
Abstract
Background
Previous studies reported that medial shoulder balance (MSB) with neck tilt correlated radiologically with T1 tilt, first rib angle (FRA), and cervical axis (CA), whereas lateral shoulder balance (LSB) correlated radiologically with clavicle angle (Cla-A), coracoid height difference (CHD), clavicle-rib intersection distance (CRID), and radiographic shoulder height (RSH). Nevertheless, there is a scarcity of literature correlating both the clinical and radiological shoulder balance parameters in adolescent idiopathic scoliosis (AIS) patients. This study investigates the correlations between preoperative radiological and clinical shoulder balance (MSB and LSB) in Lenke type 1 and 2 AIS patients.
Methods
We reviewed 50 Lenke type 1 and 2 AIS patients between 2021 and 2022. Preoperative clinical shoulder parameters included front/neck base angle, front/back clavicle angle, front/back trapezium angle ratio, front/back axilla angle, trapezial area, shoulder area index 1 (SAI 1), SAI 2, and inner/outer shoulder height (SHi/SHo). Radiological shoulder parameters included T1 tilt, FRA, CA, Cla-A, CHD, CRID, and RSH.
Results
Strong correlations (r ≥ 0.6) were observed between T1 tilt, FRA, and CA (MSB with neck tilt), and between Cla-A, CHD, CRID, and RSH (LSB) (r > 0.9). T1 tilt and FRA correlated strongly (r ≥ 0.6) with front and back neck base angles, Ln [L/R trapezial area], SAI 1, SAI 2, and SHi, with the highest coefficients for front/back neck base angles (r ≥ 0.8). CA correlated strongly with front and back neck base angles, SAI 2, and SHi. Cla-A, CHD, CRID, and RSH correlated strongly with back clavicle angle.
Conclusion
MSB (T1 tilt and FRA) demonstrated very strong correlation with front and back neck base angles, and strong correlation with Ln [L/R trapezial area], SAI 1, SAI 2, and SHi. Neck tilt (CA) correlated strongly with front and back neck base angles, SAI 2, and SHi. Meanwhile, LSB (Cla-A, CHD, CRID, and RSH) correlated strongly with back clavicle angle.
Introduction
Neck and shoulder imbalance among adolescent idiopathic scoliosis (AIS) patients is a prevalent phenomenon that should be adequately addressed in corrective surgeries.1–3 The incidence of preoperative shoulder imbalance among AIS patients was reported to be 23% and 32% for Lenke 1 and Lenke 2, respectively. 4 Kuklo et al. 5 proposed a clinical shoulder grading system based on radiographic shoulder height (RSH) difference where balanced was defined as <1 cm, minimal imbalance as 1–2 cm, moderate imbalance as 2–3 cm, and significant imbalance as >3 cm. Subsequently, Qiu et al. 6 identified a discrepancy between radiological and clinical shoulder balance and suggested that shoulder balance should be further subdivided into inner and outer shoulder height. Building on this concept, Ono et al. 7 described clinical shoulder as two distinct entities: medial shoulder balance (MSB) and lateral shoulder balance (LSB). MSB was reflected by the trapezial angle as well as Ln [L/R trapezial angle], and correlated well with radiological parameters, i.e., T1 tilt, first rib angle (FRA), and upper thoracic curve size. In contrast, these radiological parameters correlated weakly with LSB, as represented by the clinical clavicle angle. 7 Kwan et al. 8 further reported that clinical shoulder grading correlated with coracoid height difference (CHD), RSH, clavicle-rib intersection distance (CRID), and clavicle angle (Cla-A), parameters that may predominantly reflect LSB. Additionally, the authors introduced a clinical neck tilt classification based on trapezius muscle height difference, ranging from Grade 0 (no neck tilt) to Grade 3 (uncorrectable neck tilt with trapezius muscle height difference of >1 cm), and concluded that neck tilt with MSB correlated with cervical axis (CA) and T1 tilt. 8 Deng et al. 1 later emphasized that MSB and LSB represent two disparate features of shoulder balance. Among Lenke 2 AIS patients who achieved LSB (RSH <10 mm) postoperatively, 69.2% of them experienced medial shoulder imbalance (MSI) (T1 tilt <−3° or >3°). 1
With regards to the relationship between clinical and radiological shoulder balance, Qiu et al. 6 reported that none of the radiological parameters could precisely reflect the clinical shoulder appearance (none had correlation efficient, r > 0.8). In contrast, Matamalas et al. 9 identified statistically significant correlations between clinical and radiological shoulder parameters, although they ranged from poor to moderate (r < 0.6). Taken together, these findings illustrate the ongoing inconsistency in the literature concerning the strength of clinical and radiological correlation in the shoulder balance assessment. In this study, we hypothesized MSB with neck tilt as represented radiologically by T1 tilt, FRA, and CA, may correspond to specific clinical parameters. Meanwhile, LSB as represented radiologically by Cla-A, CHD, CRID, and RSH, could correspond to another specific clinical shoulder parameters. Hence, this study was designed to investigate the correlations between preoperative radiological and clinical shoulder parameters for MSB with neck tilt and LSB, among Lenke type 1 and 2 AIS patients.
