
Abstract
Purpose
: Titanium volar locking plates are widely used in distal radius fractures (DFRs) fixation, but their induction of radiographic shielding hinders fracture assessment. Carbon fiber-reinforced polyether ether ketone (CFR-PEEK) plates are radiolucent and biomechanically comparable to titanium, potentially improving intraoperative visualization and postoperative follow-up. This study aims to compare clinical and radiographic outcomes between CFR-PEEK and titanium plates.
Methods
This retrospective study included 39 patients with DRFs treated with either CFR-PEEK (n = 19) or titanium plates (n = 20) between August 2018 and June 2019. Intraoperative and postoperative parameters were compared between the two groups. The Wilcoxon rank sum test and Fisher’s exact test were applied for statistical analysis.
Results
Satisfactory fracture reduction without implant-related complications was achieved in both groups. At 12 months, wrist range of motion and radiographic alignment did not significantly differ between the groups (both p > 0.05), and Disabilities of the Arm, Shoulder and Hand (DASH) scores were comparable between the groups (11.8 ± 7.0 vs 11.9 ± 4.6, p > 0.05). Notably, intraoperative CFR-PEEK plates significantly reduced the operative time compared with titanium plates (64.16 ± 15.24 min vs 78.4 ± 20.63 min, p = 0.0387). The implant removal rates did not differ between the groups.
Conclusion
CFR-PEEK volar locking plates demonstrated clinical and radiographic outcomes comparable to titanium plates, with added advantages of radiolucency and surgical efficiency, including a significantly shorter operative time. These findings identify CFR-PEEK plates as a safe and effective alternative in DRFs fixation.
Keywords
Introduction
In recent years, orthopedic surgeons have recognized open reduction and internal fixation with plates as a viable treatment method for distal radius fractures (DRFs), especially those with unstable and comminuted fracture patterns, because it ensures immediate stable fixation and promotes early mobilization, which is crucial for recovery. 1 The advent of volar locking plates, such as those with fixed-angle screws, has produced enhanced treatment outcomes for DRFs. 1 Using these plates, surgeons can perform anatomical reduction with relative ease and effectively maintain the reduction until bone healing occurs, thereby permitting immediate postoperative mobilization. Consequently, the use of plates in the surgical treatment of DRFs can facilitate rapid recovery and improve functional mobility. 2
This study compared clinical and radiographic outcomes between CFR-PEEK and titanium plates in the treatment of DRFs. CFR-PEEK implants offer several advantages over titanium implants, including a reduced incidence of allergic reactions in patients with metal allergies, avoidance of misinterpretation of local imaging because of radiolucency, and reduced signal interference in magnetic resonance imaging (MRI).3–5 Moreover, prior studies demonstrated that CFR-PEEK implants exhibit superior strength, toughness, and fatigue resistance compared with metal implants, and CFR-PEEK plates also display high corrosion resistance and a favorable strength-to-weight ratio. 6
Furthermore, CFR-PEEK has comparable stiffness as bone, which is advantageous for fixation devices because it helps prevent proximal bone density loss, potentially mitigate stress shielding, and potentially decrease the risk of construct failure in osteoporotic bone. 7 The use of CFR-PEEK plates eliminates the risk of cold welding between screws and the plate, a phenomenon that can occur with titanium plates. 8 The distinctive design of CFR-PEEK components allows screw insertion in multiple directions relative to the screw axis, thereby conferring robust construct strength to the plate–screw assembly. 5
There is mounting clinical evidence supporting the efficacy of carbon fiber-reinforced polyether ether ketone (CFR-PEEK) implants in orthopedic, trauma, and spinal surgery.9–11 CFR-PEEK plates are radiolucent and biomechanically comparable to titanium, and they can potentially improve intraoperative visualization and postoperative follow-up. However, existing research has not provided conclusive evidence that CFR-PEEK plates significantly improve surgical efficiency versus conventional titanium plates.2,12 Therefore, this retrospective study compared the clinical and radiological outcomes of patients with DRFs treated with CFR-PEEK volar locking plates or conventional titanium volar locking plates.
