
Abstract
Traumatic diaphragmatic rupture is relatively rare, and even more difficult to diagnose. Physical examination often fails to identify this injury, and basic investigation like chest x-ray can miss this half of the time. Although not part of standard FAST (focused assessment with sonography for trauma) ultrasound scan in trauma, bedside ultrasound has the potential to pick up this pathology. This case illustrates that ultrasound in trauma can go beyond standard E-FAST (extended FAST) protocol.
Introduction
Diagnosis of traumatic diaphragmatic rupture is often delayed due to lack of pathognomonic symptoms and signs. Although it is rare and overshadowed by associated injuries, delayed diagnosis with accompanied strangulation of herniated viscera will result in higher morbidity and mortality. 1
Clinical diagnosis of traumatic diaphragmatic rupture is difficult, so various diagnostic imaging modalities play central role for this purpose, and have been proposed in establishing preoperative diagnosis, including chest radiographs, computed tomography (CT), and magnetic resonance (MR) imaging. Among those, bedside ultrasound scan, as a specific modality mastered by emergency physician, can be used. Although not part of the E-FAST (extended FAST) examination, ultrasonographic diagnosis of traumatic diaphragmatic rupture is possible by taking it “beyond” by adding time in facilitating direct visualization continuity of the highly echogenic diaphragm through its capability of multidirectional images. 2
Case report
A 26-year-old woman, a restraint front-seat passenger, was involved in a motor vehicle accident. The car hit a lorry, and the front half was wrecked. On arrival to the emergency department, the patient had blood pressure of 96/56 mmHg, heart rate of 106 beats/min, respiratory rate of 36, and room oxygen saturation of 100% with face mask. She complained of right-sided chest pain and mild shortness of breath. There was a reduced air entry on the left side. Apart from that, she also complained of neck pain, pelvic pain, bilateral arm swelling and tenderness, and left leg pain.
The chest x-ray film showed right-lung contusion and fracture at 5th, 6th, and 9th ribs on the right side and 7th–10th ribs on the left side. E-FAST scan did show free fluid at Morrison’s pouch, no pericardial fluid, and minimal left pleural effusion. However, on further ultrasound interrogation of the left diaphragm, it did not show any continuity and no regular excursion. There was disruption at the left diaphragm (Figure 1) and two tube-like appearances at lower end of the screen suggestive of stomach or loops of bowels (Figure 2). CT showed left diaphragmatic defect at posterolateral aspect with stomach, omental fat and jejunum herniated into thoracic cavity, left lung collapsed with mild pleural effusion, and multiple rib fracture (Figure 3). The patient also sustained open-book pelvic fracture. She was taken to operating room for exploratory laparotomy and diaphragmatic repair.
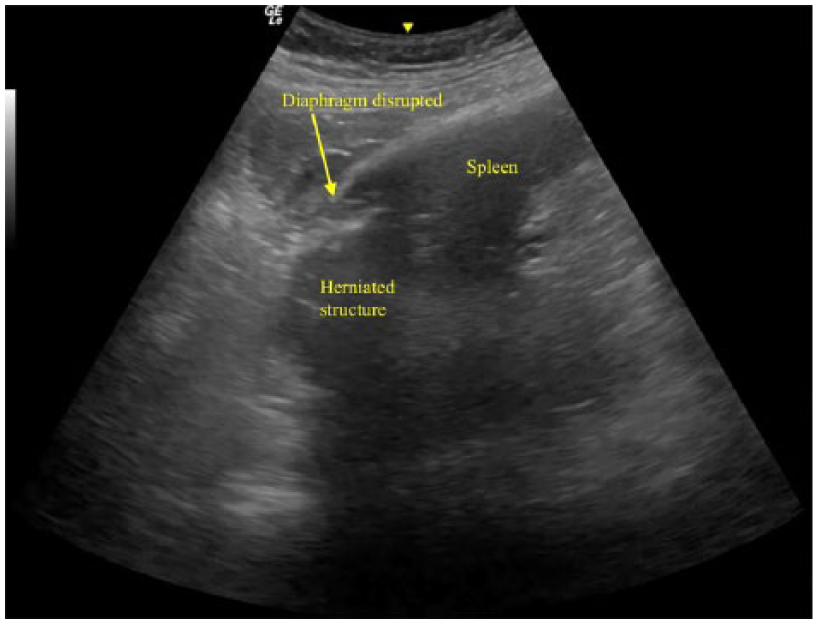
Ultrasound showing disrupted diaphragm with loop structures.
