
Abstract
Introduction:
Prehospital tracheal intubation of a difficult airway is challenging for paramedics. Thus far, the potential role of video laryngoscopes for this purpose has not been confirmed. Therefore, this study aimed to determine the impact of different types of video laryngoscopes on the success rate and time to intubation by paramedics.
Methods:
This is a prospective, randomized, crossover manikin study involving 18 paramedics. Participants performed intubation on a difficult airway in a high-fidelity manikin using Pentax-AWS®, Glidescope®, and King Vision® (with two blade types). Time to intubation and success rate of intubation were determined. Participants also rated the best glottic view and reported their preferences of devices.
Results:
In a difficult-airway scenario, the median time to intubation with Pentax-AWS® was 22.9 s (interquartile range, 19.5–24.9 s), which was significantly shorter than using other devices. There were no significant differences in the time to maximal exposure of the vocal cords between four devices (p = 0.156). The time to insert the endotracheal tube with Pentax-AWS® and King Vision® with a guide-channel blade was significantly shorter than that with the other two devices (all, p < 0.05). Pentax-AWS® and King Vision® with a guide-channel blade showed higher success rates than the other two devices (p = 0.04). With regard to device preference, 14 participants preferred Pentax-AWS® among all devices analyzed.
Conclusion:
Pentax-AWS® could be an appropriate device for paramedics in cases of difficult airways, with high success rate.
Introduction
Prehospital endotracheal intubation of difficult airway is challenging for paramedics. According to the current guidelines, endotracheal intubation is still regarded as the optimal method for maintaining a secure airway. 1 Thus far, the survival benefit of prehospital intubation by paramedics has not been confirmed.2,3 Failure rates of up to 30% have been reported for tracheal intubation in cases where paramedics performed intubation using the Macintosh laryngoscope. 4 The Macintosh laryngoscope is regarded as the gold standard for endotracheal intubation. 5 In recent times, various types of video laryngoscopes (VL) have been developed. VLs have been shown to need a shorter intubation times and resulted in higher success rate than other laryngoscopes in clinical studies that simulated a difficult airway.6–8 Therefore, VLs could be an alternative to the Macintosh laryngoscope in in-hospital endotracheal intubations.9,10
VLs are classified according to the presence of a guide channel and curvature of the blade. VLs without a guide channel are of two types according to curvature of blade: Macintosh type and angulated blade. 11 Pentax-AWS® (Pentax corporation, Tokyo, Japan) (AWS) is a VL equipped with a blade and guide channel. The endotracheal tube is preloaded into the blade with a guide channel. The operator can insert the endotracheal tube by pushing it without additional manipulation after maximal exposure of the vocal cords. Glidescope® (Verathon, Bothell, WA, USA) (GVL) is a commercial product comprising a VL equipped with an angulated blade. With this device, the endotracheal tube should be mounted on a pre-shaped angle stylet to match the curvature of the angulated blade. King Vision® (King Systems, Noblesville, IN, USA) (KV) is a VL composed of a fixed 2.4-inch video screen, handle, and disposable blade. There are two types of blades in this device: one with a tube guide channel (KV guide) and one without a channel (KV guideless).
The type of VL used could influence the success rate and the time to intubation (TTI) by paramedics. Some studies have previously compared the direct laryngoscope and VLs in a difficult-airway situation.9,12 However, to the best of our knowledge, no studies have examined the impact of different types of VL on the success rate and TTI by paramedics in difficult-airway situations. Therefore, this study aimed to determine whether the type of VL affected the results of intubation by paramedics.
Methods
Study design
We conducted a prospective, randomized, crossover manikin study at the simulation center of Hanyang University in March 2016. The local ethics committee approved this study in January 2014 (HYI-14-004-1). We registered the study protocol with Clinicaltrials.gov before study initiation (NCT02074072).
