
Abstract
Background
Total hip arthroplasty (THA) is an effective treatment for hip osteoarthritis (OA), improving pain, function, and quality of life (QOL). The Hip disability and Osteoarthritis Outcome Score (HOOS) is widely used to assess treatment outcomes; however, the minimal clinically important difference (MCID) in the short-term remains unclear. This study aimed to determine MCID values for HOOS at 3 and 6 months post-THA using the anchor method.
Methods
This multicenter prospective cohort study included patients with hip OA undergoing primary unilateral THA. HOOS subscales (symptoms, pain, activities of daily living [ADL], sport and recreation [SR], and QOL) were assessed preoperatively and at 3 and 6 months postoperatively. MCID was determined using receiver operating characteristic analyses with the Global Rating of Change scale as the anchor.
Results
A total of 127 patients were included in the analysis, with 107 patients assessed at 3 months and 102 at 6 months post-THA. At 3 months after THA, the MCID values for the HOOS subscales were 7.50 for symptoms, 8.75 for pain, 4.41 for ADL, 9.38 for SR, and 9.38 for QOL. At 6 months after THA, the corresponding MCID values were 12.50, 11.25, 23.53, 10.00, and 15.63, respectively.
Conclusion
Short-term MCID values for HOOS subscales post-THA were established, aiding early assessment of treatment effectiveness and guiding postoperative care.
Keywords
Introduction
Total hip arthroplasty (THA) is widely performed for individuals with advanced hip disease, especially for those suffering from end-stage hip osteoarthritis (OA), and is known to substantially relieve hip-related symptoms while enabling the restoration of daily function and improvement in overall well-being. 1 Because postoperative recovery trajectories vary, the systematic evaluation of patient outcomes has become increasingly important to inform clinical decision-making. In contemporary practice, treatment benefits are primarily captured using patient-reported outcome measures (PROM), which provide direct insight into how patients perceive changes after THA. 2 Among these, the Hip disability and Osteoarthritis Outcome Score (HOOS) is a highly reliable, valid, and responsive tool widely applied in clinical settings to evaluate postoperative outcomes.3–5 HOOS evaluates five subscales—symptoms, pain, activities of daily living (ADL), sport and recreation (SR), and quality of life (QOL)—making it a comprehensive tool to quantify recovery after THA. 6
Interpreting treatment effects using the minimal clinically important difference (MCID) of HOOS subscales facilitates patient-centered care. Statistical significance does not necessarily imply clinical significance. 7 MCID represents the smallest change in a measurement that reflects a meaningful improvement following treatment. 7 A treatment-induced change exceeding the MCID threshold is considered clinically meaningful. 8 MCID is commonly estimated using anchor-based and distribution-based methods. 9 Previous studies have reported lower validity for distribution-based MCID values, as they often fall below the minimal detectable change at 80%, 90%, and 95% confidence levels. 10 In contrast, MCID values derived from the anchor-based method effectively distinguish between improved and non-improved patients, demonstrating high area under the curve (AUC) values in receiver operating characteristic (ROC) analysis. 10 Therefore, the anchor-based MCID may provide a more reliable reference for clinical applications.
Although long-term MCID values for HOOS at 1 or 2 years post-THA have been established,10–12 short-term MCID values at 3 and 6 months remain largely unexplored. Moreover, MCID values for individual HOOS subscales have not been fully elucidated. Establishing short-term MCID values for HOOS would aid early clinical decision-making regarding treatment continuation. Although previously reported MCID values have varied across studies,10–13 identifying diverse MCID values based on the timing of evaluation, patient demographics, and surgical approaches may help clinicians assess treatment effectiveness more accurately.
This study aimed to determine short-term postoperative MCID values for each HOOS subscale using the anchor method and to evaluate the proportion of patients achieving MCID for each subscale.
Materials and methods
Ethics
This multicenter study received ethical approval through a single institutional review board review process, which covered all participating sites. The study protocol complied with the principles of the Declaration of Helsinki, and only non-invasive assessments required for evaluating functional status were performed. Written informed consent was obtained from all participants prior to enrollment.
