
Abstract
Oral contraceptives are widely used because of their reliability. Although oral contraceptives are known to increase the risk of thromboembolic events, there are extremely few reports of oral contraceptive–induced left ventricular thrombus. Herein, we report a 37-year-old non-smoking female, who had regularly taken oral contraceptives for 14 years, developed an anterior myocardial infarction concomitant with left ventricular thrombus, bilateral segmental renal infarctions, and lower limb ischemia. Medical treatment with a combination of dual antiplatelet therapy and anticoagulants completely relieved her symptoms.
Introduction
The wide use of oral contraceptives (OC) is based on their reliability. However, OC use is associated with an increased risk of venous and arterial thromboembolic events. 1 The majority of which are venous thrombosis events, especially peripheral venous thrombosis. OC-related arterial thromboembolic events are relatively uncommon, and generally comprise cerebral vascular events and ischemic heart diseases. 2 The present case report describes a long-term OC user who developed painless myocardial infarction (MI), concomitant with left ventricular (LV) thrombus formation, and multiple arterial embolism.
Case report
A 37-year-old non-pregnant woman presented to the emergency department with sudden onset of lower abdominal pain 1 h prior to arrival. She also complained of intermittent pain and numbness in the left leg for a few days. She denied having any chest pain or backache. She did not smoke. There was no significant past medical history. She reported regular intake of OC for 14 years. Her vital signs were stable upon arrival. Physical examination revealed lower abdominal tenderness without rebounding pain, as well as bilateral cool feet without detectable pulsations in the dorsalis pedis arteries. There was no deterioration in the muscle power of both lower limbs. Electrocardiography (ECG) revealed a sinus tachycardia, V1-V3 ST elevations, and deep Q waves on V1-V2 (Figure 1). The white blood cell count was 16,000/μL, the creatinine level was 1.27 mg/dL (reference range: 0.44–1.03 mg/dL), and the troponin-I level was 12.93 ng/mL (reference range: <0.5 ng/mL). Her creatine kinase was 135 U/L (reference range: 15–130 U/L), of which the MB fraction was 0%. All other blood tests were unremarkable. Given the suspicion of vascular events, a computed tomography