
Abstract
Objectives
To evaluate the clinical efficacy of reconstruction of plantar degloving injuries using a prefabricated anterolateral thigh plantar glabrous skin flap (PALT-PGSF).
Methods
Twelve patients, aged 22–56 years, with plantar degloving injuries were treated between July 2016 and December 2022. These defects are typically caused by traffic or machinery trauma. The avulsed plantar skin surfaces are intact, but revascularization are deemed unsuitable. The free tissue flaps transposed to reconstruct the defects were PALT-PGSFs. The flap size varied in width (6–13) cm and length (8–26 cm). The time from admission to reconstruction was 14–32 days (average, 23.1 days). The follow-up period ranged from 12 to 87 months (mean, 36.6 months).
Results
Eight cases were closed primarily and the other four were covered with skin grafts. All flaps survived; however, one case underwent an exploration procedure twice due to venous and arterial thrombosis. In two cases, ulcers occurred in the nonfabricated area of the flap, which was excised and replaced by PALT-PGSF area during the internal fixation removal and defatting procedure. In the other two cases, ulcers appeared on the front or outside of the feet. All the cases gained protective sensation on the weight-bearing portion of the heel. Patients can perform daily walking normally, and younger patients can even complete running and jumping exercises.
Conclusion
We advocate the use of the ALT-PGSF for the reconstruction of plantar degloving injuries.
Keywords
Introduction
The sole of the foot is characterized by a wear-resistant stratum corneum, thickened epidermis, abundant plantar fat pads, and rich cutaneous innervation, and firmadherence to the plantar aponeurosis via numerous vertical fibrous septa.1,2 These distinctive features enable the foot to absorb shock, provide stability during ambulation, and protect deep neurovascular structures during walking, running, and jumping. Plantar degloving injuries often result in complex plantar defects that significantly impair patient’s quality of life. No comparable tissue exists elsewhere in the body to achieve ideal reconstruction in terms of both aesthetics and function. Conventional reconstruction methods, such as skin grafts, 3 local pedicle flaps4,5 and free flaps,6,7 are suboptimal due to risks of recurrent ulceration, bulky appearance, 8 unstable or painful gait, and in some cases, progression to below-knee amputation. Improved functional outcomes may be achieved by using distinct plantar-degloved skin in prefabrication procedures. In order to evaluate the clinical efficacy of reconstruction of plantar degloving injuries using a PALT-PGSF, we describe here the PALT-PGSF, including surgical techniques, the advantages and limitations.
Patients and methods
Between July 2016 and December 2022, 12 patients with subfascial avulsions of the sole, accompanied by defects in the dorsal foot, were included in the study. The cohort consisted of 10 males and 2 females, with 8 patients sustatining injuries from machinery trauma and 4 from road traffic accidents. The mean age and body mass index (BMI) were 43.3 ± 11.29 years (range, 22–56) and 23.87 ± 2.10 kg/m2 (range, 18.9–27.0) respectively. In six cases (50%), the entire plantar foot was affected; two cases (16.7%) involved the hind foot; and four cases (33.3%) involved both the mid- and hind foot. Due to the severity of the crush injuries, the avulsed plantar skin was deemed unsuitable for revascularization.