Materials and methods
This retrospective study was conducted in a single institution with institutional review board approval (MREC ID No.: 202214-10890). Sample size calculation was performed using G* Power (version 3.1.9.6; Heinrich Heine University), based on the correlation coefficient reported by Ono et al.
7
(for trapezial angle and T1 tilt). Using an alpha of 0.05 and a power of 0.95, a minimum of 15 patients was required. A total of 73 AIS patients with Lenke type 1 or 2 curve, who underwent posterior spinal fusion (PSF) surgery between November 2021 and April 2022 were consecutively recruited. 23 patients who had poor quality radiographs or clinical photographs were excluded (Figure 1). All 50 patients recruited in this study had complete preoperative clinical photographs and radiographs. Preoperative clinical and radiological shoulder parameters were measured. CONSORT flow diagram illustrating the patient selection.
Clinical parameters
All patients were given detailed explanations and instructions on positioning, with written consent obtained prior. During clinical photography session, male patients were required to remove all upper-body clothing, whereas female patients were provided a white singlet to conceal the front of their bodies to preserve privacy. Patients were instructed to stand in an upright neutral position, defined as a comfortable natural standing posture, with both upper limbs relaxed by the sides and the head facing the camera. Clinical photographs were obtained against a grid background, which served as a reference to facilitate visual assessment of symmetry and alignment. The hips and knees were fully extended, with the feet positioned plantigrade and equidistant from the midline at approximately shoulder width.
A tripod-mounted camera was placed directly in front of the patient at shoulder level, aligned parallel to the floor, and placed at a standardised distance of one metre from the patient’s footwear. Standardised photographs were obtained sequentially in both front and back views under identical condition during quiet standing, without breath-holding instructions. To minimise posture-related variability, patients were instructed to remain relaxed and avoid voluntary shoulder elevation or neck tilting, and maintain a forward-facing head position during image acquisition.
Definitions of clinical parameters applied were mentioned in previous studies6,7,9,10 (Figure 2). Positive values indicated left-side elevation. The metric for height difference was in millimetres whereas angles were measured in degrees. (1) Front neck base angle: the angle between a horizontal reference line and the line connecting the intersections of the sternocleidomastoid muscle and trapezius muscle profiles. This was known as trapezial angle by Ono et al.
7
(2) Back neck base angle
10
: the angle between a horizontal reference line and the line connecting the base of the neck. (3) Front clavicle angle
7
: the angle between a horizontal reference line and the line connecting the upper margin of both acromial processes. (4) Back clavicle angle: the angle between a horizontal reference line and the line through two inflection points of the shoulders and upper arms. This was known as the shoulder angle by Qiu et al.
