTS. He was discharged from the hospital with an implantable cardiac defibrillator after 4 weeks.
When the patient was 5 years old, he was admitted to an ED with fever and seizure that was diagnosed as a febrile seizure. His electroencephalogram and brain magnetic resonance imaging (MRI) were normal.
His first ECG was performed in the ED when he was 5 years old. The QT/QTc interval was measured as 400/554 ms, but the automatic calculation was measured as 324/449 ms (Figure 3). When he was 7 years old, he had a seizure episode after falling from a chair. He had been complaining of chest pain before the seizure episode. The seizure recurred several times, and he was diagnosed with epilepsy.
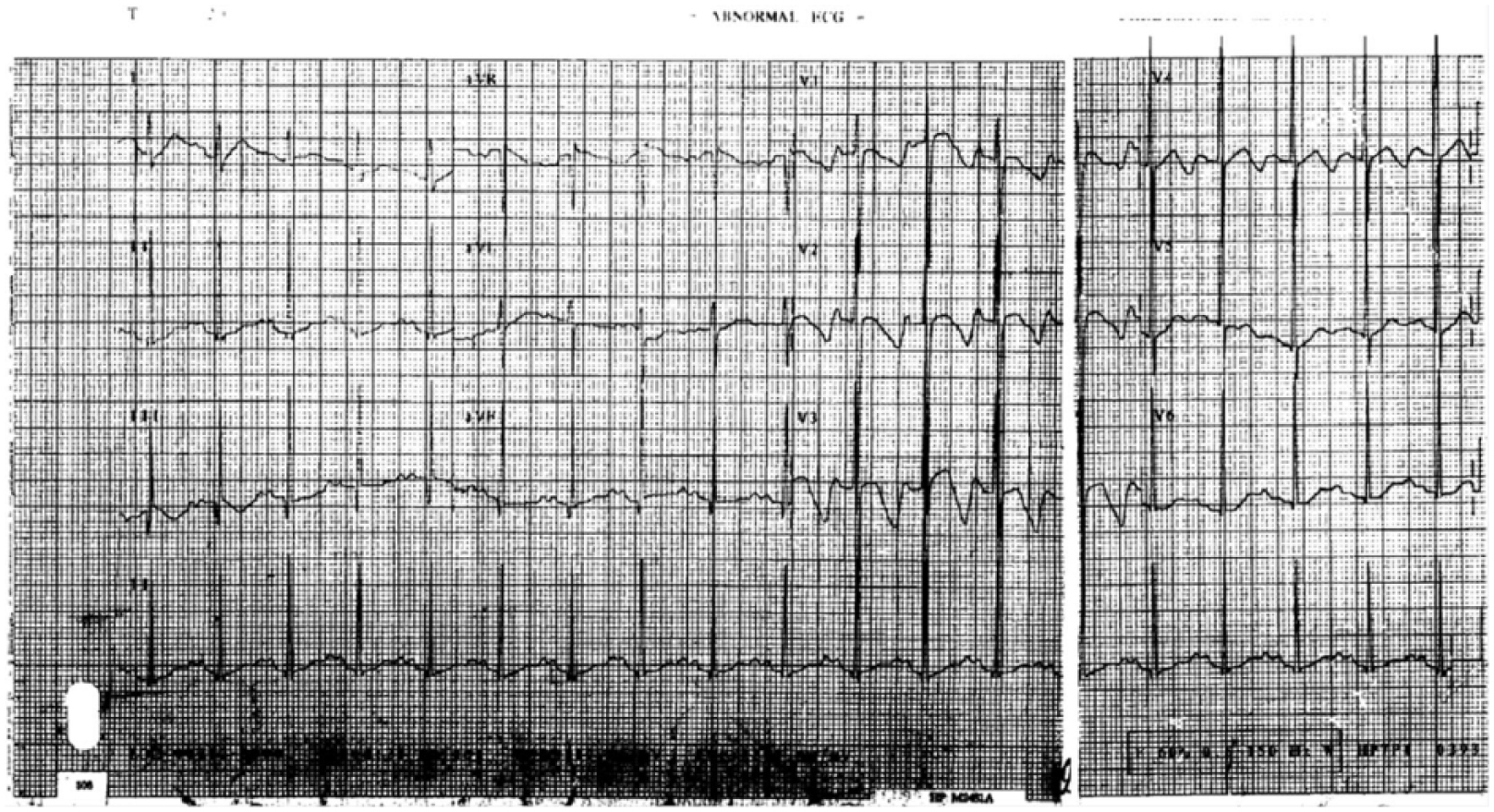
First ECG (10 years previously, at age 7).
