
Abstract
Purpose
Tibial slope influences posterior cruciate ligament tension, flexion-gap mechanics, and mid-flexion stability in cruciate-retaining total knee arthroplasty (TKA). Robotic assistance enables precise slope adjustment, yet the clinical relevance of intentional slope modification for early postoperative recovery remains unclear. This study evaluated whether tibial slope modification during mechanically aligned robotic-assisted CR-TKA affects early functional outcomes.
Methods
A retrospective cohort of 55 consecutive mechanically aligned robotic-assisted CR-TKAs performed using the VELYS™ system with ATTUNE® implants (January–July 2024) was analyzed. Patients were stratified by tibial slope change relative to baseline: Decreased (n = 42), Neutral (±0.5°; n = 5), and Increased (n = 8). Early recovery endpoints included postoperative day-1 (POD1) ambulation, POD1 pain score, length of stay, and postoperative knee range of motion. Inter-group differences were assessed using one-way ANOVA with non-parametric sensitivity testing, and linear regression evaluated slope change (Δ°) as a continuous variable.
Results
No significant differences were observed between groups in POD1 ambulation (p = 0.78), POD1 pain (p = 0.87), length of stay (p = 0.58), postoperative flexion (p = 0.69), or extension (p = 0.27). Findings were consistent on non-parametric analysis. Regression demonstrated no meaningful association between slope change and early outcomes (all p > 0.05; R2 < 0.03), with a near-flat slope–ambulation relationship (β = 0.49, p = 0.28).
Conclusion
Within a mechanically aligned robotic CR-TKA workflow, tibial slope modification was not associated with early postoperative recovery. Individualized slope adjustment may have limited impact on short-term functional outcomes. Larger prospective studies incorporating PROMs and long-term follow-up are warranted.
Keywords
Introduction
Restoring physiologic knee kinematics remains a primary objective of contemporary total knee arthroplasty (TKA). Tibial slope is a key modifiable parameter influencing posterior cruciate ligament (PCL) tension, flexion gap behavior, femoral rollback mechanics, and mid-flexion stability. Increased posterior slope has been associated with improved maximal flexion following TKA. 1 Fluoroscopic and kinematic studies have characterized patterns of femoral rollback and tibiofemoral motion in both replaced and native knees,2,3 supporting the biomechanical rationale that posterior slope may influence flexion mechanics. Conversely, excessive slope may compromise stability in PCL-deficient knees and increase posterior tibial translation. 4 Computational simulation has further demonstrated that tibial slope affects posterior condylar offset and flexion space dynamics in cruciate-retaining designs. 5
In Asian populations, native posterior tibial slope values tend to be higher than in Western cohorts. Pangaud et al. reported a +1.9° difference in global PTS in Asians versus Whites in a 3-D CT study of 378 healthy knees. 6 Such anatomical variation may influence intraoperative slope adjustment ranges and soft-tissue behaviour in cruciate-retaining TKA, highlighting the importance of validating slope-dependent recovery outcomes within an Asian arthroplasty context.
Although these biomechanical relationships are well established, the clinical impact of tibial slope variation during TKA—particularly regarding early postoperative functional recovery—remains unclear. Conventional instrumentation is limited by variability in manual guide placement, whereas robotic-assisted systems now permit sub-degree precision in component alignment and slope adjustment. 7 Robotic-arm assisted TKA has demonstrated improved early postoperative functional recovery and shorter discharge time compared with conventional jig-based TKA, 8 yet limited studies have evaluated whether intentional slope modification translates into measurable clinical benefit in pain, ambulation, or rehabilitation milestones.
Determining the influence of slope modification has implications both for biomechanical optimization and surgical workflow efficiency. Although personalized alignment concepts such as CPAK emphasise individualized restoration,9,10 if slope variation within clinically acceptable ranges does not affect short-term postoperative recovery, standardization rather than customization may simplify robotic planning and reduce intraoperative decision complexity; an important consideration in global robotic adoption.
In this context, early postoperative recovery following TKA is multifactorial and influenced by component positioning accuracy, flexion-extension gap balance, soft-tissue handling, perioperative pain control, and rehabilitation protocols. While tibial slope affects flexion-space mechanics in cruciate-retaining designs, its independent contribution to early functional recovery remains uncertain, particularly within robotically assisted workflows where alignment accuracy and gap balance are tightly controlled.
The aim of this study was to evaluate whether modifying tibial slope during robotic-assisted cruciate-retaining mechanically aligned TKA affects early recovery parameters, including POD1 pain scores, ambulation distance, hospital length of stay, and functional knee range of motion. We hypothesized that early postoperative outcomes would not differ significantly between slope-adjusted groups.