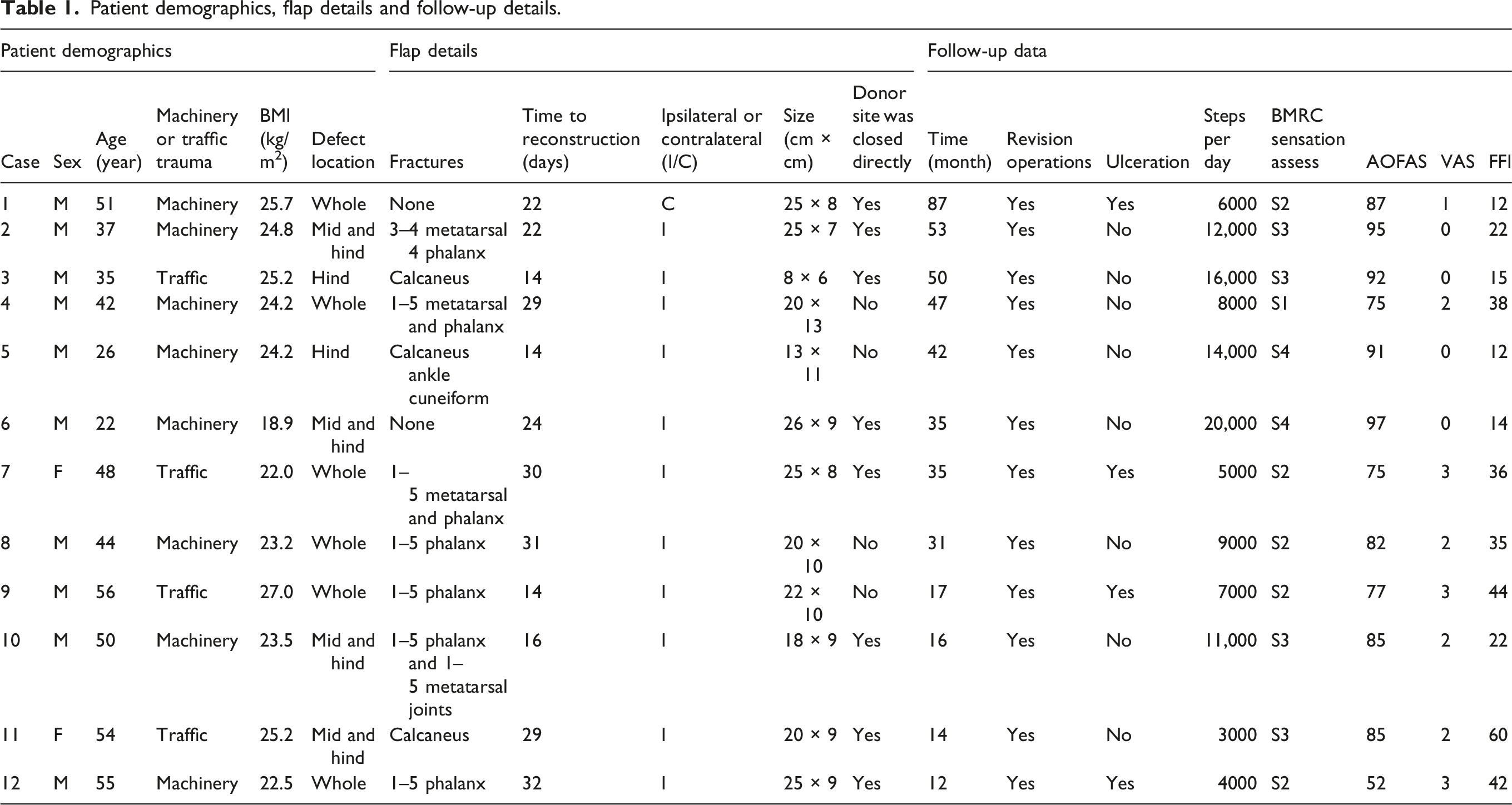
Patient demographics, flap details and follow-up details.
Emergency surgery was conducted in three stages. The first stage involved thorough debridement, tendon repair, and fracture stabilization. Full-thickness skin was then harvested from the degloved plantar skin. The second stage included designing the anterolateral thigh (ALT) flap to cover weight-bearing defects, ensuring one to three perforators were included. Prior to surgery, ultrasound scans using a wideband linear matrix array volume transducer were performed to identify the descending branch of lateral circumflex femoral and its cutaneous branches. Simultaneously, 3D images of the perforators were obtained. Based on the harvested full-thickness glabrous skin size, full-thickness skin was obtained from the ALT using a dermatome, leaving only a partial dermal layer. The full-thickness glabrous skin was grafted onto the de-dermalized ALT flap donor site. Finally, non-weight-bearing areas were covered with full-thickness glabrous skin harvested from the ALT area. The sole and other residual defects were treated with vacuum-sealing drainage (VSD). The ankle joint was maintained in a neutral position with plaster.
Dressings for the prefabricated area were changed 1-week post-surgery to assess graft survival. Negative pressure wound therapy was applied until final reconstruction. In some cases, the injured foot might require one (5 cases, 41.7%) or two (2 cases, 16.7%) additional debridement approximately 7–10 days post-injury.