Study design
This 6-month follow-up multicenter prospective cohort study determined MCIDs for HOOS subscales at 3 and 6 months post-THA using the anchor method.
Setting
The study was conducted in the rehabilitation department of three facilities. Recruitment, follow-up, and data collection occurred between February 2023 and April 2025.
Participants
Eligible participants were adults diagnosed with hip OA who underwent primary unilateral THA and were able to ambulate independently, either with or without assistive devices, both before and after THA. Individuals were excluded if they had comorbidities or postoperative events likely to affect HOOS scores, including rheumatoid arthritis, systemic lupus erythematosus, cognitive or psychiatric disorders, femoral head necrosis, major complications after THA (such as deep vein thrombosis or periprosthetic fracture), or underwent revision THA.14–20 Participants with incomplete HOOS data were also excluded from the final dataset.
A unified postoperative rehabilitation protocol was implemented across all facilities. Therapy commenced on postoperative day 1 and comprised progressive lower-limb resistance training, joint range-of-motion exercises, gait training, and targeted muscle strengthening for the hip, knee, and ankle. Following hospital discharge, participants attended outpatient sessions approximately once per week. Supervised rehabilitation was completed within 150 days after THA.
Variables
The primary endpoints were the MCIDs for the HOOS at 3 and 6 months post-THA. The HOOS consists of 40 questions across five subscales: symptoms, pain, ADL, SR, and QOL. 3 The HOOS questionnaire includes five questions for symptoms, 10 for pain, 17 for ADL, 4 for SR, and 4 for QOL. Each subscale has five response options, with 0% indicating the worst condition and 100% the best. HOOS is a highly valid, responsive, and reliable PROM for THA.3,5
Statistical analysis
MCID was calculated using the anchor method, with the Global Rating of Change (GRC) scale as the anchor. 21 Improvement in each subscale was evaluated using the 11-point GRC scale (−5 to +5), where higher positive values indicated better postoperative recovery. The 11-point GRC scale has high discriminative power. 21 A change of ≥2 points was considered clinically meaningful. 21 Patients scoring +2 or more on the GRC scale were classified as the improvement group, whereas those scoring +1 or less were classified as the non-improvement group. ROC curves were constructed using HOOS subscale score changes from preoperative to 3 and 6 months postoperative. MCID was determined using the Youden index. 22 The percentage of patients with THA achieving MCID by subscale was also calculated. All statistical analyses were performed using IBM SPSS statistics version 30.0 (IBM Corp., Armonk, NY, USA).
Sample size
Sample size estimation was conducted using MedCalc statistical software version 23.1.7 (MedCalc Software bvba, Ostend, Belgium). The analysis was performed assuming a type I error rate of 0.05, statistical power of 0.80, and a null AUC value of 0.50. The AUC values were interpreted as follows: non-predictive (AUC <0.5), low predictive capacity (0.5≤ AUC <0.7), moderate predictive capacity (0.7≤ AUC <0.9), high predictive capacity (0.9≤ AUC <1), and perfect prediction (AUC = 1).23,24 Because previous studies investigating MCID after THA have reported AUC values of 0.89–0.93, a conservative expected AUC of 0.80 was selected for the present sample size calculation. 25 The allocation ratio for the ROC analysis was informed by published postoperative distributions of improvement and non-improvement groups, setting the proportions at 0.94 and 0.06, respectively. 25 Applying these parameters, the minimum total sample size required was estimated to be 101 participants, comprising approximately 94 in the improvement group and 7 in the non-improvement group.