Given that both implants are volar locking plates with similar geometry and that all procedures were performed by the same surgeon using a standardized technique, our primary aim was to compare 12-months clinical and radiographic outcomes between CFR-PEEK and titanium plates, while a secondary aim was to explore potential intraoperative workflow advantages associated with radiolucency (e.g., operative time).
Materials and methods
Between August 2018 and June 2019, 39 patients with AO/OTA Fracture and Dislocation Classification type A–C DRFs underwent open reduction and internal fixation with CFR-PEEK plates (CarboFix Orthopedics Ltd, Herzliya, Israel) or titanium plates (DePuy Synthes, Raynham, MA, USA) by the same experienced hand surgeon. Patients were followed for at least 12 months after surgery.
Regarding the inclusion criteria, patients with DRFs with surgical indications (shortening >5 mm, radial inclination <15°, dorsal angulation >10° or volar angulation >25°, articular step-off >2 mm, disruption of the lateral radiocarpal alignment) were included. Meanwhile, the exclusion criteria were as follows: open fractures, bilateral wrist fractures, other ipsilateral upper-limb fractures, multiple fractures, concomitant major trauma, and lost to outpatient follow-up.
Surgical technique
Under general anesthesia, patients were positioned supine with the hand on the surgically treated arm extended. A tourniquet was applied to the upper arm, with pressure increased at least 120 mmHg above systolic blood pressure. A modified Henry approach with a pronator quadratus split was used. 13 After fracture reduction, the CFR-PEEK plate or titanium volar locking plate was positioned under fluoroscopic guidance. The plate–screw construct was completed in a step-by-step manner. Final reduction and the internal fixation construct were subsequently evaluated under fluoroscopic guidance under the anteroposterior, posteroanterior, lateral, and dorsal tangential views, in addition to a lateral view with 30° of elbow flexion, to eliminate the possibility of penetration of the joint space by locking screws and/or extensor tendon injury attributable to incorrect screw length. 14 The wound was irrigated with saline, closed in layers, and covered with gauze, and the wrist was immobilized with a short-arm splint.
Postoperative management
Patients were immobilized in a short-arm splint for 4 weeks. Active finger range-of-motion exercises were initiated immediately after surgery to facilitate edema control. At 4 weeks, the splint was removed and progressive wrist mobilization and formal rehabilitation were commenced. Exercise intensity was advanced according to clinical status, and therapy was continued through postoperative week 8.
Clinical evaluation
A standardized clinical functional assessment was conducted 12 months after to assess progress and outcomes. The Disabilities of the Arm, Shoulder, and Hand (DASH) score (0–100, with 0 denoting no functional impairment and 100 indicating the highest level of disability) and the ranges of wrist extension, flexion, supination, and pronation were evaluated. The operative time and implant removal rate were also assessed.
Radiographic evaluation
Standardized radiological assessments, including dorsopalmar and lateral X-rays, were conducted both before and after surgery. A follow-up evaluation was performed 12 months after surgery. Each assessment was conducted by a senior resident and the same fellow. Postoperative measurements included the scapholunate angle, radial height, radial inclination, volar tilt, and ulnar variance. The scapholunate angle was measured between the longitudinal axis of the lunate (drawn perpendicular to a line joining the dorsal and volar poles of the lunate) and a line paralleling the volar cortices of the proximal and distal convexities of the scaphoid. 15 Volar tilt was assessed on the lateral radiograph as the angle formed by a line drawn perpendicular to the radial shaft axis and a line passing through the tips of the dorsal and volar rims of the distal radial articular surface (normal, 11° ± 5°). 16 Radial inclination was measured on the anteroposterior projection as the angle between a line drawn from the radial styloid to the ulnar border of the distal radius and a line perpendicular to the radial shaft (normal, 22° ± 3°). 17 Radial height represented the difference in length between the ulnar head and the tip of the radial styloid on the PA view (normal, 14 ± 1 mm). 17 Ulnar variance represented the distance between two lines perpendicular to the central axis of the radius at 3 and 5 cm below the midpoint of the proximal lunate articular surface, including one line through the distal ulnar articular surface and the other through the medial radial articular surface. This value is negative when the ulnar articular surface is more proximal and positive when it is more distal. 18
Statistical analysis
Wilcoxon’s rank sum test was used to assess continuous variables (age, body mass index, operative time, DASH score, wrist flexion, extension, pronation, supination, and radiographic parameters). Fisher’s exact test was used for categorical variables (sex and implant removal rate). Statistical significance was denoted by p < 0.05.