A secondary reconstruction of the plantar defects was performed when no signs of infection or necrosis were present. The technique for harvesting the PALT-PGSF was identical to standard ALT flap harvesting. The prefabricated skin on the sole was transferred to its original position, with the vascular pedicle anastomosed to the posterior tibial artery and two vena comitans. It was performed with posterior tibial artery in all cases and anastomosed termino-terminal. All the lateral femoral cutaneous nerves were coapted to the calcaneal branches of the tibial nerves or the sural nerves to restore sensation. In 8 cases, the flap donor sites were directly closed, while in 4 cases, skin grafts were used.
External fixation was applied to maintain the foot and ankle in a neutral position and suspend the flap, thus preventing compression of the heel and pedicle. Postoperatively, patients received adequate doses of antibiotics, heparin, and analgesics. The affected limb was elevated and warmed using a heating lamp. Flap monitoring included color, swelling, skin temperature, elasticity, and capillary refill time. In cases of vascular insufficiency, timely exploration was performed. Once skin grafts and flaps were confirmed to be viable, patients were guided through active and passive joint and muscle rehabilitation. The external fixation device was removed approximately 1.5 months after the reconstruction.
Results
The time from admission to definitive reconstruction ranged from 14 to 32 days (23.1 ± 7.14 days). Flap widths varied from 6 to 13 cm and lengths from 8 to 26 cm. Only one flap was harvested from the contralateral ALT; the remained were obtained from the ipsilateral side. ALT donor sites could be closed primarily if the flap was less than 10 cm in width. In this series, eight donor sites were closed primarily with resulting linear scars, and four were covered with skin grafts. All flaps survived; however, one patient required two surgical explorations for venous and arterial anastomotic thrombosis. The follow-up period ranged from 12 to 87 months (36.6 ± 21.50 months).
None patients in the series were excluded because of amputation. In two patients, small ulcers developed in non-fabricated areas of the flap, which were excised and directly closed during the internal fixation removal and defatting procedure. In the other two cases, ulcers appeared on the front or lateral of the feet. The two-point discrimination of the flap was 15–30 mm (mean), and the margin of the flap and lateral femoral cutaneous nerve area obtained better two-point discrimination function and light-touch sensation than the rest of the area. Although the sensation of light touch remained unmeasurable in some areas, all patients experienced a protective sensation. Donor site complications should not be ignored. In all 12 patients, the donor area showed sensory reduction or loss, for the flap carries the nerves from the donor area. Four cases had local pigmentation, but none had motor function impairment. The time to return to walking was approximately 6 weeks for patients without fractures and 10 weeks for patients with fractures. Six months after the injury, the patient had a normal range of motion, a protective sensation over the sole, and ambulated independently. At the last follow-up, the patients could walk with regular shoes and take 3000–20,000 steps per day. A patient who could walk only 3000 steps suffered from below-knee amputation of the other leg for extensive damage in emergency surgery.
Representative case
A 22-year-old man (case 6) sustained a left plantar degloving injury accompanied by soft tissue defects on the dorsal, medial, and lateral skin of the foot during a crush injury. The middle and hind plantar skins were retrogradely avulsed (Figure 1(a) and (b)). The arteries and veins were unavailable for revascularization. The skeletons were intact. After thorough debridement, the avulsed plantar skin was harvested as full-thickness skin (Figure 1(c)) and grafted onto the dermal layer of the ALT region (Figure 1(d) and (e)). Full-thickness glabrous skin obtained from the ALT area was grafted onto dorsal, medial, and lateral defects of the foot (Figure 1(f) and (g)). The remaining wounds were covered with VSD. Twenty-four days later, plantar defects were repaired using PALT-PGSF under general anesthesia (Figure 1(h)–(j)). External fixation maintains the foot and ankle in a neutral position and suspends the flap to prevent compression of the heel and pedicle (Figure 1(k)). Both the flap and grafted plantar glabrous skin survived well after the secondary surgery (Figure 1). Plantar degloving injury accompanied with defects on the dorsal (a) and (b). The plantar skin was harvested into full thickness skin (c). The dermis layer of the ALT area (d). The prefabricated anterolateral thigh plantar glabrous skin (e). The defect on the sole of the foot (f). The full thickness skin from the thigh was grafted onto the dorsal and lateral defects of the foot (g). Pre- and post-the PALT-PGSF incision (h)–(j). External fixation maintained the foot and ankle in a neutral position and suspended the flap (k).