6
(5) Front/back trapezium angle
9
: the angle between a horizontal reference line and the line following the external border of the trapezium muscle. The left/right trapezium angle ratio was calculated. (6) Front/back axilla angle6,9: the angle between a horizontal reference line and the line through both axillae. (7) Trapezial area
7
: area enclosed by the following borders: (a) the line connecting the top margin of the acromial processes (b) the perpendicular line to it through the intersection of the sternocleidomastoid muscle and the trapezius muscle (c) the superior margin of the trapezius muscle. (Measurement from the front view.) (For normalization purposes, the natural log of the ratio of left to right trapezial area (Ln[L/R trapezial area]) was used.) (8) Shoulder area index 1 (SAI 1)
6
: a horizontal line (l
1
) was drawn through the higher axilla, followed by the plumb line through the midpoint of neck to divide between two sides. Line m was the line connecting the inflection points between shoulder and neck. Two areas were marked, both surrounded by the superior margin of the shoulders, the outer margin of the upper arms, l
1
, plumb line, and line m. Left area was identified as A1 and right was A2. The ratio A1/A2 was defined as SAI 1. (9) Shoulder area index 2 (SAI 2)
6
: A horizontal line was drawn through the lower inflection points between the shoulder and the upper arm (l
2
) followed by the plumb line through the midpoint of neck to divide between two sides. Two areas were marked, both surrounded by the superior margin of the shoulders, l
2
, plumb line, and line m. Left area was identified as B1 while right was B2. The ratio B1/B2 was defined as SAI 2. (10) Shoulder height (SH)
6
: A horizontal line through the higher axilla intersects the arms at P (left) and Q (right) was drawn, followed by the plumb line through the midpoint of neck intersecting the horizontal line (O). Two trisection lines were drawn from the horizontal line at equal space from the plumb line at both right and left sides, intersecting the shoulders at A, B (left) and A’, B’ (right). (a) Inner shoulder height (SHi): the height difference between the inner horizontal lines (A and A’). (b) Outer shoulder height (SHo): the height difference between the outer horizontal lines (B and B’). Photographs demonstrated all clinical parameters measured preoperatively.

Radiological parameters
All AIS patients had routine whole spine erect anteroposterior and lateral radiographs performed as part of the preoperative assessment. Similarly, radiographs were obtained with patients in an upright neutral standing posture, with both upper limbs relaxed by the sides, hips and knees fully extended, and the feet positioned plantigrade and equidistant from the midline at approximately shoulder width. Patients were instructed to face the imaging apparatus with a forward-facing neutral head position, without breath-holding, and to remain relaxed while avoiding voluntary shoulder elevation or neck tilting during radiographic acquisition. Radiological measurements were performed using Centricity™ Universal Viewer Zero Footprint, version 6.0 SP11.2.2, GE Healthcare. Preoperative proximal thoracic (PT) Cobb angle, main thoracic (MT) Cobb angle, lumbar (L) Cobb angle, and radiological shoulder parameters were measured from the available radiographs.
Preoperative radiological shoulder parameters measured are defined below.5,7,11 Positive values signified inclination to the right side of the reference line (left side elevated) and contrariwise for negative values. (1) T1 tilt: The angle between a horizontal reference line and the line parallel to the upper endplate of T1 vertebra (degree). (2) First rib angle (FRA): The angle between a horizontal reference line and the line connecting both superior borders of the first ribs (degree). (3) Clavicle angle (Cla-A): The angle between a horizontal reference line and the line connecting the most cephalad portion of both right and left clavicles (degree). (4) Cervical axis (CA): The angle between a vertical reference line and the longitudinal axis of cervical spine (bisecting the centre of C2 odontoid process and C7) (degree). (5) Coracoid height difference (CHD): A horizontal line was traced at the superior border of both right and left coracoid processes. The height difference was identified between the right and left lines measured (millimetres). (6) Clavicle-rib intersection distance (CRID): The height difference between the horizontal lines at the level of intersection between the clavicle and the outer border of second rib (millimetres). (7) Radiographic shoulder height (RSH): the difference between the horizontal lines at the level of soft tissue shadow superior to the acromioclavicular joint (millimetres).
Statistical analysis
Data analysis was conducted using SPSS Version 26.0 (SPSS Statistics for Windows, IBM Corp., Armonk, New York, USA). Continuous variables were assessed for normality using the Shapiro-Wilk test and by visual inspection of histograms. Continuous data are presented as mean and standard deviation for parametric data and as median and interquartile range (IQR) for non-parametric data. Categorical data are presented as frequency and percentage. Comparison between Lenke subgroups were performed using the independent t-test for parametric continuous data, Mann-Whitney U test for non-parametric continuous data, and Fisher’s exact test for categorical variables. Pearson correlation analysis was used for normally distributed continuous variables while Spearman correlation analysis was applied for non-normally distributed continuous variables, to assess the relationships between preoperative clinical and radiological shoulder balance parameters. In this study, we regarded r, <0.20 as very weak, 0.20 – 0.39 as weak, 0.40 – 0.59 as moderate, 0.60 – 0.79 as strong, and 0.80 – 1 as very strong correlation.9,12 P value <0.05 was the cut-off value for statistical significance.