Equipment and materials
Participants intubated the airway with AWS, GVL, KV guide, and KV guideless using an endotracheal tube with an internal diameter of 7.0 mm (Portex, St. Paul, MN, USA) and the manufacturer stylet for GVL (Figure 1). We used a high-fidelity manikin (Difficult Airway Management Simulator-Training Model, Kyoto Kagaku, Kyoto, Japan) for difficult simulated airway with cervical spine immobilizations and intermediate degree of limited mouth openings. Manikin was placed on a bed (760 mm × 2110 mm, 228 kg; Transport stretcher, Stryker Co., Kalamazoo, MI, USA).
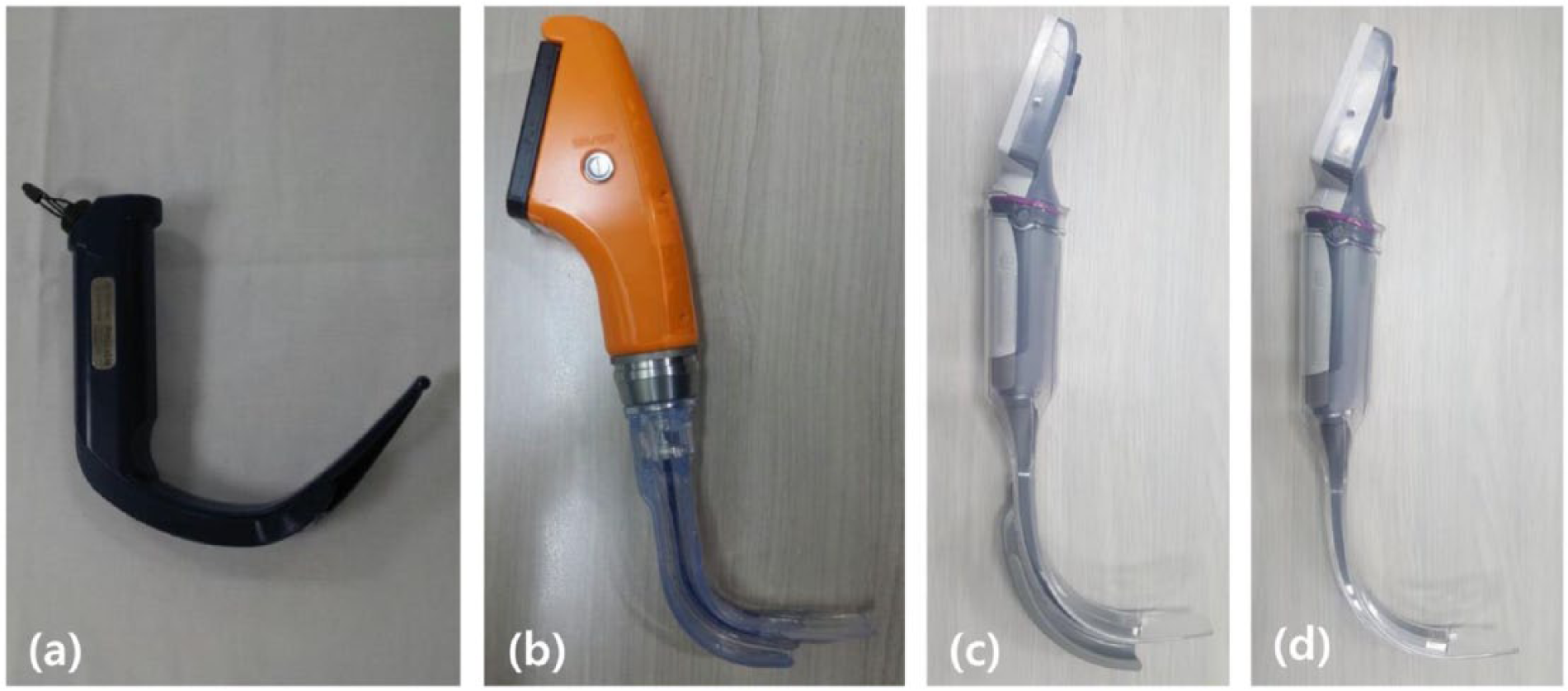
Endotracheal intubation performed using three types of video laryngoscopes: (a) Glidescope®, (b) Pentax-AWS®, (c) King Vision® with channeled, and (d) King Vision® with non-channeled blades.