Results
Cohort characteristics
Of the 127 eligible patients, 107 were followed up at 3 months. At 6 months, 102 remained, whereas five were lost to follow-up (Figure 1). Baseline characteristics and HOOS data before and after THA are shown in Tables 1 and 2, respectively. Study flow diagram. HOOS, Hip disability and Osteoarthritis Outcome Score; THA, total hip arthroplasty. Baseline patient characteristics. Values are presented as mean ± standard deviation. ASA, American Society of Anesthesiologists physical status classification; BMI, body mass index; CCI, Charlson comorbidity index; THA, total hip arthroplasty; WHO, World Health Organization. HOOS subscale scores pre-THA and at 3 and 6 months post-THA. Values are presented as mean ± standard deviation. ADL, activities of daily living; HOOS, Hip disability and Osteoarthritis Outcome Score; QOL, quality of life; SR, sport and recreation; THA, total hip arthroplasty.


Minimally clinically important difference
MCID thresholds for HOOS at 3 months post-THA.
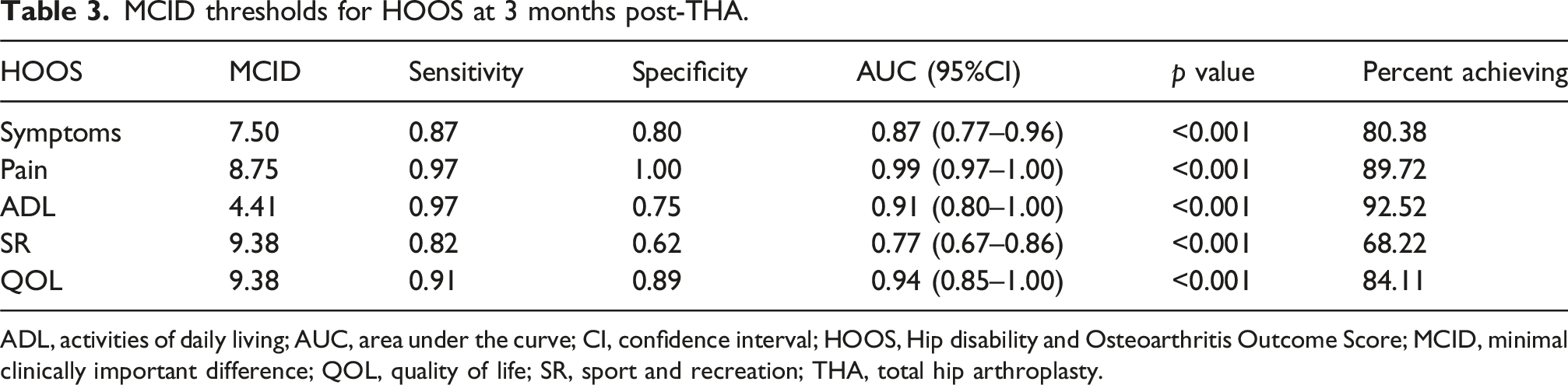
ADL, activities of daily living; AUC, area under the curve; CI, confidence interval; HOOS, Hip disability and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; QOL, quality of life; SR, sport and recreation; THA, total hip arthroplasty.
MCID thresholds for HOOS at 6 months post-THA.

ADL, activities of daily living; AUC, area under the curve; CI, confidence interval; HOOS, Hip disability and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; QOL, quality of life; SR, sport and recreation; THA, total hip arthroplasty.
Discussion
This study determined the MCID of HOOS subscales at 3 and 6 months post-THA, with AUC values of at least 0.77 for all subscales, confirming statistical significance. These findings support the validity of MCID as a measure for assessing postoperative improvements across subscales.
This study is the first to calculate MCID for HOOS subscales at 3 and 6 months post-THA. In previous studies, all MCIDs calculated by HOOS subscale were after 1 year post-THA.10–12 Compared to prior findings—symptoms (17.0), pain (27.5), ADL (19.1), SR (16.7), and QOL (6.0) 12 —the MCID values observed at 3 months in this study were lower for all subscales except for QOL. At 6 months, the MCIDs for ADL and QOL exceeded the prior 1-year estimate, while the MCIDs for symptoms, pain, and SR remained lower. This difference may be attributed to the progressive improvement in physical function over time following THA.26,27 Additionally, the higher MCID values for ADL and QOL at 6 months post-THA in this study may reflect differences in patient demographics and treatment methods.
