
Abstract

Case
A 76-year-old patient with history of diabetes mellitus (DM), hypertension, and hyperlipidemia presented to the Emergency Department for fever and malaise. The patient’s spot blood glucose was 40.8 mmol/L. The preliminary blood culture result showed Gram-negative bacilli.
Questions
Answers
Anterior–posterior (AP) sitting view of CXR showed large right subphrenic gas density, suspicious for gas-forming liver abscess.
Selected axial CT image at the liver showed a large predominantly gas containing collection with multi-loculations, gas-pockets, and internal debris occupying the right lobe of liver. Right pleural effusion was also noted.
Gas-forming pyogenic liver abscess.
Klebsiella pneumoniae.
K. pneumoniae pyogenic liver abscess and bacteremia are associated with metastatic infections. Central nervous system (CNS), eyes, and lung are the most common sites involved. Diabetic patients are particularly at high risk of developing septic endophthalmitis.
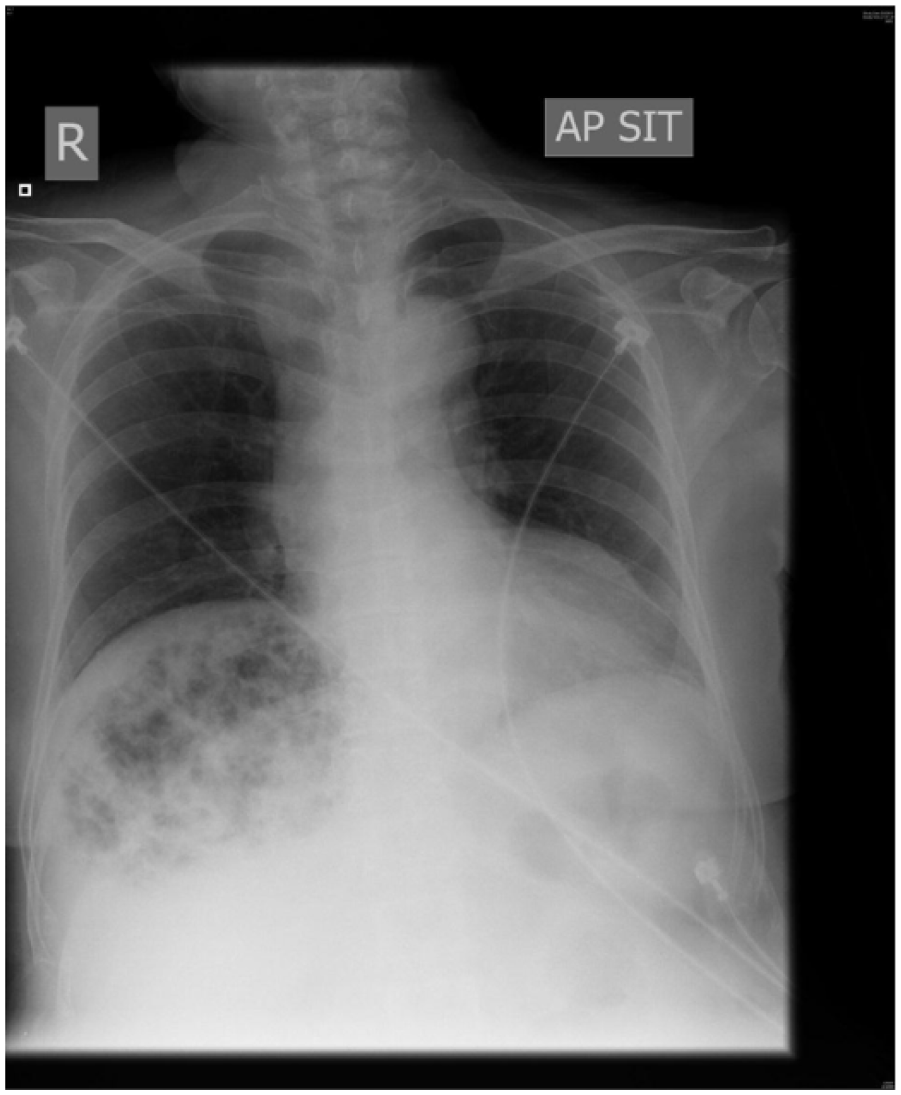
AP sitting view of CXR.

Axial CT image of upper abdomen.