Discussion
Seizure is a common cause of visits to the ED. In the United States each year, more than 1 million people—1% of all ED patients—visit EDs with seizure. 1 LQTS is a rare but fatal disease, and in many cases, the first symptom is a seizure. One study showed that a misdiagnosis of epilepsy in individuals with LQTS remained uncorrected for an average of 11.8 years, and seizure is present for a longer time than other LQTS symptoms. 2 Therefore, in patients who visit the ED with seizures, the possibility of LQTS should be considered. Our patient was diagnosed with LQTS 10 years after a visit to the ED with his first seizure.
A detailed medical history is important to rule out arrhythmogenic syncope in patients with seizure. Our patient complained of chest pain before every seizure episode; this can be a sign of syncope due to cardiac causes. 3 However, his symptoms, which also included postictal confusion, can be mistaken for those of epilepsy. 4 In addition, our patient was diagnosed with long QT syndrome type 2 (LQT2), which is more often misdiagnosed than long QT syndrome type 1 (LQT1) because it occurs at night or when the patient is resting. 5
In our case, ECG monitoring was crucial for the diagnosis of LQTS. Although the American College of Emergency Physicians recommends ECG when a first seizure occurs, there is no mention of the importance of the ECG in patients with a history of epilepsy. 6 ECG monitoring of patients with recurrent seizures in the ED is thought to be helpful in the diagnosis of LQTS.
The delay in diagnosis in our case was also caused by misinterpretation of the ECG. ECG was performed four times in the ED, and prolongation of the QTc interval was observed in all the recordings. However, the patient’s records contained no mention about QTc interval of the reading. QTc measurement appears to be simple, but it is reported that less than 50% of cardiologists and less than 40% of non-cardiologists interpret it correctly. 7 QT interval is measured from the beginning of the QRS complex to the ending point of the T wave. In addition, a large U wave should be included in the measurement of the QT interval. 4 In our patient, the QT interval is normal if it does not include a U wave. 8 The findings of an automatically interpreted QT interval can also cause confusion. Manual measurements are reported to be superior to automated measurements. The automatically measured QT interval in our patient was in the normal range.
A group of expert on LQTS proposed four guidelines for measuring QT interval:8,9
Use a limb leads that best reveal the end of the T wave;
Measure from beginning of QRS wave to the end of the T wave and include a U wave if it is large enough to be merged with T wave;
Measure the QT interval during peak plasma concentration of a QT-prolonging medication;
Adjust QT interval for heart rate.
A simple visual assessment of long QT is by comparing the length of QT interval to the length of two R waves. If the QT interval is more than half of the RR interval, long QT should be suspected.
The prevalence of LQTS is approximately 1 in 3000 and may be underestimated. 10 In most cases, the ED is the first place a patient with syncope or seizure episode will be seen by a physician. To avoid misdiagnosing LQTS patients, emergency physicians should obtain a detailed clinical history along with reliable interpretation of the QT interval.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Chung-Ang University Research Grants in 2013.
Availability of data and materials
This case report has no restrictions on the availability of data and materials.
Informed consent
The patient provided informed consent.
Ethical approval and human rights
All authors adhered to the Helsinki Declaration; patient confidentiality and anonymity were preserved.