Results
Demographic data for 50 Lenke type 1 and 2 AIS patients.

Parametric variables are presented as median ± standard deviation, while non-parametric variables are reported as median [interquartile range].
Height and weight are recorded to the nearest whole unit to minimise false precision.
Comparison of clinical and radiological shoulder balance parameters between Lenke type 1 and 2 AIS patients.

FRA: First rib angle; Cla-A: Clavicle angle; CA: Cervical axis; CHD: Coracoid height difference; CRID: Clavicle-rib intersection distance; RSH: Radiographic shoulder height; Ln[L/R trapezial area]: natural log of the ratio of left to right trapezial area; SAI 1: Shoulder area index 1; SAI 2: Shoulder area index 2; SHi: Inner shoulder height; SHo: Outer shoulder height.
Parametric variables are presented as median ± standard deviation, while non-parametric variables are reported as median [interquartile range].
Cobb angles are recorded to the nearest whole unit to minimise false precision.
aStatistically significant.
Pearson correlation analysis for radiological shoulder balance parameters.
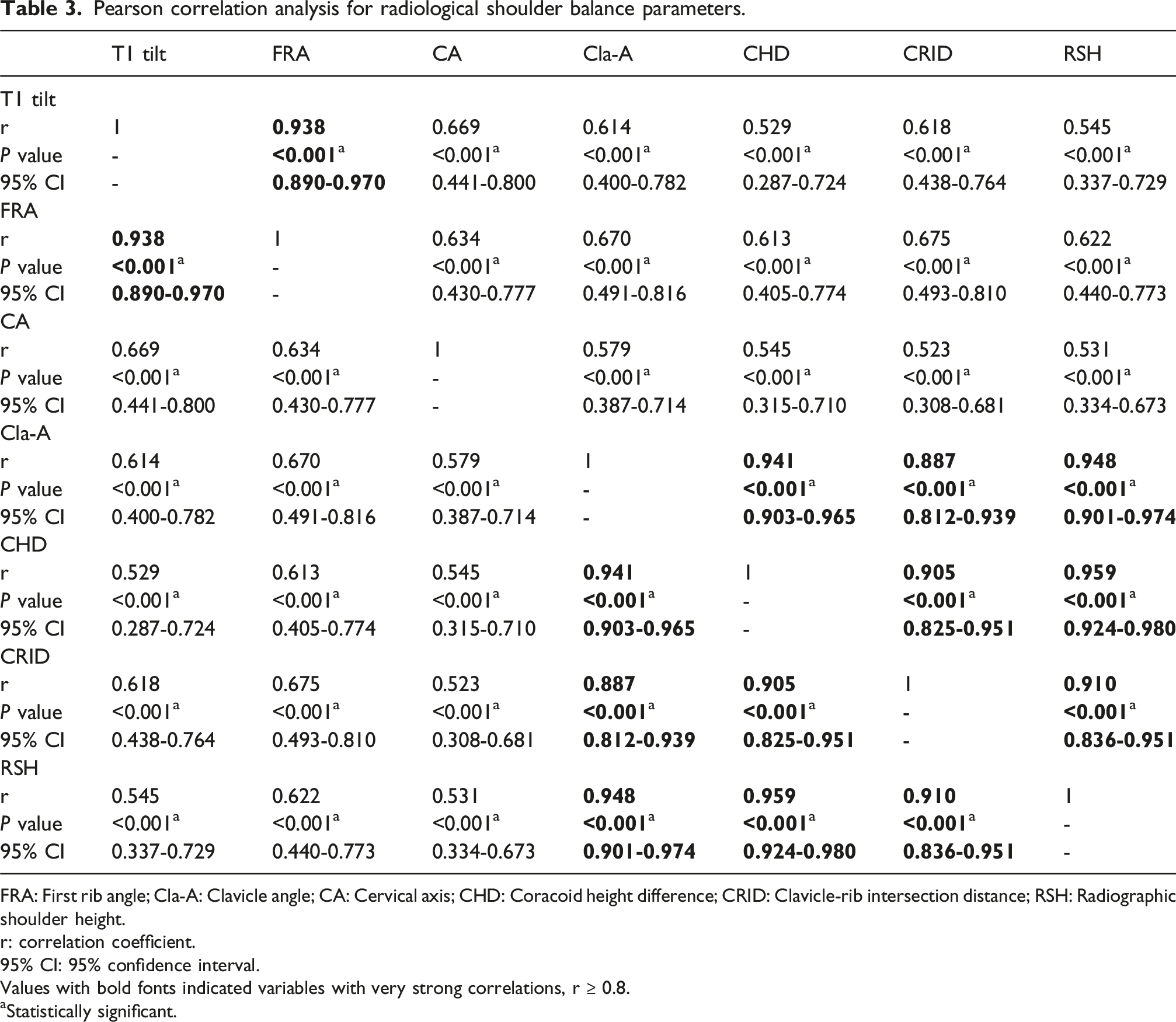
FRA: First rib angle; Cla-A: Clavicle angle; CA: Cervical axis; CHD: Coracoid height difference; CRID: Clavicle-rib intersection distance; RSH: Radiographic shoulder height.