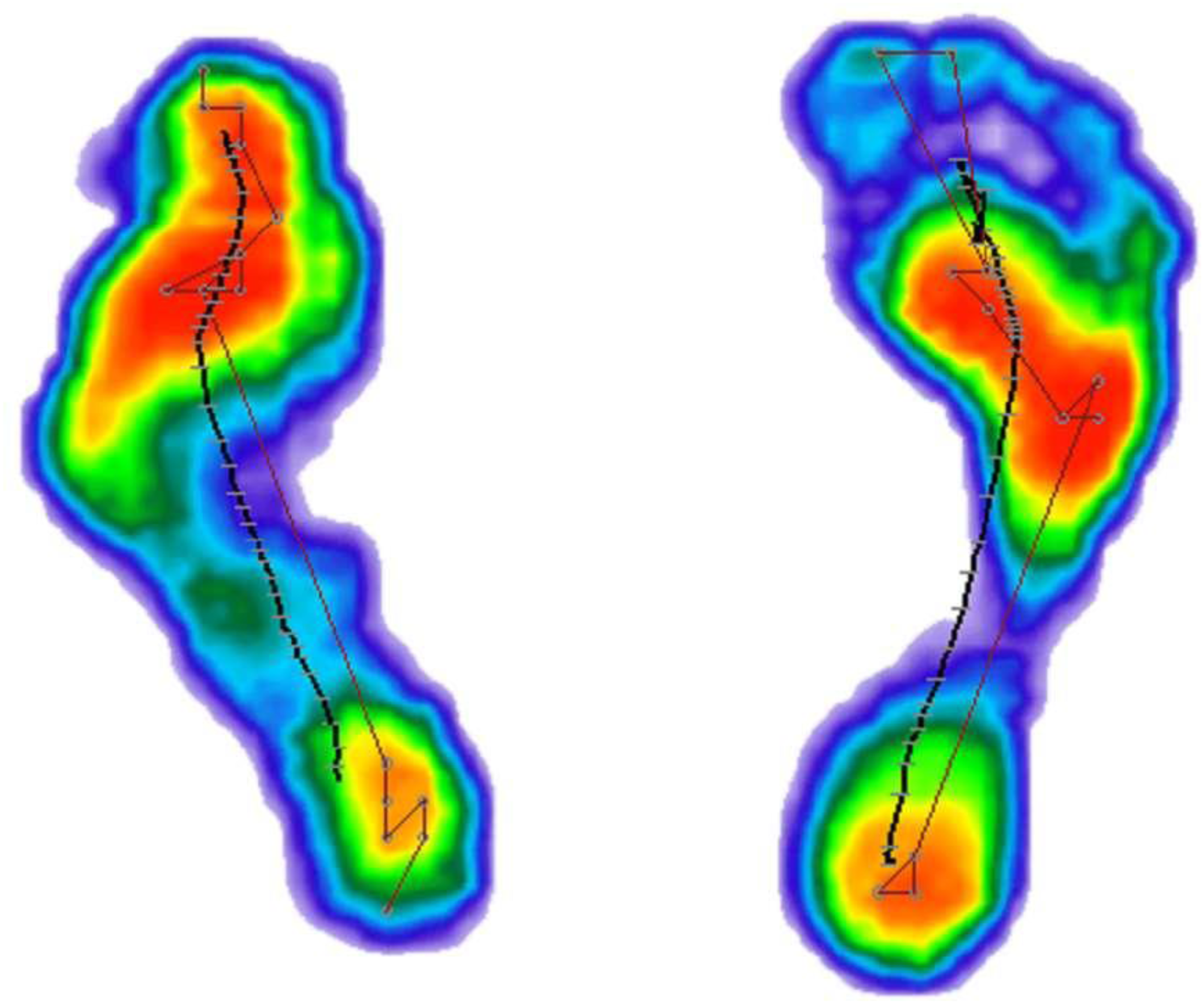
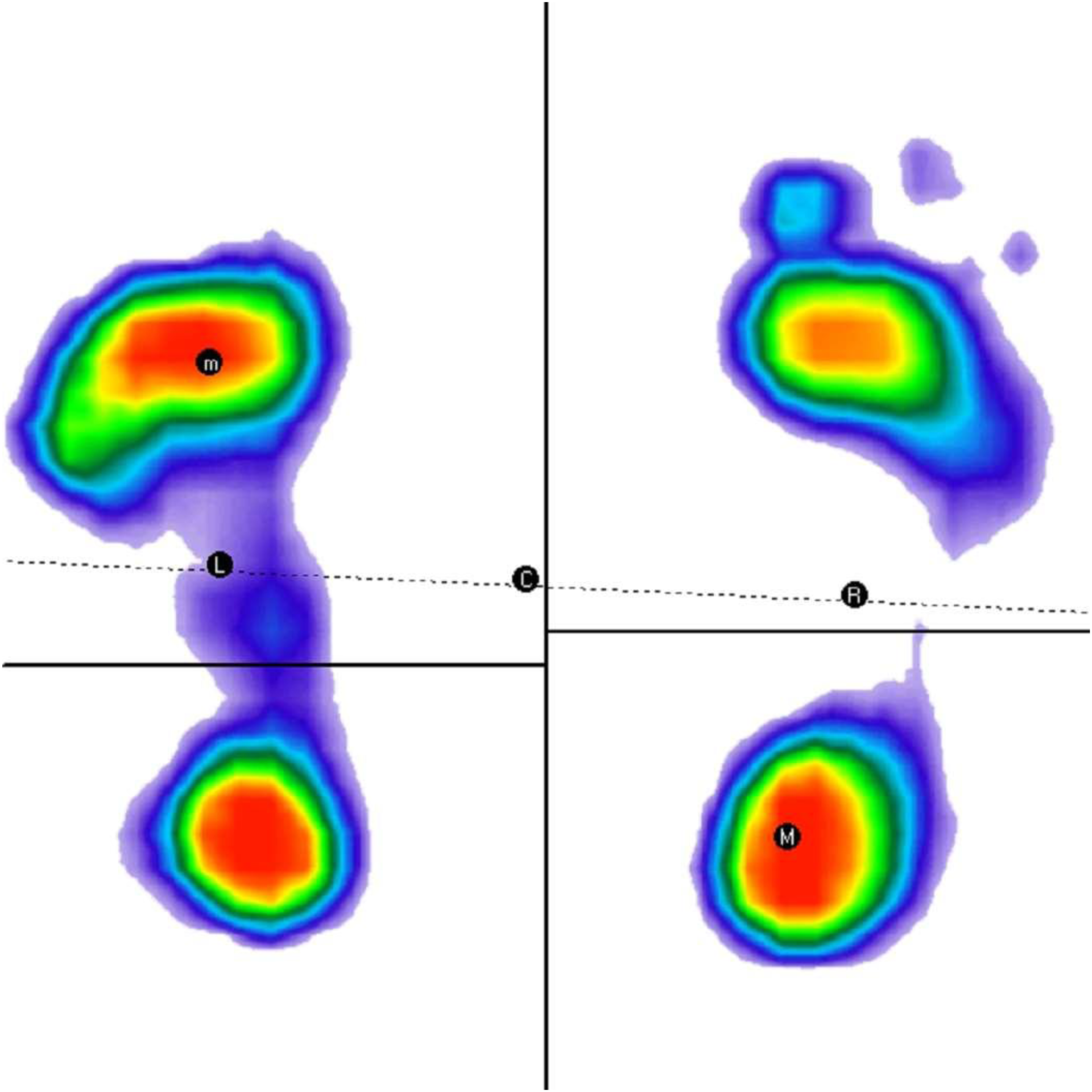
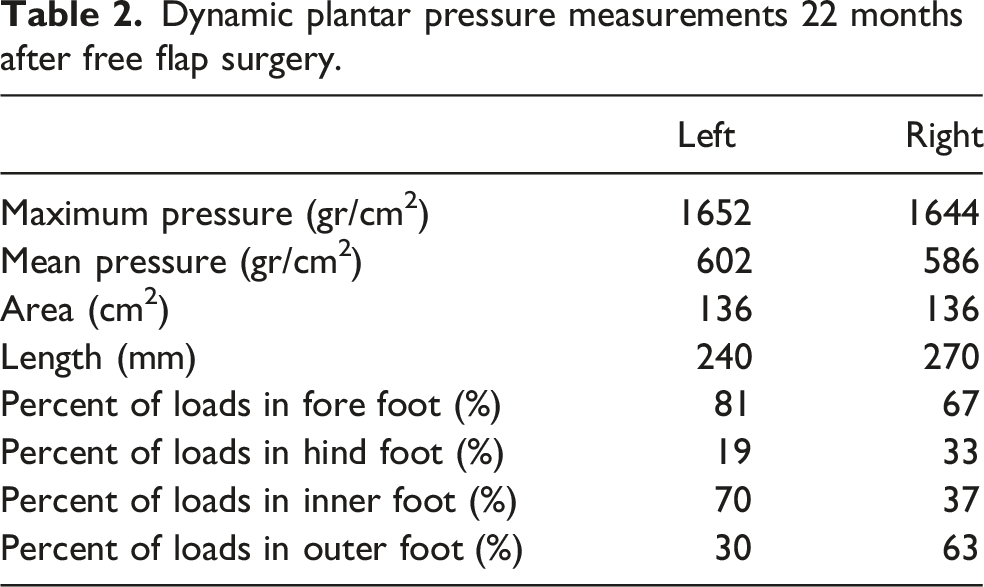
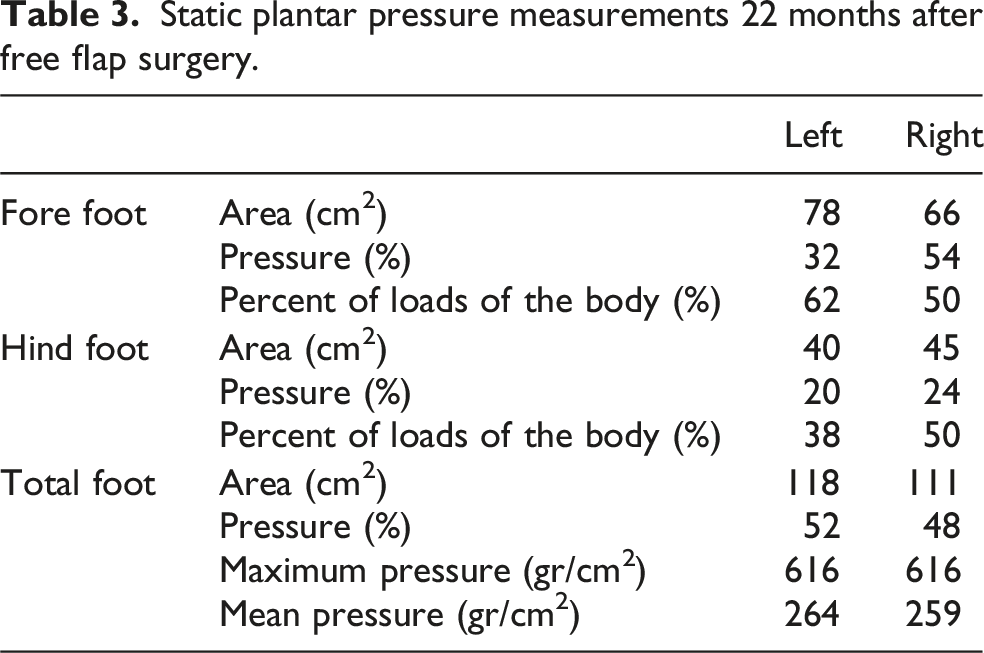
Nine months later, secondary debulking and revision procedures were performed to replace the ulcerated area with the prefabricated ALT-plantar glabrous skin. The patient’s final appearance and function were satisfactory (Figure 2(a)–(d)). 22 months later, plantar pressure distribution measurements in both feet were performed using an Easysteps Pedography Analyzer (FreeStep, Free4 40 × 40; Sensor Medica s.a.s). The subject walked over the platform at normal speed, and simultaneously, the peak pressure, maximum force, contact area, and contact time were recorded. These parameters were analyzed in three anatomical regions of interest, the hindfoot, midfoot, and forefoot, and both regions were divided into inner and outer sides. Differences in the dynamic plantar pressure distribution patterns between the feet were observed (Figures 3 and 4 and Tables 2 and 3). The final follow-up period was 35 months. The patient had a thick keratinized layer, protective sensation, durable skin, ideal outlook, good weight-bearing capacity, S3 + sensation, and no gait abnormalities. He was able to run and jump normally and walked approximately 20,000 steps daily without ulceration or pain (Figure 2). Appearance and function 22 months after free flap surgery. Warmth, good texture matches, contour, and pink color of the flap (a) and (b). Range of motion of the ankle (c) and (d). Dynamic plantar pressure distribution 22 months after free flap surgery. Static plantar pressure distribution 22 months after free flap surgery. Dynamic plantar pressure measurements 22 months after free flap surgery. Static plantar pressure measurements 22 months after free flap surgery.