was performed, which showed a LV thrombus (2.3 × 1.8 cm2) and bilateral segmental renal infarctions (Figure 2). Arterial duplex ultrasound of the lower extremities revealed total occlusions of the bilateral popliteal arteries. Due to the ST elevations on the ECG, a cardiologist was consulted. It was concluded that primary coronary intervention was not imperative due to the uncertain history of chest pain and the deep Q waves on the ECG. Cardiovascular surgeons were consulted for evaluating the necessity of surgical interventions for both LV thrombus and ischemic legs. They recommended medical treatment rather than an emergent surgical intervention, since there is a high rate of LV thrombus recurrence even after emergent surgical intervention. A two-dimensional echocardiography also disclosed a thrombus at apex of left ventricle, and an anteroseptal wall hypokinesis with preserved LV contractility. The patient received aspirin, clopidogrel and intravenous heparin immediately, and was admitted to the coronary care unit.
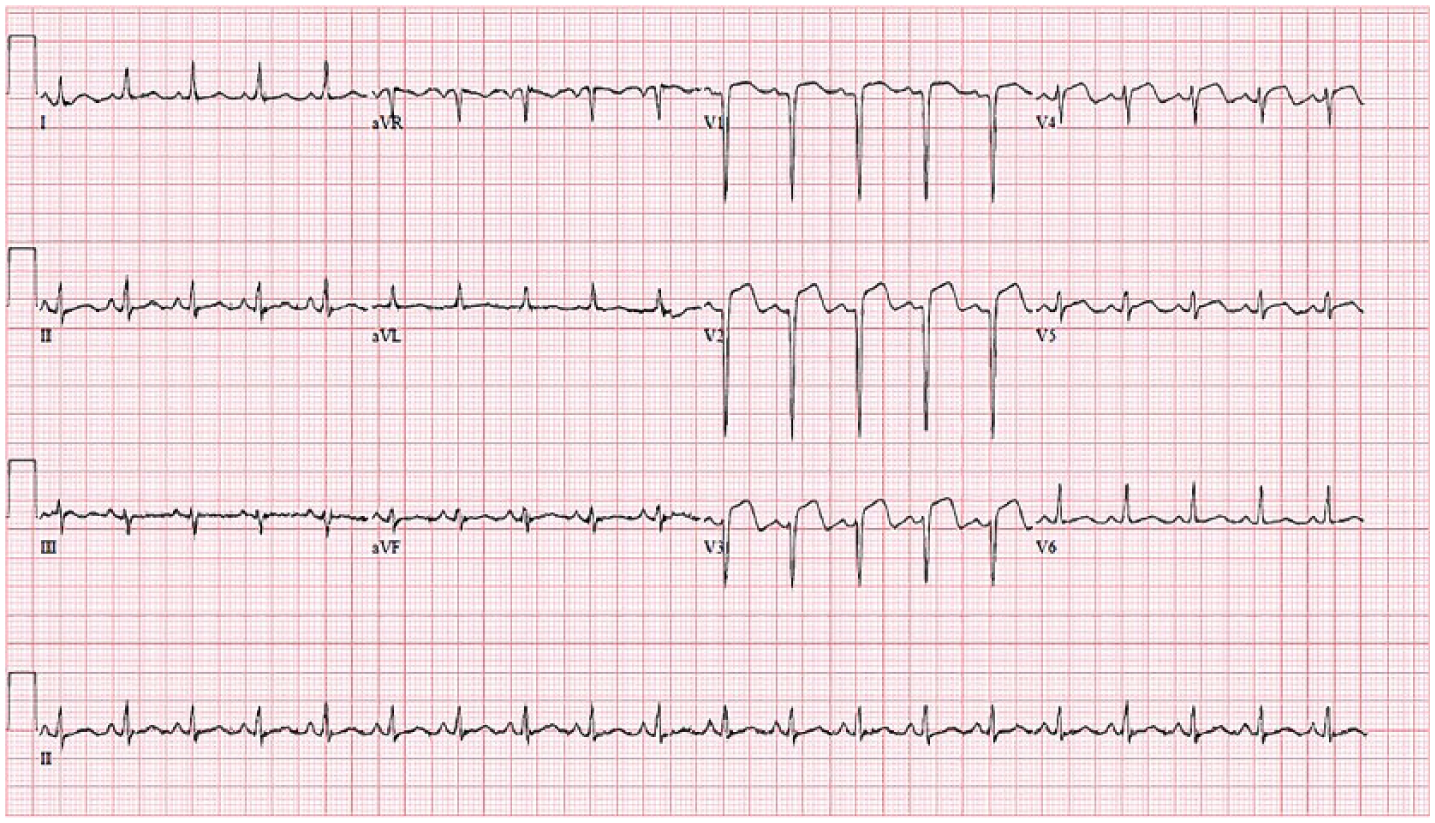
Electrocardiography showed a sinus tachycardia, V1-V3 ST elevations, and deep Q waves on V1-V2.
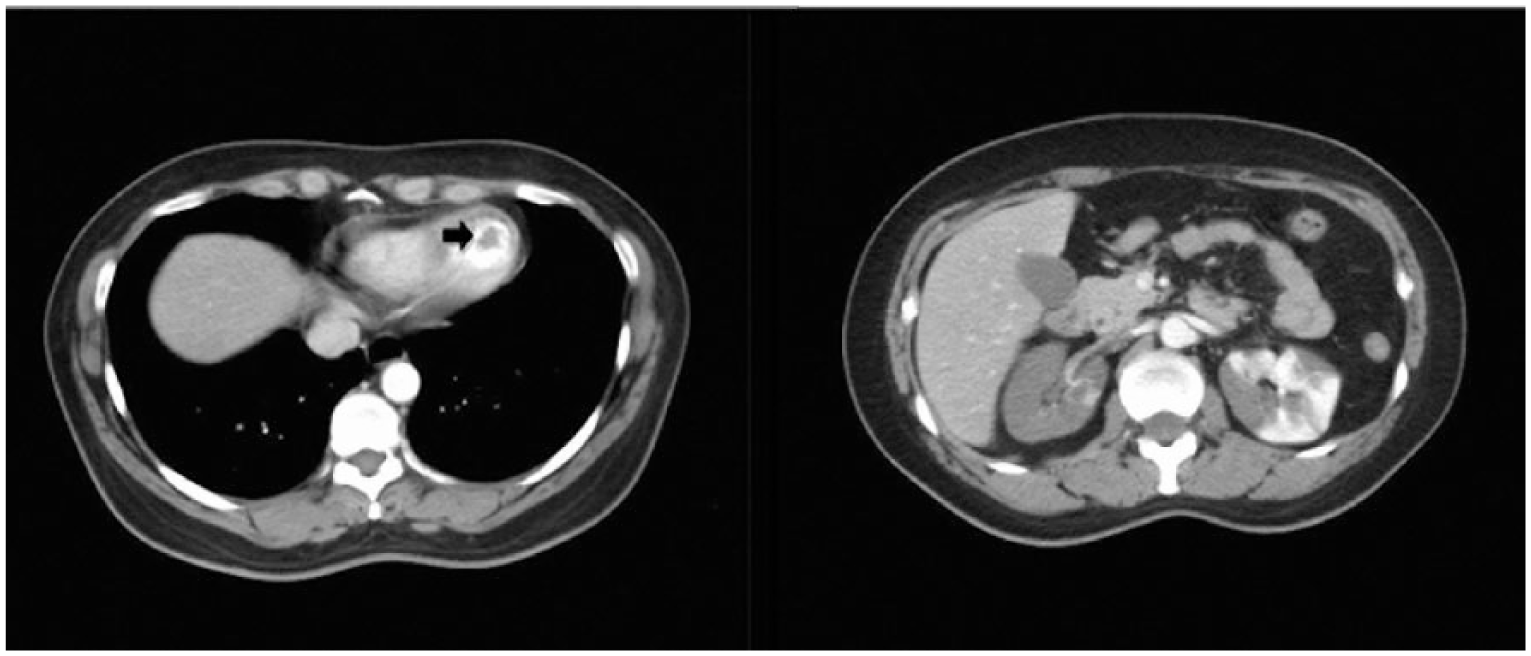
Computed tomography revealed a left ventricular thrombus (black arrow) and bilateral renal infarcts.
Further evaluations showed that the patient was negative for C3, C4, antinuclear antibody, Protein C, Protein S, fibrinogen, fibrin degradation product, anti-cardiolipin antibodies, and anti-phospholipid antibodies. The troponin-I level declined to 7.04 ng/mL, and the MB fraction remained 0% on day 2 of hospitalization. The pain in the abdomen and both legs was decreasing. Cardiac catheterization on day 4 revealed a 51% stenosis of the left anterior descending artery and a thrombus at the first diagonal branch. Dual antiplatelet therapy was continued, and the patient was shifted from intravenous heparin to oral warfarin on day 10, and was discharged on day 12. LV thrombus was totally undetectable on the follow-up echocardiography 2 months later.
Discussion
OC increase the risk of both venous and arterial thrombosis. However, arterial thromboembolic events, such as ischemic heart disease or cerebral vascular diseases, are relatively uncommon. Reports of LV thrombosis associated with OC use are even rarer.3,4 OC use in conjunction with Ergotamine was reported to result in development of two LV thrombi and right internal carotid embolic occlusion in a 35-year-old woman. The patient developed confusion, left hemiparesis, aphasia, and eventually died 2 days afterwards. 3 Another report described a 43-year-old female smoker who had taken OC for 16 years and developed LV thrombus concomitant with acute stroke and right ischemic leg. 4