r: correlation coefficient.
95% CI: 95% confidence interval.
Values with bold fonts indicated variables with very strong correlations, r ≥ 0.8.
aStatistically significant.
Correlation analysis between clinical and radiological shoulder balance parameters.
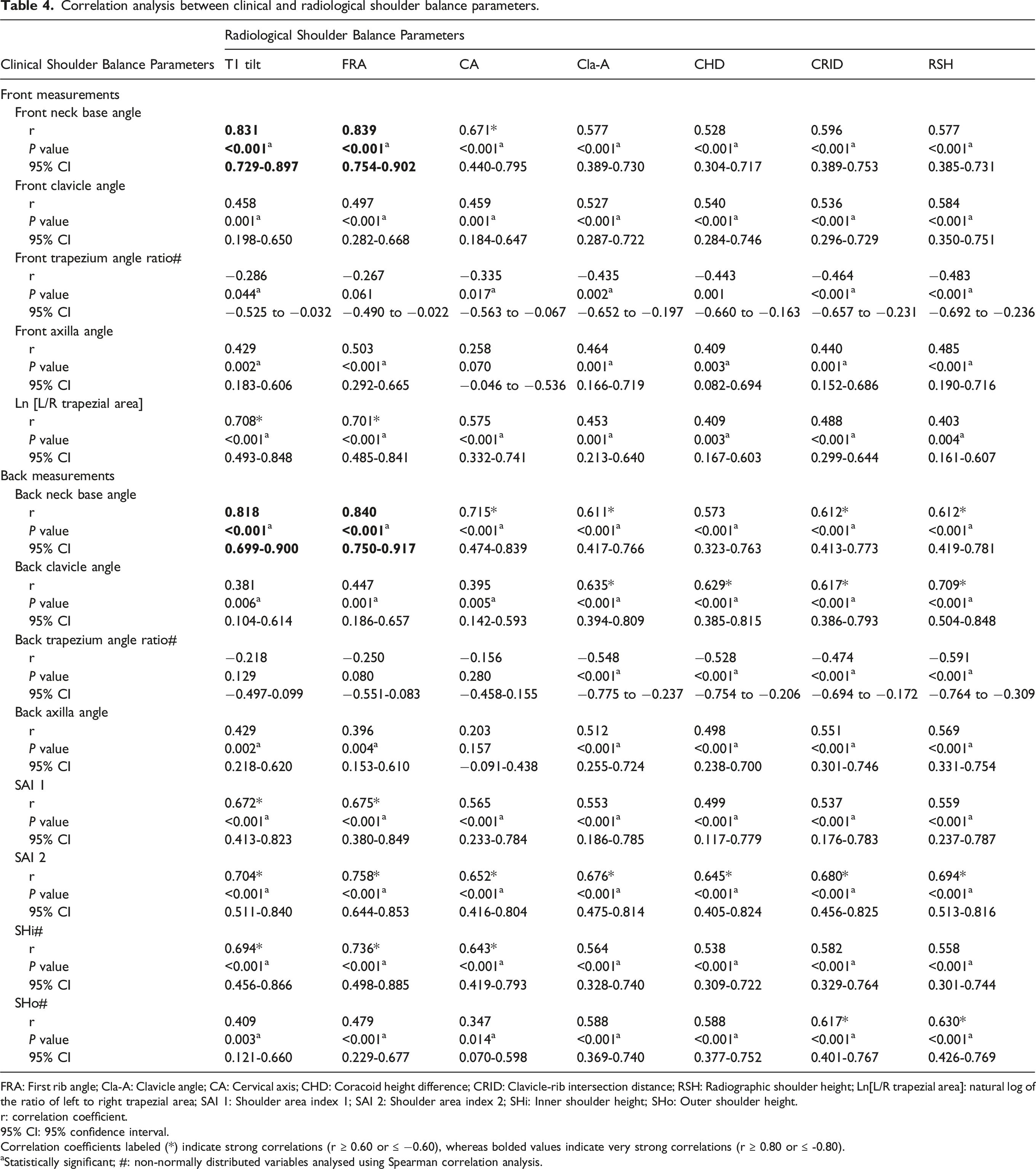
FRA: First rib angle; Cla-A: Clavicle angle; CA: Cervical axis; CHD: Coracoid height difference; CRID: Clavicle-rib intersection distance; RSH: Radiographic shoulder height; Ln[L/R trapezial area]: natural log of the ratio of left to right trapezial area; SAI 1: Shoulder area index 1; SAI 2: Shoulder area index 2; SHi: Inner shoulder height; SHo: Outer shoulder height.