Discussion
The plantar skin has the thickest stratum corneum of the body, 9 dense fibrous septa, abundant fat pads and numerous sensory nerves.1,2,4,10,11 The thickness of the unloaded heel pad is approximately 1.84 cm. 12 This distinct architecture determines the characteristics of standing up well under stress, pressure, and shearing forces during walking, jumping, and running. When full body weight is transmitted through the foot, the heel bears approximately 50-80%, with the distal sole and metatarsal heads bearing the remainder.12,13 Subfascial avulsion of the plantar skin mostly originates from the plantar fascia and usually develops into defects. Plantar skin defects can significantly hamper a patient’s quality of life. However, there are no ideal tissues for their replacement throughout the body. Therefore, the choice of the reconstruction method for weight-bearing plantar foot defects is very important. Colleagues1,4,10 recognizes that the ideal flap for the reconstruction of weight-bearing plantar skin needs to meet the characteristics of a durable thick skin with protective sensation, adequate soft tissue cushioning, and good anatomic contour.
The commonly used methods include skin grafts, local or pedicled flaps, and free flaps. However, no single method can achieve ideal repair. Skin grafts are simple, cause less trauma, have a short surgical time, and have disadvantages such as eczema, recurrent ulceration, unsightly scaring,8,14 hyperpigmentation,15,16 and painful hyperkeratosis at the junction between the skin graft and the normal plantar skin. 17 Consequently, it is impossible for these patients to walk long distances. Contralateral plantar medial skin grafts can avoid repeated ulceration and increase the wear resistance ability, but fail to absorb shock efficiently because of the lack of a proper amount of soft tissue to buffer stress. 18 It may be ideal for forefoot defects to use contralateral instep-thick skin grafts. 19
The design of the local and regional flaps of the lower leg was flexible and adjacent to the defect area. The methods included distally based sural island, posterior artery, lateral supramalleolar, and pedicled fibular flaps. They are convenient for the treatment of small proximal defects of the feet and ankles. Recurrent ulcerations and excessive keratosis are common complications. 20 They are prone to edema and venous congestion and cannot meet weight-bearing requirements. A study 21 of 36 cases showed that the durability of the distally based island superficial sural artery flap was excellent; however, this flap was inadequate. Currently, the medial plantar artery island flap has become a cornerstone in the reconstruction of foot and ankle defects because the donor site is in a relatively non-weight-bearing area and the tissue can provide durable, ulcer-free, sensate coverage of the plantar defects.20,22 A comparative study showed that the medial plantar artery flap is superior to the reversed sural artery flap because the former results in better functional outcomes and fewer postoperative complications. In addition, it allows earlier work on patients. 23 However, degloving injuries are usually too severe for the use of local or regional flaps as reconstruction options. Therefore, the contralateral medial plantar area should be considered in healthy feet. Thus, it induces bipedal injuries, prolongs the time taken to reach the ground, and increases the risk of deep vein thrombosis. Moreover, the donor site must be covered with a skin graft,13,20 and the use of a free medial plantar flap is limited by the defect. 4
Free-tissue flaps play an important role in microsurgical reconstruction. The anterolateral thigh flap, known as the universal flap, has the advantages of a large-region, shady donor site, long vascular pedicle, feeling-reconstruction ability, ease of harvest, versatility, and constant anatomy.7,24 Because of their bulky appearance, it needs to take several defatting procedures are required. Patients cannot walk with a stable gait, and chronic ulcers may occur later. 25 Moreover, they cannot provide durability and stability, which are crucial for meeting weight-bearing regional demands in the long term. 26 Latissimus dorsi flaps, another workhorse free flap for reconstruction, are selected to promote stability to some extent because of the dual tight tissue plane 27 or muscle fibrosis later.28,29 Skin-grafted muscle flaps have no subcutaneous fat, and skin grafts tend to adhere more rigidly. 27 However, ulcerations are common. Rainer C and colleagues 30 reported a 27% ulceration rate of muscle flaps and a 60% ulceration rate of free flaps for the weight-bearing region in a 44.4 months follow-up study. Karacalar 17 reported a contusion of the calcaneus treated with a combined free rectus abdominis muscle and plantar skin graft. The main advantages of this procedure are that it replaces weight-bearing skin of the heel with histologically similar skin from the instep, the fibrofatty pad of the heel with muscle, provides a good cosmetic result in the heel, and the scars at the donor site are well hidden.