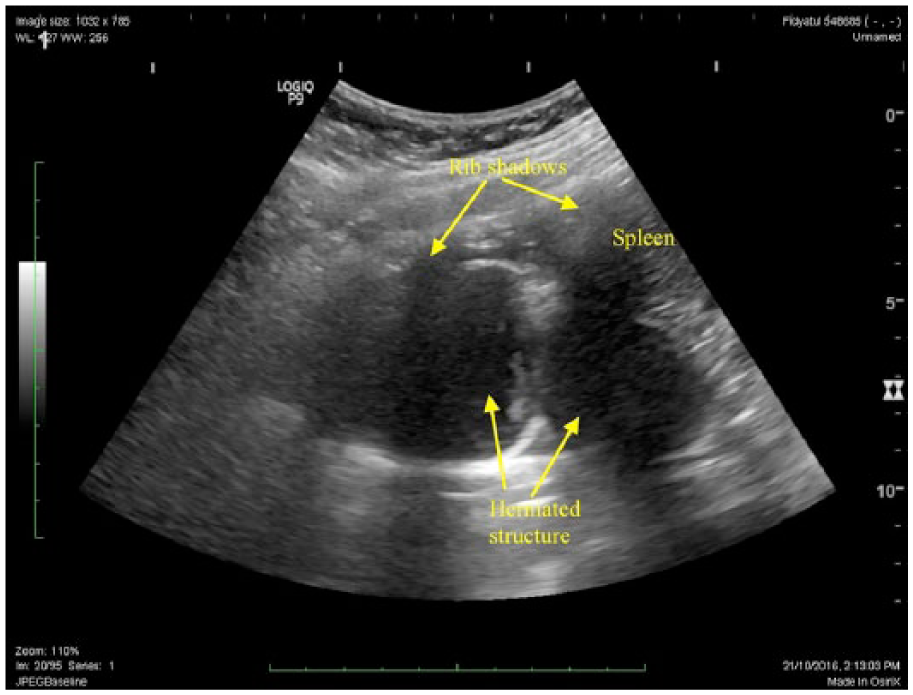
Ultrasound at left mid-axilla showing two rounded structures which could be either herniated stomach or loops of bowels.
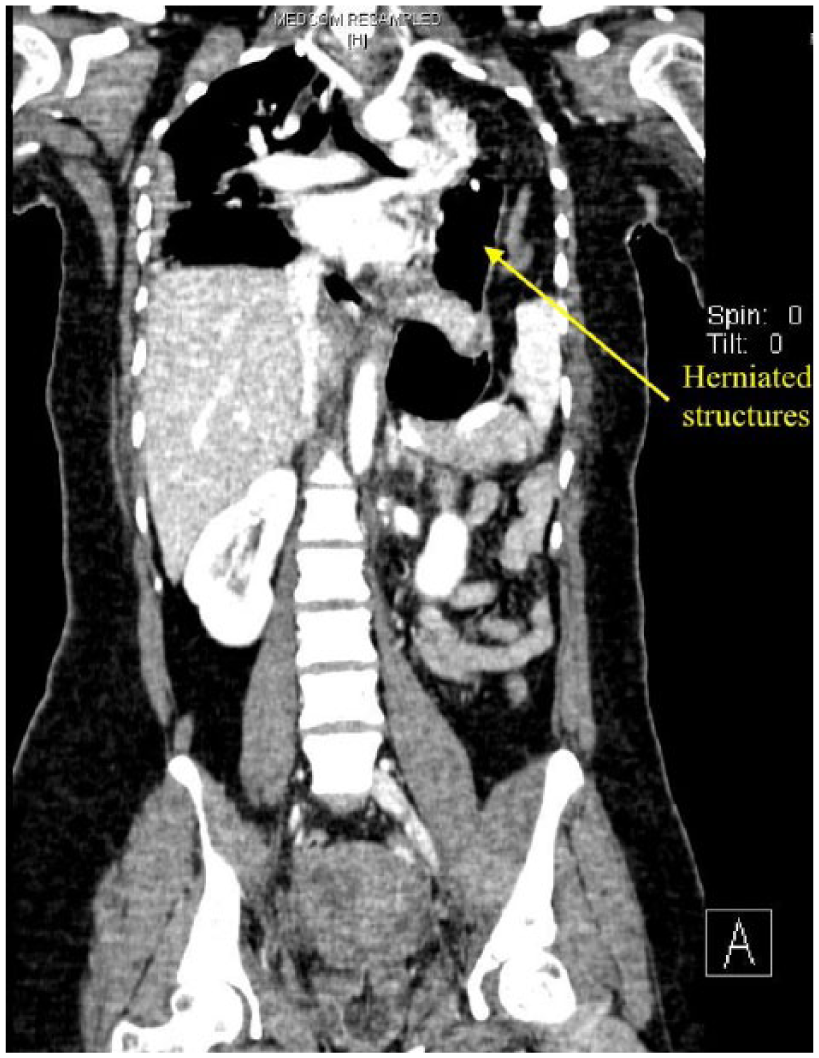
CT thorax showing herniated stomach with two tube structures representing what was seen on ultrasound.
