
Abstract

Case History
A middle-aged man presented to the emergency department with acute weakness and numbness of both legs. The symptoms occurred while he bent over to fix a tire at the garage. He also complained of abdominal pain with a stinging sensation, which was radiated from his back. He denied fever, vomiting, difficulty of defecation or urination, or any recent trauma history. Upon arrival, his temperature was 36.9°C, pulse rate 74 beats per minute, respiratory rate 20 breaths per minute, and blood pressure 148/90 mmHg. He was alert and well oriented. His abdomen was soft, without tenderness or rigidity. The distal pulsation of bilateral lower limbs could not be detected. The muscle power grades of both lower limbs were zero. A computed tomography angiography (CTA) with contrast (Figure 1) and then a magnetic resonance angiography (MRA; Figure 2) were performed. The three-dimensional (3D) reconstruction of images of aorta from a spiral CTA was available (Figure 3).

A computed tomography angiography scan with contrast.

A magnetic resonance angiography.
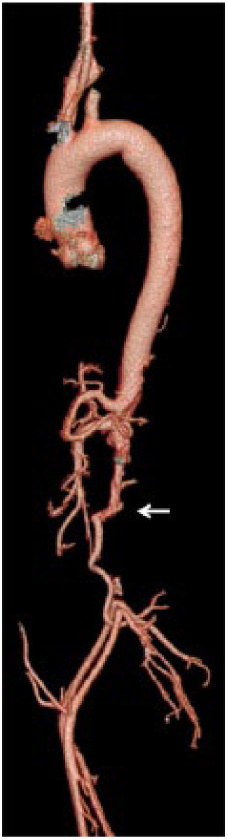
A 3D reconstruction of aorta from a spiral computed tomography angiography.
Questions
What were the CTA findings?
What were the MRA findings?
What was the diagnosis?
Answers
The CTA with contrast showed an aortoiliac thrombotic occlusion (arrow; Figure 1).
The MRA showed a symmetric hyperintensity (arrow) on T2-weighted imaging (T2WI)/diffusion-weighted imaging (DWI) in the anterior part of spinal cord at the T9–12 levels (Figure 2), compatible with a thrombosis obstructing the artery of Adamkiewicz from the extensive aortic thrombosis (arrow; Figure 3).
The diagnosis was Leriche syndrome with acute spinal cord infarction.
Discussion
Leriche syndrome results from thrombotic aortoiliac occlusion 1 and could be complicated with spinal cord infarction. The symptoms include sudden and severe back pain, followed by rapidly progressive bilateral flaccid limb weakness and sensory loss, particularly for sensations of pain and temperature. 1 The neurologic deficit of spinal cord infarction is largely defined by the involvement of vascular territory in the spinal cord.2,3 Neurologic presentations may occur painlessly, but most spinal infarcts are painful.4,5As with different levels of the spinal cord lesion involved, the symptoms may vary from mild or even reversible leg weakness to quadriplegia. 4 Early recognition of this rare disease along with timely intervention may improve outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical adherence
The study procedures were in accordance with ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.