
Abstract
Background
This study aims to evaluate the clinical and arthroscopic results of medial meniscus posterior tear (MMPRT) repair using an all-inside meniscal repair device combined with high tibial osteotomy (HTO), compared with HTO performed without MMPRT repair.
Methods
Overall, 38 patients who underwent open-wedge HTO using a locking plate were examined. Preoperative magnetic resonance imaging (MRI) and intraoperative arthroscopic evaluation confirmed MMPRT. During HTO, meniscal repair with an all-inside meniscal repair device was performed in 24 cases, while partial meniscectomy of the movable torn meniscus was conducted in 14 cases with MMPRT. At 2 years postoperatively, arthroscopic meniscus healing, clinical results, and radiologic results were compared.
Results
Arthroscopic evaluation showed improvement in the condition of the medial compartment cartilage after HTO in both groups. In the repair group, meniscus root healing was observed in 22 of 24 cases (92%), whereas in the no-repair group, healing was observed in 10 of 14 cases (71%); however, the difference was not statistically significant. Medial joint space increased in both groups (from 2.4 to 3.2 mm and 2.6 to 3.2 mm, respectively), and clinical scores also improved after HTO, with no significant differences between groups. Osteoarthritis progression, as assessed by K-L grade, progressed after HTO in both groups, without significant differences.
Conclusions
No significant differences were observed in arthroscopic, clinical, or radiographic results after HTO, regardless of MMPRT repair with the all-inside meniscal suture device. These findings suggest that MMPRT repair with the all-inside meniscal repair device may not be necessary during HTO.
Introduction
High tibial osteotomy (HTO) is an effective treatment option for medial osteoarthritis (OA) with varus deformity. 1 HTO could correct the mechanical axis of the lower limb, thereby shifting load-bearing to the less affected lateral compartment. 2
Medial meniscus posterior root tear (MMPRT) commonly coexists with medial OA. Since MMPRT disrupts meniscal hoop tension, patients with this condition often present with more severe knee OA.3,4 MMPRT occurs most frequently in middle-aged and elderly patients. Considering that MMPRT represents a degenerative process affecting the meniscal tissues, its intrinsic healing potential is limited.5,6
MMPRT is repairable in younger patients 6 ; however, partial meniscectomy is often recommended in older patients to relieve pain wing to the low healing potential. 7 Arthroscopic pull-out repair demonstrates superior clinical outcomes than partial meniscectomy in patients with MMPRT.8,9 Additionally, repair using an all-inside meniscal repair device yields better clinical and radiological outcomes than pull-out repair. 10 For patients with MMPRT and varus deformity, HTO without MMPRT repair could represent an effective treatment option.7,11 Furthermore, HTO combined with pull-out suture repair is an effective treatment approach.12,13 Therefore, an all-inside meniscal repair device can be applied for MMPRT repair during HTO in patients with this condition.
This study aims to evaluate the clinical, radiologic, and arthroscopic outcomes of MMPRT repair using an all-inside meniscal repair device, compared to cases without MMPRT repair during open wedge HTO.
Materials and methods
In this study, 38 patients (3 men and 35 women; mean age, 57.3 [range, 35–65] years) who underwent medial open-wedge HTO for varus deformity with medial OA were enrolled between July 2017 and October 2022. All patients underwent open-wedge HTO with locking plate fixation. MMPRT was confirmed in all 38 cases using preoperative magnetic resonance imaging (MRI) and intraoperative arthroscopy. Repair with an all-inside meniscal repair device (Fast-Fix 360, Smith & Nephew, Andover, MA) was performed in 24 cases. In 14 cases of MMPRT, only partial meniscectomy of the mobile torn meniscus was performed.