Participants
We recruited 18 paramedics who participated in an airway-management workshop in March 2016. We included healthy volunteers aged between 16 and 60 years. We excluded people who had wrist and low-back disease. All participants signed a written consent form before participation. The sample size was calculated on the basis of a pilot study on the time required for intubation with AWS, GVL, KV guide, and KG guideless devices. The mean (standard deviation) (seconds) TTI was 21.29 (2.47) for AWS, 64.68 (23.01) for GVL, 40.03 (22.09) for KV guide, and 76.21 (18.01) for KV guideless. The estimated sample size was calculated using G-power 3.1.2®m (Heine Heinrich University, Düsseldorf, Germany) and revealed that a sample of 16 participants was required for this study (effect size of 1.104, a-error of 0.05, and power of 0.8); nonetheless, we enrolled 18 participants to account for a 10% drop-out rate.
Interventions
All participants completed a brief questionnaire consisting of demographic information (age, gender, body weight, and height) and prior experience of intubations using VLs in a clinical situation. Ten minutes prior to the start of the trials, participants were allowed to practice intubations with all laryngoscopes to familiarize themselves with the use of the Difficult Airway Management Simulator-Training Model in normal airway settings in neutral position. A total of 18 participants were enrolled and randomly allocated to four groups. After allocation, the participants were arranged in a random order by a computer-generated list of random numbers to minimize learning effects and were asked to perform intubation with the laryngoscopes. The intubations were performed under simulated normal and difficult-airway settings: Group A (n = 5) performed the first intubation with AWS; Group B (n = 5) performed the first intubation with GVL; Group C (n = 3) performed the first intubation with KV guide; and Group D (n = 5) performed the