Sequential relationship between MI and LV thrombosis in this patient is debatable. We believe that the patient had a recent painless MI preceding the LV thrombus formation based on the following reasons: (1) the patient did not present any acute chest pain, (2) the major etiology of LV thrombus is anterior MI accompanied by LV systolic dysfunction,5,6 (3) the LV thrombus could develop within 1–2 days after the occurrence of an anterior MI,5,6 and (4) the deep Q wave on ECG and the trend of serial cardiac biomarkers. In contrast with previous two reports, OC use seemed to be the only contributing factor of the thromboembolic events in our patient. Besides, our case is distinctive because the patient had a documented MI, which is supposed to precede LV thrombosis and other thromboembolic events.
Anticoagulant therapy is the mainstay of treatment for LV thrombosis. Both vitamin K antagonists and high-dose intravenous heparin have been shown to be effective and safe, and can reduce the risk of further embolic events.7,8 A combination of antiplatelet agent and anticoagulation therapy has also proved effective. 9 A retrospective study reported that there was no significant difference in the rate of post-treatment thromboembolism between patients who were treated with anticoagulants, surgical removal, or antiplatelet agents, although the surgical treatment group tended to have fewer post-treatment thromboembolic events. 10 There is no clear consensus on the optimal treatment strategy for LV thrombosis, as well as OC-related LV thrombosis. In our patient, conservative medical treatment resulted in complete resolution of the LV thrombus without new thromboembolic events.
Although extremely rare, young OC users may develop acute MI followed by LV thrombus formation and multiple embolisms. A combination of antiplatelet agents and anticoagulants can be an effective treatment choice in patients with OC-related LV thrombus and multiple embolisms in the absence of severe complications that need surgical interventions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.