r: correlation coefficient.
95% CI: 95% confidence interval.
Correlation coefficients labeled (*) indicate strong correlations (r ≥ 0.60 or ≤ −0.60), whereas bolded values indicate very strong correlations (r ≥ 0.80 or ≤ -0.80).
aStatistically significant; #: non-normally distributed variables analysed using Spearman correlation analysis.
On the contrary, only the back clavicle angle demonstrated a strong correlation with all LSB parameters, i.e., RSH (r = 0.709), Cla-A (r = 0.635), CHD (r = 0.629), and CRID (r = 0.617) (p < 0.001). SHo correlated strongly with CRID (r = 0.617) and RSH (r = 0.630) (p < 0.001). Meanwhile, front clavicle angle, front/back trapezium angle ratio, front/back axilla angle, did not have any strong correlation with MSB with neck tilt or LSB parameters (r < 0.6).
Discussion
In the recent years of research, shoulder balance has been evaluated as two distinct entities (MSB and LSB) whereas neck tilt as represented by CA was another constituent.1,3,7,8,10,13,14 Ono et al. 7 reported that clinical MSI (trapezial angle and Ln[L/R trapezial area]) correlated well with T1 tilt, FRA, and upper thoracic curve size while lateral shoulder imbalance (LSI) exhibited discrepancy to T1 tilt. Kuklo et al. 5 proposed Cla-A as a radiographic predictor for clinical shoulder balance as represented by RSH. Similarly, Kwan et al. 8 also reported significant correlations between clinical shoulder height, which represents LSB, and the radiological parameters (Cla-A, CHD, CRID, and RSH). The authors elaborated on clinical neck tilt (with/without MSI) and deduced that it correlated well with CA and T1 tilt. 8 Our results further affirmed that MSB with neck tilt and LSB were represented by different radiological parameters.
The results in this study supported that MSB, as represented radiologically by T1 tilt and FRA, had very strong correlations (r ≥ 0.8). This is consistent with the findings reported by Ono et al. 7 Furthermore, T1 tilt and FRA (MSB) correlated strongly with clinical parameters, i.e., front and back neck base angles, Ln [L/R trapezial area], SAI 1, SAI 2, and SHi. Interestingly, front and back neck base angles demonstrated very strong correlations (r ≥ 0.8) with T1 tilt and FRA, and they may be the best clinical indicators for MSB. However, back neck base angle and SAI 2 also demonstrated significant correlations with other radiological LSB parameters, suggesting that these parameters may lack specificity. In conjunction with other studies, our findings demonstrated a very strong correlation (r ≥ 0.8) between CHD, Cla-A, CRID, and RSH, which were indicative of LSB.8,11,15 We identified that the back clavicle angle demonstrated a strong correlation to radiological LSB, especially RSH (r = 0.709).