first intubation with KV guideless. For VLs, the manikin’s head and neck were placed in the neutral position. The height of the bed was approximately 80 cm, which was approximately the height of the participant’s mid-chest level. Participants had a 10-min break after each intubation in one simulated airway and a 30-min break before change to another airway scenario (Figure 2).
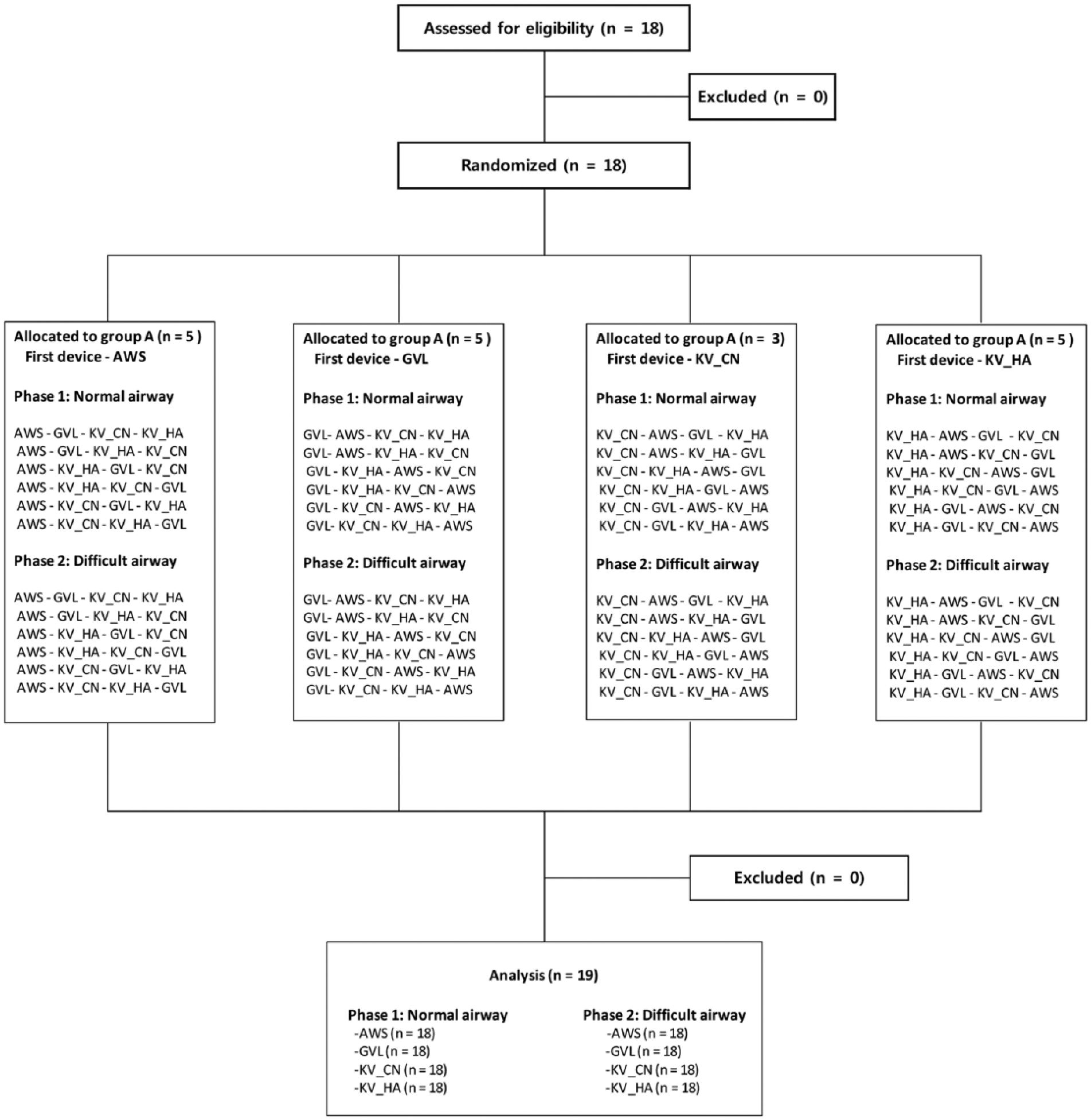
Diagram of the flow of participants through the study.
Outcomes
The primary outcome was intubation time, which was recorded from the start point to the mid-point and from the mid-point to the endpoint. The person recording the time was informed about the method to record the intubation time and was blinded to the objective of this study. The start point was taken as the time when the participant inserted the blade between the teeth after the person recording the time asked him or her to start. The mid-point was when the participant exposed the vocal cord maximally and stated “I can see.” The endpoint was at the first manual ventilation after intubation, regardless of success or failure of air inflation into the manikin’s lungs. The time to visualize the glottic view (TTV) was measured from the start point to the mid-point, and the time to progress the endotracheal tube (TTP) was consecutively measured from the mid-point to the endpoint. The TTI was calculated from the start point to the endpoint (TTV + TTP). Intubation failure was considered to occur when the tip of the tube was not properly placed in the trachea but was placed in the esophagus or the oral cavity or when the TTI was ≥90 s.13,14
Secondary outcomes were the success rate for intubation, attaining a glottic view using the percentage of glottic opening (POGO) scale, and the preference for laryngoscopes. The preference for laryngoscopes was recorded by asking the participants to choose the laryngoscope that would be most favorable in difficult-airway situations.