Prefabrication involves the introduction of a vascular pedicle into native recipient tissue that does not harbor an appropriate pedicle 31 or the plantation of skin in an area with a pedicle. 32 The tissue was then mobilized using a new axial pedicle for reconstruction. 31 This is a modification of the pedicle flap method and has been widely used for the reconstruction of burn injuries31,32 and cosmetic defects.33–35 Erol introduced a free skin graft into a vascularized pedicle flap in an animal experiment and successfully used it clinically. 36 Wei et al. used a distally based sural artery flap or an anterolateral thigh flap as a carrier to reconstruct heel defects and achieved perfect outcomes. 37
In our study, we used an avulsed plantar degloving skin on the dermis of the ALT area using an axial ALT flap, creating a new prefabricated flap that can achieve durable sensory functions. We think this is an ideal skill for reconstruction, not only for making full use of the avulsed skin but also for obtaining good functions for plantar degloving injuries. If possible, the ipsilateral thigh was used as the prefabricated area to allow the patient to use the healthy leg and to reduce the risk of thrombus formation. Because the blood supply is abundant in the dermis layer, prefabricated skin has a rapid vessel growth and survival rate; thus, patients can exercise as soon as possible. Moreover, it reduces the incidences of dysfunction and thrombosis. The sole-to-thigh grafted skin can survive for approximately 7–10 days after the operation. In addition, the ALT area was flat; therefore, there was no need to apply pressure, thereby saving a significant amount of emergency time. During the secondary operation, we can take part in the normal anterolateral thigh skin for easy observation of blood circulation. Therefore, it is essential to include the lateral femoral cutaneous nerve in flap elevation. Anastomosis of the lateral femoral cutaneous nerve with the cutaneous nerves at the recipient site is fundamentally important in surgery because it is important to reconstruct the protective sensation in the weight-bearing area.19,30 Although the PALT-PGSF is bulky, the subcutaneous tissue acts as an absorber during ambulation. In addition, during the long-term follow-up period, contracture of the grafted heel skin on the flap resulted in a tight fit of the heel bone, which was beneficial for a stable gait. The corneum of the prefabricated skin was thick to ensure wear resistance. External fixation was used to place the ankle in the neutral position, which made it easy to prevent pressure over the heel and pedicle. It was also convenient to observe the survival conditions of PALT-P3GSFs.
Despite these advantages, this method also has several disadvantages. First, this surgical method was used only in highly selected patients. Second, a two-stage procedure is required, and there is waste of split-thickness skin in the ALT area if the dorsal or non-weight-bearing area remains intact. In patients with obesity, the flap is bulky and requires several debulking procedures.
Summary
deal reconstruction of the weight-bearing plantar heel requires durable thick skin with a protective sensation, adequate soft tissue for absorbing shock, and good anatomical contour. 38 The PALT-PGSF is a very useful way to retain more foot functions, such as durability, fewer wobble steps, color and textural matching, and protection against re-ulceration. It is useful for reconstructing plantar degloving injuries and restoring both function and aesthetics, especially for the hind or mid-hind foot.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Footnotes
Ethical considerations
Ethical approval to report these cases was obtained from the ethics committee of Wuxi Ninth People’s Hospital Affiliated to Soochow University.
Consent to participate
Informed consent was obtained from all patients or theri legal guardians included in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online. Supplemental Digital Content 1: Video (1–5) of the function of flexion-extension, gait, running, and jumping 22 months after the final follow-up.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.