As this was a retrospective consecutive cohort, no a priori sample size calculation was performed. Therefore, the study should be considered exploratory, and non-significant differences must be interpreted with caution given the risk of type II error.
Results
Demographic characteristics of the participants
Demographic characteristics of patients with distal radius fractures treated with CFR-PEEK versus titanium volar locking plates.

*n: number; M±SD: mean ± standard deviation.
aWilcoxon rank sum test.
bFisher’s exact test.
Clinical outcomes
Clinical outcomes.

*n: number; M±SD: mean ± standard deviation; ROM: range of motion.
aWilcoxon rank sum test.
bFisher’s exact test.
Radiographic outcomes
Radiographic outcomes.
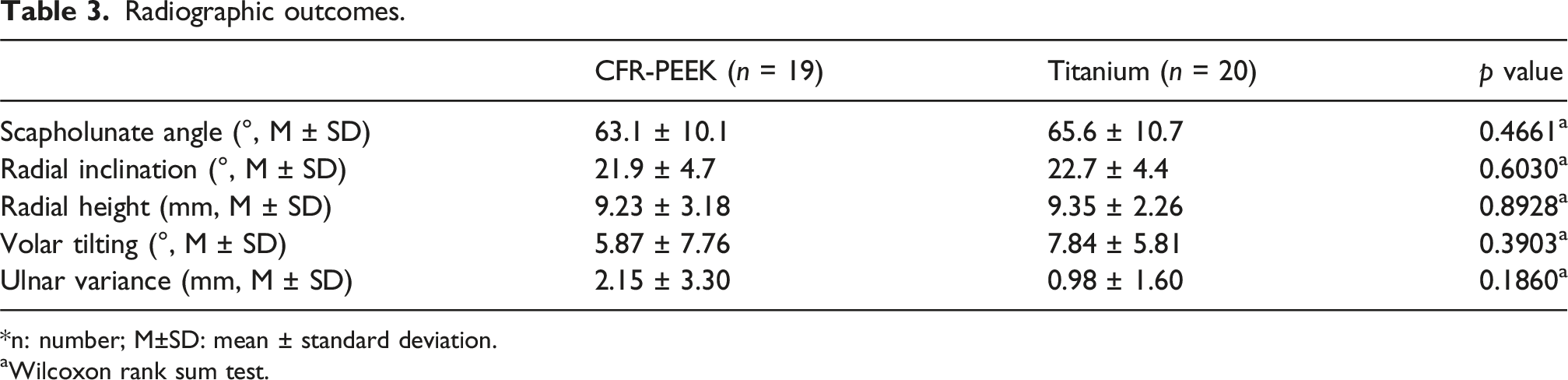
*n: number; M±SD: mean ± standard deviation.
aWilcoxon rank sum test.
Discussion
In this study, CFR-PEEK plates achieved comparable outcomes as titanium plates in terms of fracture alignment, wrist ROM, DASH scores, and implant removal rates. Compared with conventional titanium plates, CFR-PEEK plates offer distinct intraoperative advantages owing to their radiolucency, and they were associated with a significantly shorter operative time, which could confer potential benefits in older patients or patients with multiple comorbidities by minimizing the surgical duration and exposure to general anesthesia, an aspect that was not addressed in previous studies.