Statistical analysis
Data were compiled using a standard spreadsheet application (Excel, Microsoft, Redmond, WA, USA) and were analyzed using the Statistical Package for the Social Sciences (SPSS) 18.0 KO for Windows (SPSS Inc., Chicago, IL, USA). We generated the descriptive statistics and presented them as frequencies and percentages for categorical data and medians with interquartile ranges for continuous data, because the data were not normally distributed. To compare the intubation time among the four laryngoscopes and POGO scale, the Friedman test was used for continuous variables. A post hoc analysis was performed using the Wilcoxon signed rank test and a Bonferroni correction. Values of p < 0.05 were considered significant.
Results
General characteristics
A total of 18 participants were enrolled, and none of them were excluded. The general characteristics of the participants are shown in Table 1.
Demographic characteristics of the participants.
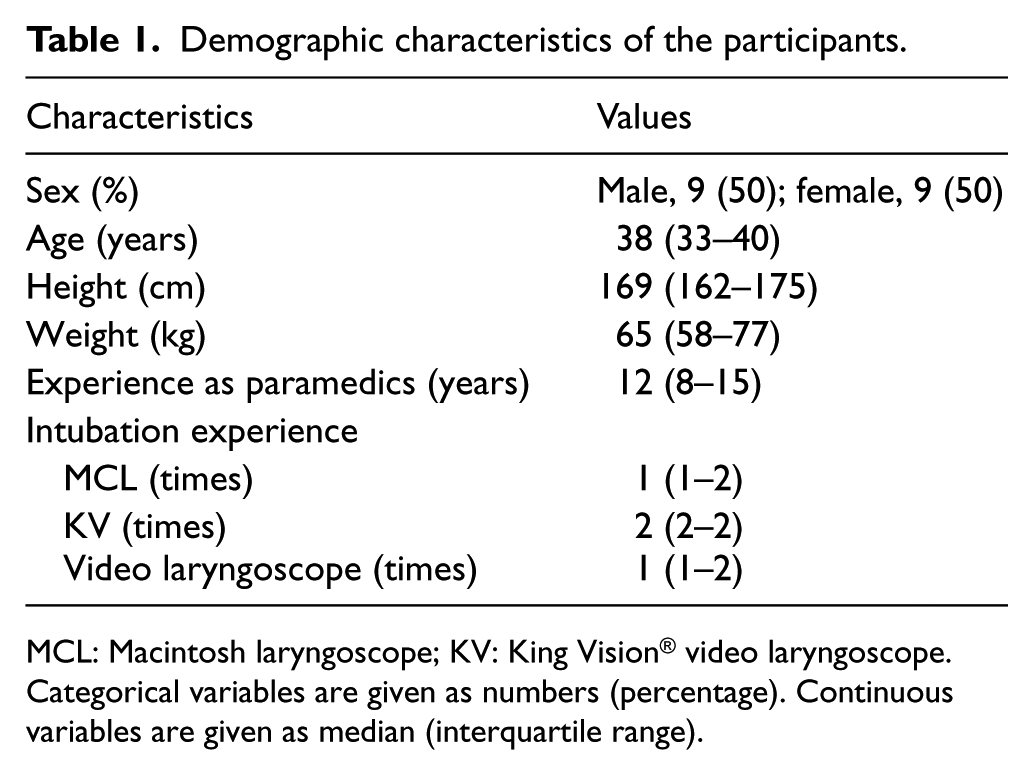
MCL: Macintosh laryngoscope; KV: King Vision® video laryngoscope.
Categorical variables are given as numbers (percentage). Continuous variables are given as median (interquartile range).
Tracheal intubation in normal airway
TTI of the KV guide was the shortest, followed by AWS, GVL, and KV guideless (p = 0.026). There were no significant differences between the AWS and KV guides (p = 0.845). There was no significant difference among the VLs except for KV guideless (all p > 0.05). In terms of TTP, progression of the endotracheal tube using VLs with a guide channel (AWS and KV guide) was shorter than that using VLs without a guide channel (KV guideless and GVL) (all p < 0.05). However, there was no significant difference between AWS and KV guide (p = 0.744) (Table 2). Intubation with AWS and KV guide showed the highest success rate, followed by GVL and KV guideless.