Materials and methods
Study design and population
This was a single-surgeon retrospective cohort study including 55 consecutive patients who underwent primary mechanically aligned robotic-assisted cruciate-retaining total knee arthroplasty (TKA) using the VELYS™ Robotic-Assisted Solution with ATTUNE® CR implants (DePuy Synthes, Warsaw, IN, USA) at a tertiary academic hospital between January and July 2024. All procedures were performed by a fellowship-trained senior Orthopaedic surgeon using a standardized mechanical alignment, tibia-first robotic workflow.
Surgical technique
All procedures were performed by a fellowship-trained senior Orthopaedic surgeon using a standardized tibia-first mechanical alignment workflow. A midline skin incision and medial parapatellar arthrotomy were routinely used. The anterior cruciate ligament, anterior horns of both menisci, and infrapatellar fat pad were excised for visualization, and the lateral fat pad was elevated to assist femoral registration.
Robotic navigation pins were placed intra-incisionally on the femur and extra-incisionally on the proximal tibia, with optical arrays secured to bone. Anatomical registration included the hip center of rotation, distal femoral mechanical axis, femoral condyles, tibial plateau landmarks, and bilateral malleoli. A mechanical alignment tibia-first approach was utilized, with robotic-guided tibial resection performed first and femoral preparation subsequently refined based on real-time gap-balancing feedback to achieve symmetric flexion–extension gaps.
Intraoperative planning was optimized using the PROADJUST™ interface to allow controlled adjustments within a mechanically aligned construct (Figure 1). All components were cemented, tibial stem extension was used routinely, and the patella was resurfaced in all cases. Periarticular analgesia and topical tranexamic acid were administered, and wounds were closed in layers using Vicryl® No. 1 and No. 2 for soft tissues and skin staples. Standardized postoperative care included multimodal analgesia, physiotherapy-guided mobilization from POD1, and routine sterile dressing management per institutional protocol. PROADJUST™ Surgical Planning Screen in VELYS™ showing intraoperative tailoring of tibial slope, bone resection parameters, and implant positioning to achieve balanced medial-lateral gaps in flexion and extension.
Group classification
Patients were classified according to tibial slope change measured on standardized standing lateral weight-bearing radiographs. Tibial slope was measured using CARESTREAM Vue PACS (Carestream Health, Rochester, NY, USA) following established radiographic reference-line methodology. Measurements were performed independently by two authors (JTEL and CG), with discrepancies resolved by a senior arthroplasty surgeon (TMH). Inter-rater reliability for tibial slope measurement was assessed using a two-way random-effects intraclass correlation coefficient (ICC) with absolute agreement, consistent with recommended reliability assessment for continuous radiographic measurements. Tibial slope change (Δ°) was calculated as the difference between postoperative and native preoperative slope values.
Patients were stratified into three groups based on the direction and magnitude of slope modification rather than fixed absolute values: Decreased (reduction relative to baseline; n = 42), Neutral (Δ within ±0.5°; n = 5), and Increased (greater postoperative slope than baseline; n = 8). Final values used for analysis were based on consensus measurements following adjudication.
Outcome measures
Clinical outcomes were collected from electronic medical records and physiotherapy documentation. Primary early-recovery endpoints included POD1 ambulation distance (meters, supervised physiotherapy measurement), POD1 pain score (0–10 numerical rating scale), and length of stay (LOS) in days. Postoperative knee ROM (flexion and extension) was recorded at discharge and at standard 6-months follow-up.
Statistical analysis
Continuous variables are reported as mean ± standard deviation and summarized with 95% confidence intervals where applicable. One-way ANOVA was used to compare outcome differences across slope groups, with significance defined as p < 0.05. Non-parametric Kruskal–Wallis and Mann–Whitney U testing were performed as sensitivity analyses given group-size imbalance. To evaluate slope modification as a continuous parameter, linear regression was used to assess association between tibial slope change (Δ°) and postoperative functional outcomes. Statistical analysis and data visualization were performed using R (R Foundation for Statistical Computing, Vienna, Austria).
Ethics and institutional review board determination
This study was conducted in accordance with institutional governance for retrospective analysis of de-identified clinical data and was approved by an institutional review board (ref: 2024/4046). The requirement for informed consent was waived due to the retrospective study design.
Results
Patient characteristics
Patient demographics and baseline characteristics by tibial slope modification group.