Surgical technique
All patients underwent preoperative full-length anteroposterior weight-bearing radiography of the lower limb. The correction target was the mechanical axis positioned at 62.5% of the medial-to-lateral width of the tibial plateau, measured from the medial border. Arthroscopic evaluation was performed in all patients. Repair with an all-inside meniscal repair device was performed in 29 patients. At the torn edge of the detached meniscus, the first suture of the implant was inserted, while the second suture was anchored in the root remnant and tensioned to reduce the meniscus back to the remnant (Figure 1). A proximal biplanar osteotomy was performed posterior to the tibial tuberosity after complete separation of the pes anserinus. The superficial medial collateral ligament was then elevated from the periosteum. Subsequently, the posteromedial tibial osteotomy site was opened, and fixation was achieved with a locking plate. Allogeneic cancellous bone chips (Readi-GRAFT Cancellous Chips, LifeNet Health, Virginia Beach, Virginia) were mixed with autologous bone marrow harvested from the ipsilateral anterior superior iliac spine and grafted into the osteotomy gap. The osteotomy site was covered with the superficial medial collateral ligament. Furthermore, the pes anserinus was resutured to the periosteal membrane. All patients began range-of-motion exercises on the second postoperative day while using a night splint. Partial weight-bearing was permitted from 2 weeks postoperatively, and full weight-bearing with a brace was allowed after 4 weeks. Repair using an all-inside meniscal device performed in a 62-year-old male patient. (a) Torn meniscus (arrow) was debrided using an arthroscopic shaver. (b) At the torn edge of the detached meniscus, the first suture of the implant was introduced, while the second suture was placed in the root. (c) Meniscus was repaired.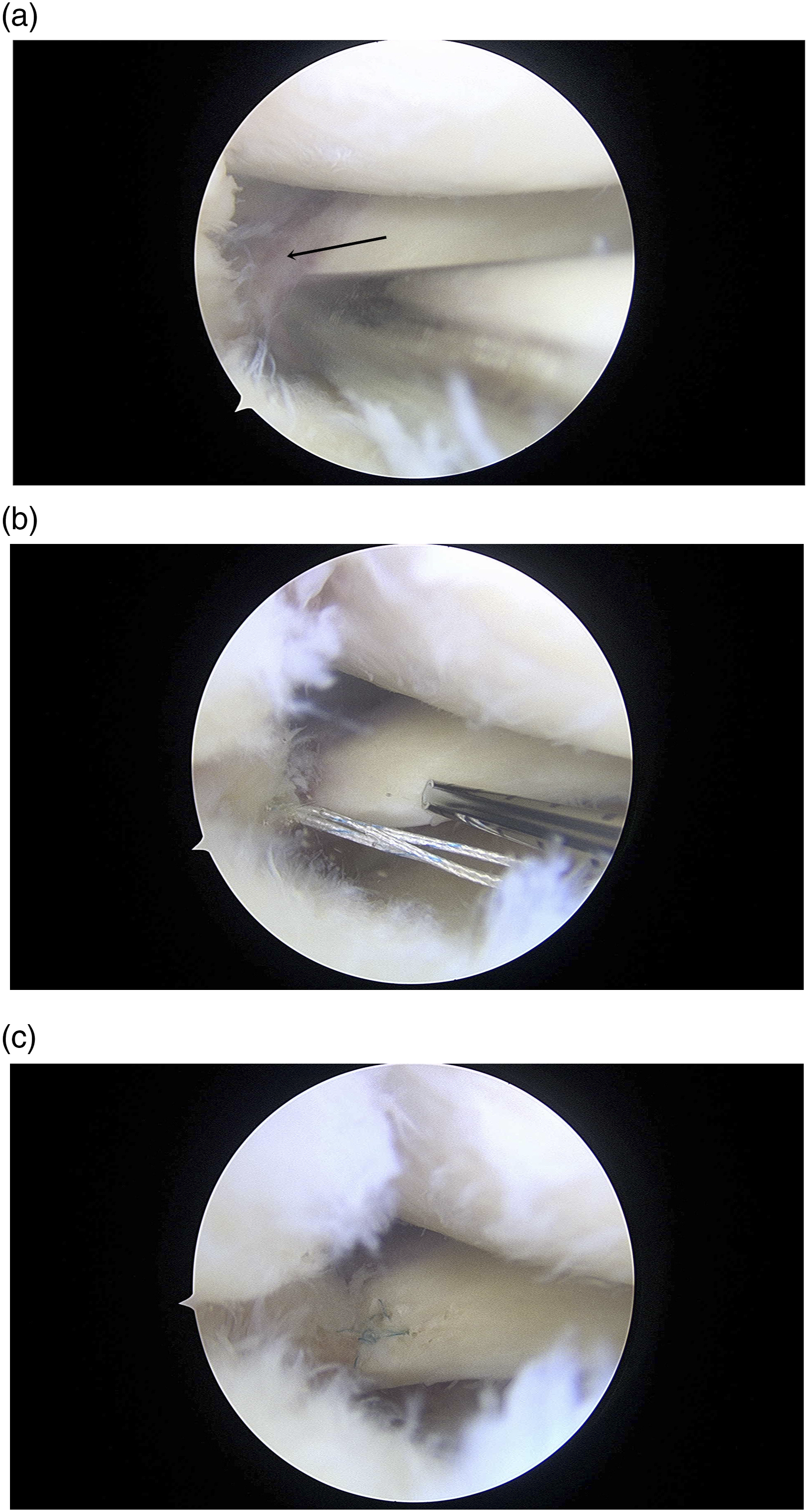
Evaluation
Patients were followed up for 24 months after surgery. Clinical outcomes were assessed using the Hospital for Special Surgery (HSS) score, Knee Society knee score (KS), function score (FS), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Radiologic evaluation included measurement of the mechanical axis, medial joint space width (from the center of the medial femoral condyle to the medial tibial plateau on the Rosenberg view), and OA grade of medial compartment using the Kellgren–Lawrence (K-L) classification. The preoperative and postoperative 24-months results were compared. Arthroscopic evaluation was performed 24 months after surgery while removing the plate, and the meniscus healing and cartilage status were evaluated.