Tracheal intubation in a normal airway (n = 18).
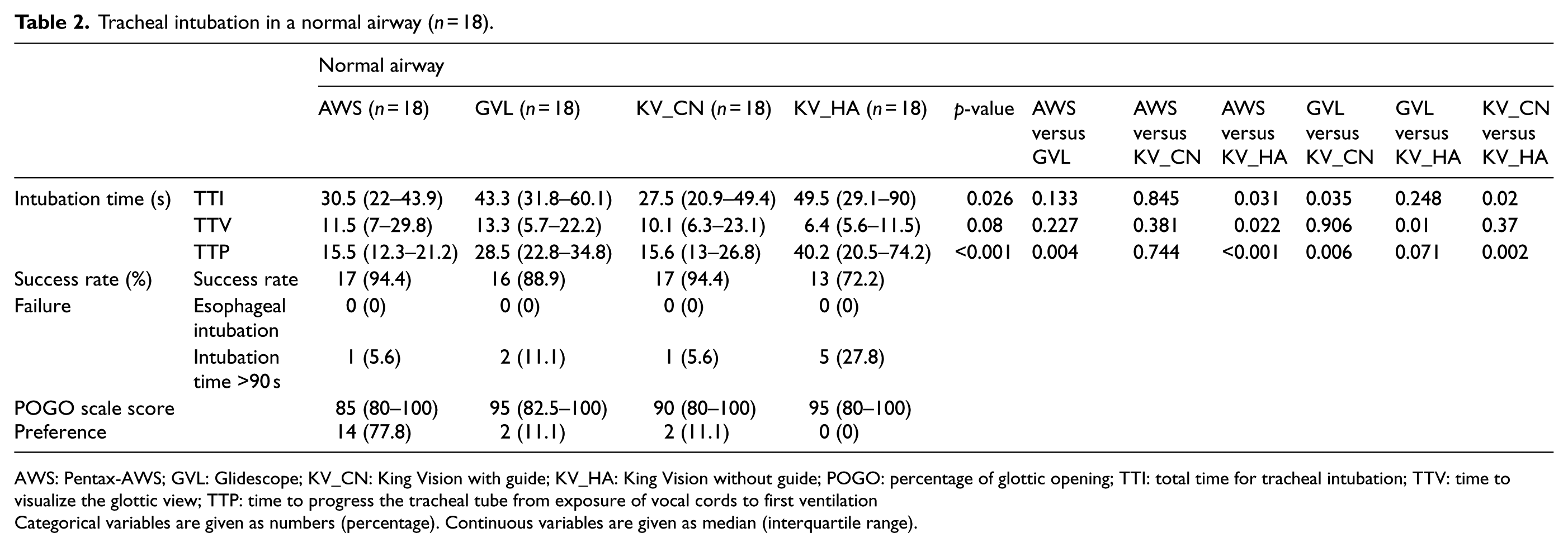
AWS: Pentax-AWS; GVL: Glidescope; KV_CN: King Vision with guide; KV_HA: King Vision without guide; POGO: percentage of glottic opening; TTI: total time for tracheal intubation; TTV: time to visualize the glottic view; TTP: time to progress the tracheal tube from exposure of vocal cords to first ventilation
Categorical variables are given as numbers (percentage). Continuous variables are given as median (interquartile range).
Tracheal intubation in a difficult airway
The TTI and TTV of the AWS were significantly shorter than those of the other VLs (all p < 0.05). However, there was no significant difference among the other VLs (all p > 0.05). TTP of the VLs with guide (AWS and KV guide) was faster than that of the VLs without guide (KV guideless and GVL) (p < 0.05), except for GVL and KV guide (p = 0.053). However, there was no significant difference between KV guideless and GVL (p = 0.102; Table 3).
Tracheal intubation in a difficult airway (n = 18).