Values are presented as mean ± standard deviation unless otherwise indicated. P-values calculated using Kruskal–Wallis test for continuous variables and chi-square test for categorical variables.
Tibial slope magnitude
Magnitude of tibial slope modification following robotic-assisted CR-TKA.

Values are presented as mean ± standard deviation. Overall between-group difference in Δ slope was statistically significant (one-way ANOVA p = 1.5 × 10−9; Kruskal–Wallis p = 3.0 × 10−7).
Between-group differences in Δ slope were highly significant (ANOVA p = 1.5 × 10−9; Kruskal–Wallis p = 3.0 × 10−7), confirming that the three cohorts represented distinct slope-modification patterns rather than trivial variation. Slope adjustments were broadly distributed across the cohort rather than clustered close to zero (Figure 2), with 28 of 55 patients (50.9%) demonstrating ≥5° change and 14 of 55 (25.5%) demonstrating ≥7° change, indicating that the study evaluated clinically meaningful alignment modification. Distribution of tibial slope modification (Δ°) across the study cohort.
Early postoperative functional outcomes
Early postoperative functional outcomes by tibial slope modification group.

Values are presented as mean (95% confidence interval). P-values calculated using one-way ANOVA. Non-parametric sensitivity analysis (Kruskal–Wallis) yielded consistent results.
Given group-size imbalance and non-normal distribution, non-parametric testing was additionally performed. Kruskal–Wallis analysis demonstrated no difference in POD1 ambulation (H = 0.54, p = 0.76), and secondary comparison merging Neutral and Increased groups likewise showed no difference versus Decreased (Mann–Whitney U = 257.5, p = 0.86). Overlapping 95% CIs further support the absence of clinically meaningful differences.
Regression analysis
Linear regression analysis of tibial slope change (Δ°) and early functional outcomes.
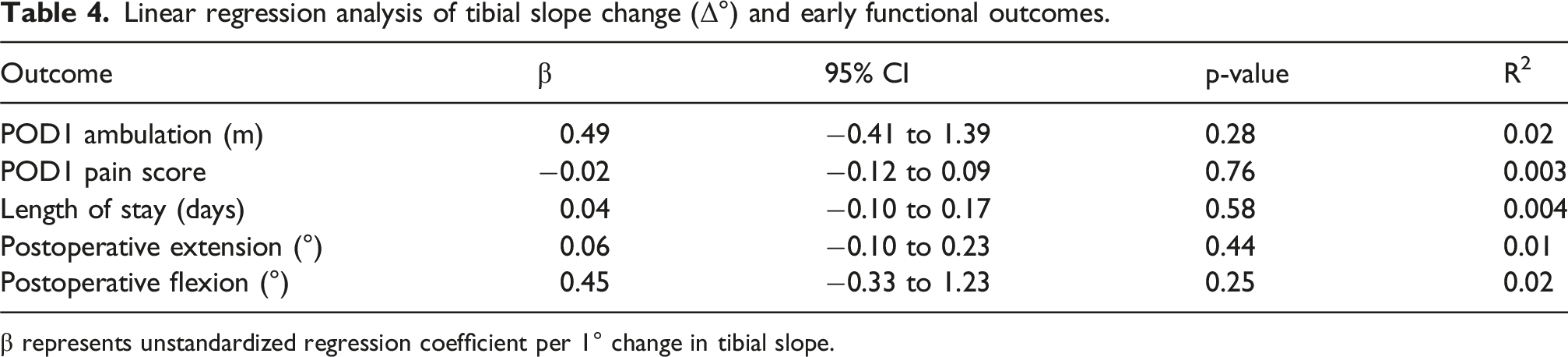
β represents unstandardized regression coefficient per 1° change in tibial slope.
The low coefficients of determination across all models indicate that tibial slope variation accounted for minimal variance in early postoperative recovery metrics, supporting the absence of a dose–response relationship between slope modification and early functional outcomes.
Discussion
Main findings
This study evaluated whether modifying tibial slope during robotic-assisted cruciate-retaining mechanically aligned TKA affects early postoperative recovery. Across 55 consecutive cases performed using the VELYS™ Robotic-Assisted Solution, no statistically significant differences were observed in POD1 ambulation, POD1 pain scores, hospital length of stay, or postoperative knee range of motion between the Decreased, Neutral, and Increased tibial slope groups. These findings suggest that tibial slope variation within the intraoperative range achieved in this cohort (−13° to +6°) was not associated with meaningful differences in early functional outcomes.