A notable finding of this study was the marked increase in the MCID threshold for the ADL subscale from 3 months (4.41) to 6 months (23.53) post-THA. Although this change may appear substantial, it should be interpreted in the context of the anchor-based MCID methodology. MCID is not a fixed biological constant but is rather a time-dependent construct that reflects patients’ perception of meaningful change relative to their recovery stage. At 3 months post-THA, many patients experienced rapid functional gains, and even small improvements in basic daily activities may be perceived as clinically meaningful. In contrast, by 6 months, functional recovery has progressed substantially, and patients have often recalibrated their internal standards, requiring larger absolute improvements in ADL scores to perceive further change as meaningful. This shift results in a higher MCID threshold despite continued clinical improvement, rather than indicating instability of the measurement itself. Importantly, the diagnostic performance of the ADL MCID at 6 months remained good (AUC = 0.86), supporting the interpretability of this threshold despite its higher absolute value.
The SR subscale demonstrated the lowest MCID achievement rates at both 3 and 6 months compared with the other subscales. This is consistent with the predominantly older study population, for whom high-level activities are less likely to be regained early after THA. Although HOOS was originally designed to accommodate a wide range of functional expectations—including younger or more active patients—older adults may face slower or more heterogeneous recovery patterns in sport-related tasks. 28 For older adults seeking to return to SR, individualized interventions may be necessary alongside standard rehabilitation. Furthermore, the AUC for MCID in SR remained below 0.8, warranting caution when interpreting treatment effectiveness. 29
The primary strength of this study was the first calculation of MCID by HOOS subscales in the short-term after THA for hip OA. The ability to clarify treatment effects earlier would be beneficial to both clinicians and patients, contributing significantly to patient-centered care. Nevertheless, this study has several limitations. First, the sample size in this study was not sufficient for generalization. Although the study size allowed validation of moderate predictive value, the findings may not have represented the entire population of patients undergoing THA worldwide. In particular, more than 90% of the cohort consisted of female patients. This sex distribution may reflect the epidemiology of hip OA in Japan, where acetabular dysplasia—more common in female—frequently contributes to the development of secondary hip OA and subsequent THA. 30 However, the underlying etiology of hip OA (primary age-related vs secondary dysplasia-related) was not systematically assessed in this study. Therefore, it was not possible to stratify MCID values according to disease etiology, and the derived thresholds likely represent aggregated estimates across a heterogeneous hip OA population. Given that both sex and disease etiology may influence postoperative recovery trajectories and patient-reported outcome responses, this imbalance may limit the external validity of the MCID estimates, particularly when applied to male patients or to populations wherein primary OA predominates. 31 Future studies with larger and more demographically balanced cohorts are needed to establish etiology-specific MCID thresholds and to enhance the generalizability of these findings across diverse patient populations. Second, SR subscale demonstrated only fair discriminative ability at both 3 and 6 months postoperatively (AUC <0.8). This finding is likely attributable to the advanced age of the study cohort and limited engagement in high-demand activities during the early postoperative period. In older patients undergoing THA, the recovery of SR-related functions is often delayed or heterogeneous, which may reduce the ability of short-term score changes to discriminate between clinically meaningful and non-meaningful improvement. Third, adjustments for factors influencing HOOS results, such as socioeconomic determinants and physical activity, remained inadequate. A lower educational level has been associated with worse pain and physical function, 32 and inactive patients undergoing THA experience greater improvements in physical activity levels than those who were active before surgery. 33 Future studies should adjust for these factors. Finally, differences in THA techniques and their impact on MCID could not be examined. Variations in functional recovery speed and pain relief may exist across surgical techniques, warranting further investigation.34,35
Conclusion
In this study, we calculated MCID by HOOS subscales at 3 and 6 months postoperatively for patients undergoing primary unilateral THA for hip OA. These findings may be useful in evaluating the effectiveness of various interventions and treatments for patients who have undergone THA.
Footnotes
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.