The feasibility of the shoulder balance measurements evaluated in this study supports their use in routine clinical assessment. Front-view evaluation appears to be more appropriate for assessing MSB. Based on our findings, the front neck base angle demonstrated stronger correlations with MSB-related parameters (r = 0.831 with T1 tilt; r = 0.839 with FRA), and may therefore better represent MSB. This parameter was previously described as trapezial angle by Ono et al., and was reported to have excellent intra-observer reliability (intraclass correlation coefficient (ICC) = 0.997). 7 In contrast, LSB appeared to be better represented by posterior clinical assessment, with the back clavicle angle showing stronger associations with LSB (CHD, Cla-A, CRID, and RSH). This parameter has demonstrated good inter-observer and intra-observer reliability (ICC = 0.80 and 0.88, respectively), as reported by Matamalas et al. 9 Collectively, these findings highlight the complementary roles of anterior and posterior assessments in characterizing shoulder balance. From a surgical planning perspective, UIV selection is commonly influenced by preoperative shoulder tilting, and previous studies have suggested that an elevated left shoulder may warrant a higher fusion level.16,17 Consequently, future studies investigating the targeted assessment of the MSB and LSB, establishing clinically pertinent thresholds for imbalance, may further facilitate the selection of UIV, potentially mitigating postoperative shoulder imbalance.
Nevertheless, our results were contrary to the findings of previous reports. We identified that most of the clinical shoulder parameters had moderate to strong correlations with radiological shoulder parameters for both MSB and LSB. A study of 80 idiopathic scoliosis patients by Matamalas et al., 9 reported weak to moderate correlations (r < 0.6) between clinical and radiological parameters despite being statistically significant. Qiu et al. 6 highlighted that none of the radiological shoulder parameters could precisely reflect the clinical parameters. However, the cut-off value applied in their study for a strong correlation coefficient was 0.8, which was higher than the common references. Yang et al. 18 evaluated the clinical and radiological shoulder balance of 74 Lenke 1 and 2 AIS patients. They observed that none of the radiological measures demonstrated a strong correlation (r > 0.8) with clinical shoulder balance. 18
Previous studies had investigated the effects of neck and shoulder imbalance on patients’ perception of clinical outcomes and deduced that it was associated with patients’ dissatisfaction.19,20 Postoperative shoulder imbalance not only led to patients’ dissatisfaction but might lead to possible complications, e.g., distal adding-on, lumbar curve progression, or postoperative truncal shift. 4 Therefore, recognising the potential clinical and radiological predictive factors is essential to avoid postoperative shoulder imbalance. For instance, preoperative shoulder balance, skeletal maturity, MT curve flexibility, UIV level selection, or UIV tilt angle, should be considered in the preoperative planning.21–24 Therefore, our findings could be applied as a guide in the preoperative measurement of clinical and radiological MSB with neck tilt and LSB.
This study solely concentrated on the preoperative data. We acknowledged that it was one main limitations in our study. Future studies could incorporate postoperative and long-term follow-up to further investigate the progression of neck and shoulder balance at different stages. Another limitation would be the discrepancy in the patients’ positioning during the clinical photography and radiography sessions. Patients might position themselves differently in both settings. A further limitation is the absence of a study-specific intra-observer and inter-observer reliability assessment using intraclass correlation coefficients. However, all clinical shoulder balance parameters reported in this study were derived from the previously published methodologies. Nevertheless, a previous study by Chiu et al. 25 concluded that T1 tilt had good reliability, CA, CRID and CHD had moderate reliability, whereas RSH and Cla-A had poor reliability.
Conclusion
MSB, as represented by T1 tilt and FRA, demonstrated very strong correlations with the front and back neck base angles (r ≥ 0.8), and strong correlations with Ln [L/R trapezial area], SAI 1, SAI 2, and SHi. Neck tilt, as represented by CA, correlated strongly with the front and back neck base angles, SAI 2, and SHi. LSB, as represented by Cla-A, CHD, CRID, and RSH, demonstrated a strong correlation with the back clavicle angle.
Footnotes
Acknowledgements
The authors would like to acknowledge Universiti Malaya Medical Centre for their invaluable support and assistance, which has contributed to the successful completion of this work.
Ethical considerations
This retrospective review was approved by our institutional review boards (MREC ID No.: 202214-10890).
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Mun Keong Kwan, Sin Ying Lee, and Woon Theng Heng. The first draft of the manuscript was written by Mun Keong Kwan, Sin Ying Lee, and Woon Theng Heng, Chee Kid Chiu, and Chris Yin Wei Chan. All authors commented on and reviewed previous versions of the manuscript. Mun Keong Kwan was responsible for conceptualization, methodology, supervision, and providing resources for the study. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.