Statistical analysis
Demographic data and clinical scores between the three groups were compared using the Chi-square test and Mann–Whitney U test. The radiological results were compared using the Mann–Whitney U-test. Preoperative and postoperative results were compared using the Wilcoxon Signed-rank test.
A p-value <0.05 indicated statistical significance. All statistical analyses were performed using SPSS Statistics version 23.0 (IBM Corp., Armonk, NY).
Results
Demographics and preoperative values.

MMPRT medial meniscus posterior root tear.
K-L grade, Kellgren–Lawrence grade.
ICRS, international cartilage repair society.
HSS, Hospital for special surgery.
KS, knee score.
FS, function score.
WOMAC, the Western Ontario and MacMaster.
Postoperative results in patients without MMPRT repair.

MMPRT, medial meniscus posterior root tear.
K-L grade, Kellgren–Lawrence grade.
ICRS, international cartilage repair society.
HSS, Hospital for special surgery.
KS, knee score.
FS, function score.
WOMAC, the Western Ontario and MacMaster.
Postoperative results in patients with MMPRT repair.

MMPRT, medial meniscus posterior root tear.
K-L grade, Kellgren–Lawrence grade.
ICRS, international cartilage repair society.
HSS, Hospital for special surgery.
KS, knee score.
FS, function score.
WOMAC, the Western Ontario and MacMaster.
Postoperative results in both groups.

K-L grade, Kellgren–Lawrence grade.
ICRS, international cartilage repair society.
HSS, Hospital for special surgery.
KS, knee score.
FS, function score.
WOMAC, the Western Ontario and MacMaster.
Discussion
In the present study, the clinical results of patients who undergo HTO with MMPRT repair using the all-inside meniscal repair device improve after 2 years. Meniscus healing is also satisfactory on arthroscopic evaluation; however, OA continues to progress. Similar results are show in patients without MMPRT repair. Furthermore, the results do not differ significantly between the two groups.
In patients with neutral alignment, MMPRT is often managed with partial meniscectomy for pain relief. 7 Previous studies show that partial meniscectomy reduces posterior fallout and mechanical symptoms.14,15 Nha et al. 16 report healing of MMPRT in patients with varus alignment after HTO without MMPRT repair. In the present study, clinical results and arthritis progression do not differ between patients with or without MMPRT repair. These findings reveal that HTO alone is an adequate treatment for patients with MMPRT.
HTO shifts the mechanical load from the medial to the lateral compartment, thereby reducing joint pressure and promoting cartilage regeneration. 17 Similarly, MMPRT has the potential to heal and remodel through the same decompression mechanism. Consistent with this concept, the present study showed that clinical scores and cartilage condition improve in patients who undergo HTO without MMPRT repair, comparable to those who undergo HTO with MMPRT repair using an all-inside repair device.
Yoon et al. 10 reported that all-inside repair improves functional outcome scores and yields better radiological results than transtibial pull-out suture repair in patients with MMPRT. In contrast, the present study identifies no significant advantage of all-inside repair during HTO in terms of clinical outcomes, arthroscopic findings, or arthritis progression. Arthritis progressed significantly in both groups, with no differences between them. In contrast, clinical scores improve significantly in all groups without differences between them. Furthermore, even when MMPRT repair is not performed, outcomes do not differ from those of patients who do not experience MMPRT. Additionally, meniscus healing appears more favorable in patients who undergo repair, although the difference is not statistically significant. Furthermore, MMPRT repair provides no significant clinical advantage. Consequently, the use of an all-inside meniscal repair device in patients with MMPRT and varus deformity is unnecessary.
The limitations of this study include the small number of patients, short-term follow-up period, and retrospective design. Additionally, the confirmation of the MMPRT site using MRI will be necessary in future studies.
Conclusion
No significant differences were observed in arthroscopic, clinical, or radiographic results after HTO, regardless of MMPRT repair with the all-inside meniscal suture device. In patients with MMPRT, repair with the all-inside meniscal device is not required during HTO.
Footnotes
Funding
This research was supported by Kyungpook National University Research Fund, 2025.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.