Comparison with previous literature
Our results align with those of previous biomechanical studies demonstrating that CFR-PEEK implants provide equivalent stability as metallic plates while reducing stress-shielding effects.6,19 Recent clinical reports also support the safety of volar PEEK plates in DRF fixation, which achieved comparable complication rates as titanium.12,20 However, few studies directly compared CFR-PEEK and titanium plates in clinical cohorts. Through this head-to-head comparison, the present study adds important evidence to the growing literature on CFR-PEEK implants.1–3,5,12
Clinical implications
Titanium volar locking plates are widely used to correct DRFs, but their induction of radiographic shielding hinders fracture assessment. The radiolucency of CFR-PEEK implants represents a practical advantage over titanium plates during both intraoperative fluoroscopy and postoperative follow-up (Figure 1). Unlike titanium plates, CFR-PEEK permits unobstructed visualization of fracture lines, enabling precise reduction and implant placement without temporary Kirschner wire insertion (Figure 2). This technical benefit can translate into shorter operative times and reduced soft-tissue disruption. Radiographic comparison during reduction. Left: Titanium volar locking plate used for fracture reduction causes radiographic shielding. Right: CFR-PEEK volar locking plate used for reduction demonstrates radiolucency, permitting clear visualization of the fracture position. Surgical technique for the CFR-PEEK plate. Left: During fracture reduction, the CFR-PEEK plate is inserted to facilitate simultaneous reduction and fixation. Right: Final fluoroscopic view after reduction displaying anatomic alignment.

Strengths and limitations
The strengths of this study included the use of a uniform surgical technique by the same experienced hand surgeon and standardized assessments at 12 months. Nonetheless, several limitations must be acknowledged. Specifically, the retrospective design and modest sample size limited statistical power and generalizability, the follow-up period was relatively short, precluding evaluation of long-term complications such as post-traumatic arthritis or late implant failure, and minor imbalances in the fracture type distribution could have influenced outcomes (Figure 3). Serial radiographs in anteroposterior and lateral views. Preoperative images (a and b) demonstrate a distal radius fracture. Immediate postoperative images (c and d) show satisfactory fracture reduction and internal fixation with a radiolucent CFR-PEEK volar locking plate. At 3 months postoperatively, follow-up radiographs (e and f) indicate fracture union, which can be more readily appreciated due to the plate’s radiolucency.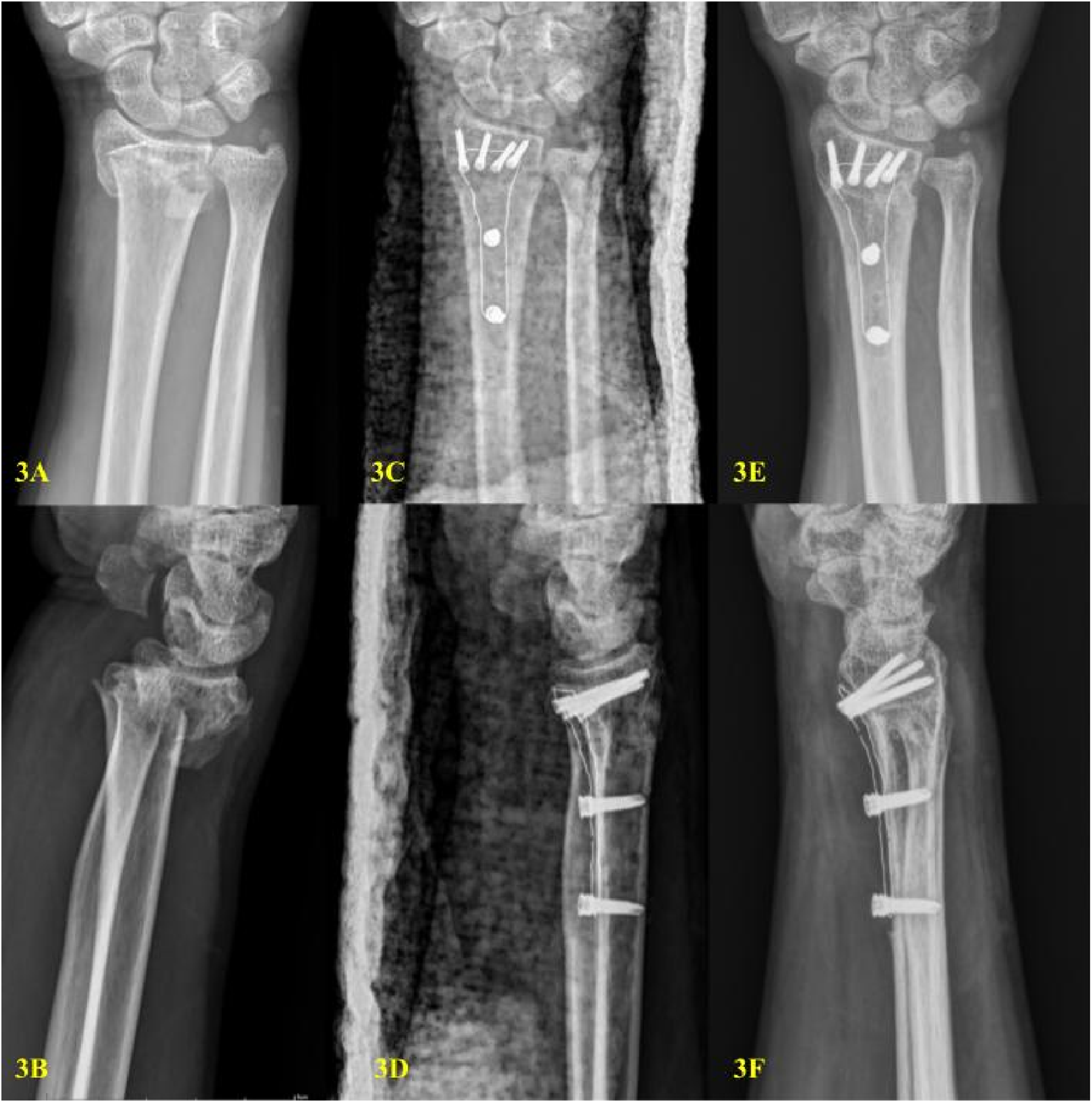