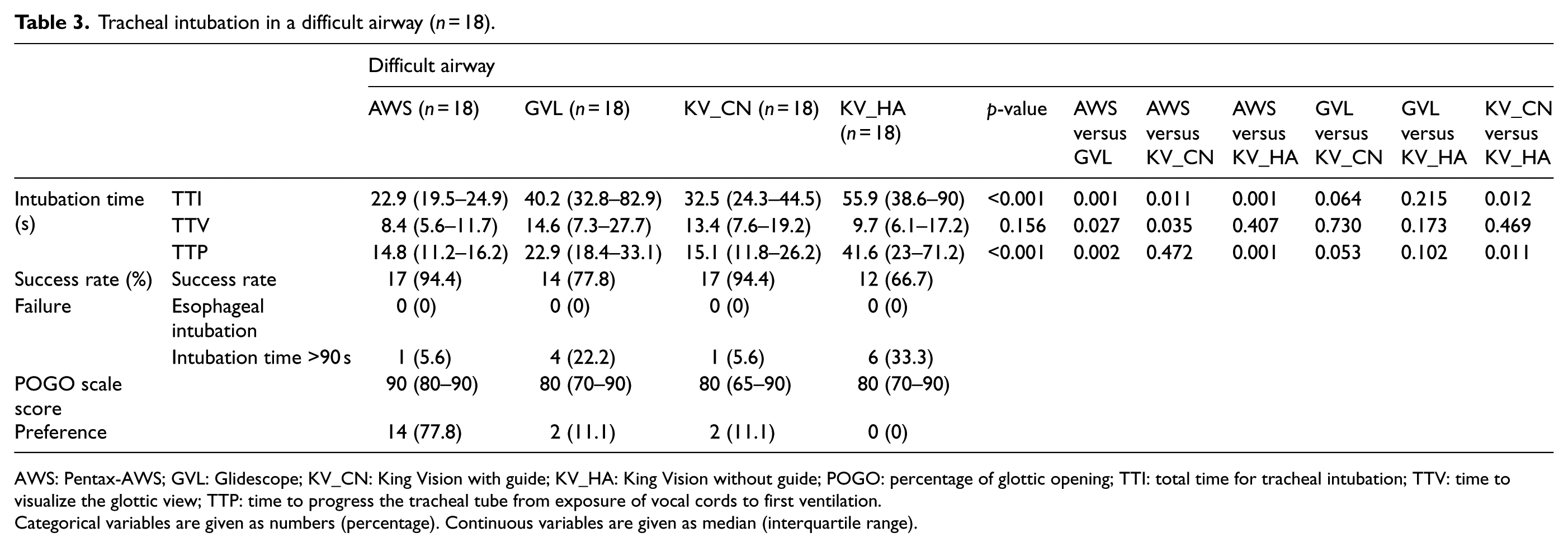
AWS: Pentax-AWS; GVL: Glidescope; KV_CN: King Vision with guide; KV_HA: King Vision without guide; POGO: percentage of glottic opening; TTI: total time for tracheal intubation; TTV: time to visualize the glottic view; TTP: time to progress the tracheal tube from exposure of vocal cords to first ventilation.
Categorical variables are given as numbers (percentage). Continuous variables are given as median (interquartile range).
Preference for laryngoscopes
A total of 14 participants (77.8%) preferred AWS, 2 participants (11.1%) preferred GVL, and the remaining participants preferred KV guide among the 4 laryngoscopes for use in difficult-airway situations.
Discussion
In this study, we demonstrated that VLs with a guide channel (AWS and KV guide) were more successful and faster than VLs without a guide (KV guideless and GVL) when used by paramedics in a manikin with a simulated difficult airway. Paramedics could expose the vocal cord well with all four types of VLs analyzed (POGO score > 80). There was no esophageal intubation in the failed cases. Among the four types, AWS was the most preferred by the participating paramedics.