Regression analysis further confirmed the absence of a clinically meaningful continuous association between slope change (Δ°) and early postoperative metrics, with minimal explanatory value (R2 < 0.03) and a near-flat slope–ambulation trend (β = 0.49, p = 0.28). In practical terms, for every 1° change in tibial slope, POD1 ambulation increased by < 0.5 m on average—well within expected postoperative variability and with confidence intervals crossing zero, indicating no reliable directional effect.
Posterior tibial slope is biomechanically relevant in cruciate-retaining TKA, influencing flexion space tensioning, rollback mechanics, and PCL function.1,4,5 Although these principles suggest that individualized slope adjustment might theoretically optimize flexion or mid-flexion stability, the present results demonstrate that slope modification alone was not associated with measurable early clinical benefit when surgery is performed within a mechanically aligned robotic workflow. Importantly, no cases of postoperative instability or PCL-related complications were observed despite larger slope reductions, supporting the safety of slope modulation when performed within a balanced robotic workflow.
Early postoperative mobility is multifactorial and influenced by perioperative pain control, quadriceps inhibition, postoperative swelling, and rehabilitation protocols, which may limit the sensitivity of early recovery metrics to isolated biomechanical variables such as tibial slope. Although posterior tibial slope influences PCL tension and flexion-gap mechanics, its independent contribution to early functional recovery appears limited within a controlled robotic workflow, where soft-tissue balance and component positioning are tightly optimized. As such, subtle biomechanical differences introduced by slope variation may be overshadowed by these dominant perioperative factors, explaining the absence of a detectable clinical association. This finding should be interpreted cautiously given the small sample size and potential type II error.
The anatomical context is also notable. Native posterior tibial slope values tend to be higher in Asian populations compared with Western cohorts, with Pangaud et al. reporting a +1.9° difference in global slope between Asian and White participants in a 3-D CT analysis of 378 healthy knees. 6 Such variation may partially explain the broader slope distribution observed in this cohort (−13° to +6°). Despite this wider range, slope modification still demonstrated no association with early outcomes, reinforcing the limited influence of slope variation within mechanically aligned robotic CR-TKA.
These findings have important clinical implications. Robotic-assisted TKA provides highly accurate component placement 7 and improved early recovery relative to conventional jig-based techniques, 8 but if postoperative results remain comparable across slope categories, standardized slope targets rather than routine individualized customization may simplify robotic planning and reduce intraoperative decision complexity, supporting efficient global adoption. This perspective remains compatible with personalized alignment philosophies such as CPAK,9,10 but emphasizes that within mechanical alignment, slope modification functions primarily as a balancing tool rather than a means to reproduce patient-specific anatomy. Accordingly, these findings should not be generalized to kinematic alignment workflows, in which slope may be used more aggressively to recreate native biomechanics and where later functional differences may emerge.
Limitations
This study has several limitations. First, its retrospective single-centre design introduces potential selection bias. Second, a formal a priori sample size calculation was not performed due to the exploratory retrospective design, and the study may be underpowered to detect small intergroup differences. Third, subgroup distribution was uneven, particularly in the Neutral cohort (n = 5), which may limit statistical power and increase the risk of type II error, thereby reducing the ability to detect small but potentially clinically relevant differences between slope categories. Fourth, early postoperative outcome measures such as POD1 ambulation distance may be influenced by external factors including physiotherapy protocols, patient motivation, and pain tolerance, introducing variability independent of surgical parameters. Fifth, only early postoperative outcomes were evaluated, and longer-term follow-up, including detailed PROMs such as OKS, KOOS-JR, and FJS at 1–2 years, may provide additional insight into functional recovery and patient-perceived benefit. Finally, although a single-surgeon workflow enhances internal consistency, it may limit generalizability across varied surgical philosophies, implant designs, and rehabilitation environments.
Future work should include prospective studies with larger balanced cohorts, standardized PROM collection, and long-term follow-up evaluating functional recovery, mid-flexion stability, implant survivorship, and polyethylene wear. Whether slope variation influences later recovery milestones or gait characteristics remains an important area for investigation.
Conclusion
In this mechanically aligned robotic-assisted cruciate-retaining TKA cohort, no association was detected between tibial slope modification and early postoperative outcomes within the range achieved (−13° to +6°). No significant differences were observed across slope groups, and regression analysis demonstrated negligible predictive value (R2 < 0.03). These findings suggest that individualized slope adjustment appears to have limited impact on early recovery in mechanically aligned robotic CR-TKA. Further prospective studies incorporating PROMs and longer-term follow-up are warranted.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.