The modest sample size limits statistical power to detect small between-group differences. Based on the observed variability of functional scores, the present cohort would be expected to detect only moderate differences; smaller clinically relevant differences may have been missed.
Future directions
Future work should include large-scale post-market surveillance and registry-based real-world evidence to better characterize uncommon mechanical failure modes, complication patterns, reoperation rates, and potential health-economic impact of CFR-PEEK implants. Multicenter prospective studies may complement these data; however, real-world datasets are particularly valuable for evaluating device performance beyond small comparative cohorts.
Conclusion
CFR-PEEK volar locking plates achieved comparable, and in some aspects superior, clinical and radiographic outcomes as conventional titanium plates in the fixation of unstable DRFs, particularly in terms of the operative time. The radiolucency, biocompatibility, and potential of CFR-PEEK plates to improve postoperative functional recovery underscore their translational significance as an advanced implant technology. These findings suggest that CFR-PEEK plates represent both a safe alternative and a paradigm shift in the surgical management of DRFs. Prospective multicenter trials are warranted to further validate their role in shaping future clinical practice.
Footnotes
Consent to participate
Patient consent was waived due to the observational design of this study, with approval granted by the Institutional Review Board.
Author contributions
All authors conceptualized the article. Research design: Kun-Yi Lin. Acquisition, analysis or interpretation of the data: Tse-Pu Huang, Hui-Sen Tseng; Zhi-Hong, Zheng. Drafting the manuscript: Tse-Pu Huang. Revising the manuscript: Zhi-Hong, Zheng; Kun-Yi Lin; Pei-Hung, Shen. All authors have read and approved the final submitted manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study are contained in the article. Requests for further details may be directed to the corresponding author.
Institutional review board statement
This retrospective study received approval from the Institutional Review Board of Tri-Service General Hospital (Approval Number: A202105142). All procedures adhered to applicable guidelines and regulations. This study has been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.