A number of patient and manikin studies have evaluated the use of VLs by paramedics in difficult-airway situations.15–18 AWS and Airtraq® showed shorter TTI than the Macintosh laryngoscope in a manikin study. 8 In another study, Glidescope® Ranger and McGrath® Series 5 showed longer TTI than the Macintosh laryngoscope in a simulated difficult airway. 5 In this study, all four VLs provided acceptable visualization of the glottis, and there were no significant differences in the TTV among the four VLs. However, the TTI was shorter with AWS and KV guide than the other VLs. Furthermore, VLs with a guide channel (AWS and KV guide) showed shorter TTP than the other two VLs, and VLs without a guide channel made it difficult to insert the endotracheal tube into the trachea. In addition, paramedics could have difficulty in operating the endotracheal tube with the aid of the monitor of VLs. 12 The tip of the endotracheal should pass through an acute angle to enter the larynx and may risk coming in contact with the anterior tracheal wall. 5
The success rate of VLs with a guide channel (AWS and KV guide) was higher than that of VLs without a guide (KV guideless and GVL). There was no esophageal intubation, and the cause of failure to intubation was a TTI >90 s. Paramedics who failed to intubate found it difficult to insert the endotracheal tube, despite a good laryngeal view. 5 They were unfamiliar with operating the endotracheal tube while indirectly visualizing the airway anatomy on a video screen. 12 With the AWS device, the blade tip needs to be inserted posterior to the epiglottis (Miller-type approach), which elevates the epiglottis directly. On the other hand, the GVL is inserted anterior to the epiglottis in the vallecular fossa (Macintosh-type approach). 11 Some of the paramedics who failed to intubate had inserted the GVL using the Miller-type approach, which could make the tube insertion more difficult. The success rates for paramedics in endotracheal intubation using a VL for difficult airways are variable.5,8 The success rate within 30 s was higher with AWS and Airtraq® than with the Macintosh laryngoscope in a manikin study, 8 whereas the success rate for intubation was similar for McGrath®, GVL, and Macintosh laryngoscopes in another study. 5 The reason for this variability may be attributed to different study settings.
The participants rated AWS as the most-preferred airway device in difficult-airway situations. AWS has the target symbol on the liquid crystal display monitor, which indicates optimal alignment when centered on the glottis. In addition, the image is visible from almost all angles, and therefore, paramedics need not to be positioned close to patient’s head in a difficult scenario. Moreover, the AWS has a blade-equipped guide channel. Therefore, paramedics can insert the tube by just pulling along the guide channel. The manufacturer of the KV recommends that the Macintosh- or Miller-type approach be used and that the midline of the blade be inserted perpendicular to the nose to avoid the chest in patients (lateral blade insertion). However, the AWS did not need lateral blade insertion due to its different handle design. In addition, some paramedics complained of difficulty in inserting the blade tip by the Macintosh-type approach. These characteristics of AWS could be the reason for its preference over the other VL devices.
Despite our important findings, this study had several limitations that need to be addressed. First, difficult airways created by an advanced simulator may not be equivalent to the actual situations encountered clinically. More sophisticated and standardized simulation models representing realistic difficult airways should be used in the future. Second, we compared only four different types of VLs. Various other types of VLs have been developed and are used in clinical settings, and their utility in the management of the difficult airways should be investigated. Third, we examined only two intubation scenarios—normal airway and difficult airway—with limited mouth opening and immobilized cervical spine. The usefulness of these VLs should be determined in other situations as well, such as in airway edema, presence of blood, or copious secretions in the oropharyngeal cavity. As different experiences and level of skills among paramedics could influence the result of intubations, future studies should use a larger sample size to confirm our findings.
Conclusion
VLs with a guide channel such as AWS could be an appropriate laryngoscope for paramedics to use in cases of difficult airways, as it less time consuming and has a higher success rate than the other VLs analyzed in this study.
Footnotes
Acknowledgements
The authors thank Drs LY for their willingness to participate in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.