Discussion
Traumatic diaphragmatic rupture is a serious condition that requires surgical repair. It is an uncommon injury with prevalence of 0.8%–1.6% of patient admitted with blunt injury. 3 It occurs more frequently on the left side because it is assumed that the liver plays a role in having a protective effect on the right side or that right-sided injury is underdiagnosed.4,5 Unfortunately, the diagnosis is often delayed because clinical and radiographic evaluations are insensitive. Initial plain radiographs have demonstrated sensitivities of 28%–65%, and CT has been shown to be 5%–84% sensitive. 6 As reports on ultrasound diagnosis are anecdotal, there is no figure on sensitivities.
Ultrasound is usually the first-line imaging modality performed in trauma patient admitted to the emergency department. Several reports in literature have described findings suggestive of diaphragmatic rupture. Kim et al. showed from their cases that the ruptured diaphragm was well demonstrated on ultrasonography because of the presence of fluid collection in the pleura or subphrenic spaces, and the appearance of the diaphragm was considered disrupted, non-visualized, or floating. Ultrasound is also helpful in detecting herniation of organs and structures in the peritoneal cavity through the diaphragmatic defect. Real-time ultrasonography aids in detecting bowel peristalsis and small bowel mucosal folds in cases of bowel herniation. 2 Right-sided diaphragmatic rupture is considered when presented with a “liver sliding” sign (hepatic parenchymal movement is seen against the parietal pleural surface when lung parenchyma is normally seen). 6
Having said that, there are several recognized limitations. Diaphragmatic rupture can be mimicked on ultrasonography by the presence of gas in the stomach and splenic flexure of the colon. Also, performance of ultrasonography can be limited by aeration of the lungs, subcutaneous emphysema, or overlying bandages and monitoring cable. 2 Bedside emergency ultrasonographic diagnosis of traumatic diaphragmatic rupture is to be a diagnostic value, with advantage of good accessibility and the drawback of being operator dependent. 7
CT can improve the accuracy of diagnosis and aid in direct visualization of the diaphragm. The sign of diaphragmatic defect on CT includes sudden interruption of diaphragmatic contour and intrathoracic position of abdominal organs or mesentery. Associated herniation of omental fat can also be correctly identified. 8
Traumatic diaphragmatic rupture is difficult to diagnose in polytrauma. E-FAST scan could be useful as a “rule” in diagnostic tool. 9 Many emergency physicians look for haemothorax during E-FAST scan by looking above the diaphragms, it is a simple thing to include a brief evaluation of diaphragm’s continuity, herniated abdominal content, or any sonographic signs suggestive of diaphragmatic rupture.
There is no literature available to suggest the learning curve or specific training to diagnose diaphragmatic rupture on ultrasound. But we believe that physicians who are comfortable with using ultrasound, if had previous encounter with a case, or exposure to the knowledge, would be able to detect the abnormality with ease. However, as per most point of care ultrasound, it is more specific than it is sensitive. Therefore, a negative scan cannot be used to rule out diaphragmatic rupture. The more important point is that a physician is able to pick up something abnormal and order a more appropriate investigation such as CT.
As the management of polytrauma patient is now moving toward whole body CT scan, the question arises whether performing point of care ultrasound such as the E-FAST protocol is really necessary. But the fact remains that due to availability and cost, this practice is mostly only routinely done in high-income developed countries. As such, ultrasound is still essential as an adjunct to trauma management for the rest.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Malaysian Ministry of Health for the permission to publish this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.