Discussion
K. pneumoniae is a well-known human nosocomial pathogen and community-acquired Klebsiella infections often lead to pneumonia and urinary tract infection. In recent years, a distinct invasive syndrome due to Klebsiella infections which causes pyogenic liver abscess and bacteremic dissemination has been increasingly reported in Asia and also become an emerging disease worldwide. Currently, K. pneumoniae is the main cause of pyogenic liver abscess in Hong Kong 1 and other Asian countries including Singapore, 2 South Korea, 3 Taiwan, 4 and China. 5 In a retrospective study of patients with pyogenic liver abscess in a local tertiary hospital, K. pneumoniae accounted for 52% of the culture isolates from the blood and abscess aspirates. 1 The invasive nature of some K. pneumoniae strains is related to the presence of the capsular antigen serotypes K1 and K2. Strains expressing these capsular antigen serotypes have a high prevalence of resistance to phagocytosis, intracellular killing by neutrophils and bactericidal complements, which result in invasive infections. 6 In a retrospective study of patients with K. pneumoniae pyogenic liver abscess focusing on septic ocular or CNS complications, the K1 strains were found to be more virulent than the K2 strains to cause septic ocular (endophthalmitis) or CNS complications. 7 The mucoviscosity-associated gene A (magA) is another important virulence factor and has been described as the causative gene for K. pneumoniae liver abscess and septic metastatic complications. 6
The most common clinical presentations of K. pneumoniae pyogenic liver abscess are fever, chills, and abdominal pain, but these symptoms are non-specific. 6
Patients may develop septic shock and multiple organ failure from the overwhelming infection. CNS, eyes, and lung are the most common sites of metastatic infections which could be the initial presenting symptoms. A search for occult pyogenic liver abscess is indicated in patients with K. pneumoniae bacteremia and metastatic infections, such as meningitis, septic endophthalmitis, septic pulmonary emboli, and empyema. 8 Invasive K. pneumoniae infections predominantly occur in patients with underlying DM. Thus, patients who suffer from invasive K. pneumoniae infections must be searched for underlying DM. 9
Gas-forming pyogenic liver abscess is an uncommon condition accounting for 4–24% of pyogenic liver abscess.10,11 It carries a much higher mortality rate. The mortality rates had been reported ranging from 27.7% to 37.1%.12,13 K. pneumoniae is the most common pathogen of gas-forming pyogenic liver abscess. 12 Other pathogens reported to cause gas-forming pyogenic liver abscess include Escherichia coli, 10 Salmonella, 14 and Clostridium species. 15 Gas formation occurs as a result of mixed acid fermentation of glucose within the abscess. The high blood glucose level in patients with poor DM control provides a more favorable environment for the bacteria to form gas. 16
Diagnosis of gas-forming pyogenic liver abscess is made by radiological imaging. Radiographs, X-rays of chest or abdomen, may show pockets of gas or gas density within the liver parenchyma (as in our case), but it has been reported to be visible in only up to 36% of the cases. 16 Gas-containing liver abscess at the right lobe with fluid level may mimic free gas under diaphragm on erect CXR. 17 CT scan is more sensitive than ultrasonography in diagnosing small liver abscesses. 18 Moreover, ultrasonography is often inadequate in the evaluation of gas-forming pyogenic liver abscesses. The complex echotexture, presence of ring-down artifacts, and poorly defined margins lead to underestimation of the abscess size, difficulty in identifying loculations, and erroneous interpretation of multiplicity of abscess cavities. 19 Apart from the diagnostic purpose, radiological findings could also provide prognostic information. Globular configuration, shaggy margin, alveolar internal structure, and total gas content on CT scan are associated with poor prognosis. 13
Management of gas-forming pyogenic liver abscess includes sepsis management, strict glycemic control, antibiotic therapy, and aggressive source control by percutaneous or surgical drainage. The abscess can be percutaneously drained under both ultrasonography and computed tomographic guidance. Surgical intervention should be considered if failure to improve with percutaneous drainage and antibiotic therapy, or presence of multiple abscesses which renders percutaneous drainage technically difficult.6,9 Septic endophthalmitis is an important complication of invasive K. pneumoniae infections, and it commonly occurs in diabetic patients. The prognosis is extremely poor. Most of the patients with septic endophthalmitis result in severe visual deficit. Early diagnosis and treatment could improve the outcome.6,9 Therefore, ophthalmological assessment is warranted in all the patients with K. pneumoniae bacteremia or pyogenic liver abscess.