
Abstract
Introduction
Total Hip Arthroplasty (THA) is a widely performed orthopaedic surgery, essential for treating severe pain and mobility issues arising from various conditions. The anticipated rise in Total Hip Arthroplasty (THA) procedures underscores the critical importance of their success, which is heavily dependent on the accurate positioning of prosthetic components. Various approaches like the Direct Anterior Approach with Fluoroscopy (DAA-F THA) and Robotic-assisted THA (RA THA) have their limitations. Computer-Navigated THA (CN THA) has emerged as a promising alternative, offering real-time feedback and potentially enhanced accuracy in component placement. This study evaluates the precision of CN THA in correcting leg length discrepancies and accurately positioning the acetabular component.
Methods
The study involved 122 consecutive patients undergoing direct anterior CN THA by the senior author. Exclusions were based on different surgical approaches, need for revision surgery, and infections. The study focused on the precise placement of acetabular components and leg length restoration. CN THA was used for intra-operative measurements, while post-operative radiographs were analyzed with TraumaCad® for comparison. Statistical analyses included Pearson correlation coefficients and descriptive analyses.
Results
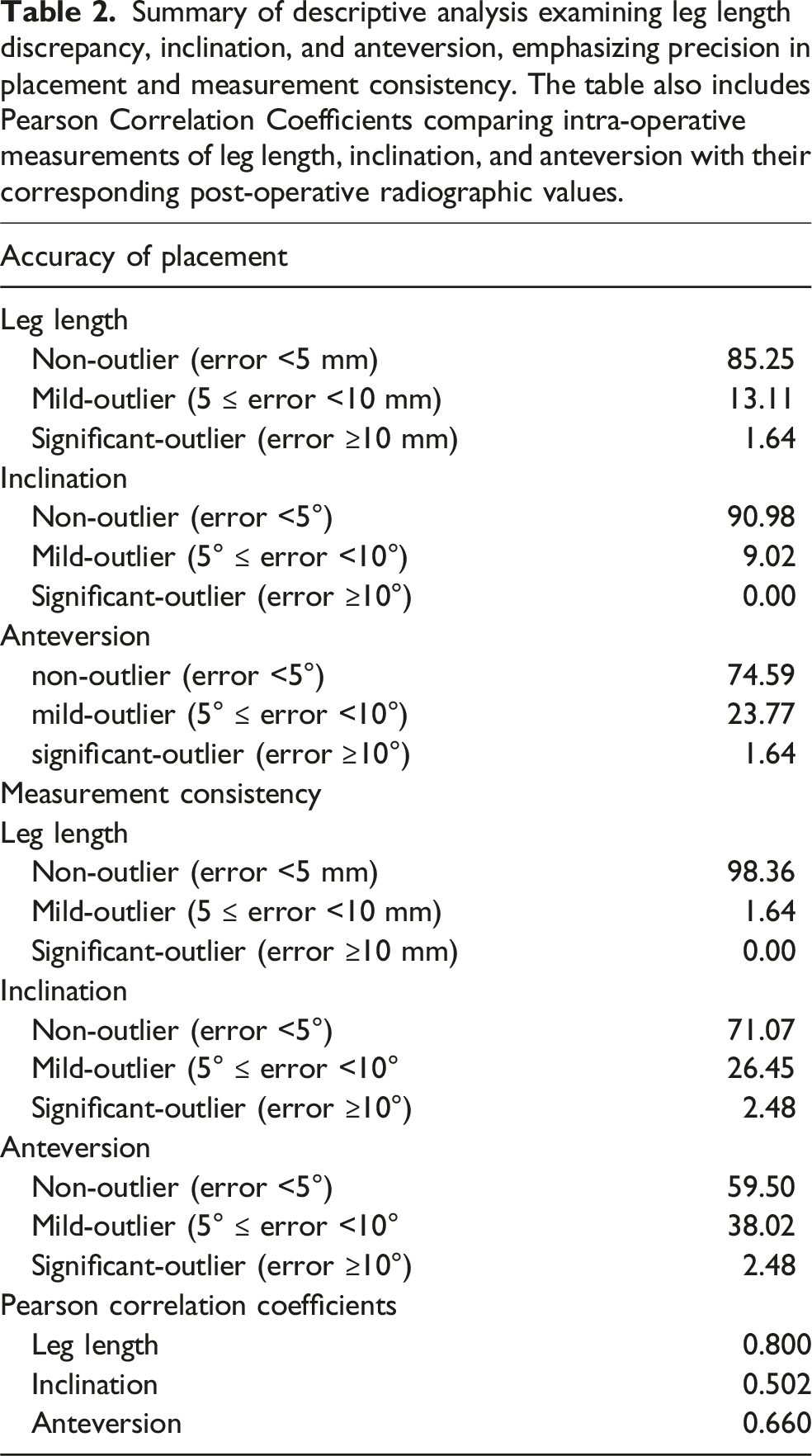
CN THA showed high accuracy in leg length restoration with 85.25% of cases showing less than 5 mm discrepancy. Similarly, acetabular component positioning was precise, with 90.98% of inclination and 74.59% of anteversion measurements within acceptable ranges. The correlation between intra-operative and post-operative measurements was strong, indicating the reliability of CN THA measurements.
Conclusion
CN THA was shown to be highly accurate in correcting leg length discrepancies and achieving proper acetabular component positioning. The strong correlation between intra- and post-operative measurements underscores the reliability of CN THA. The study, however, is limited by its single-surgeon, single-approach design, and lack of a control group. Despite these limitations, CN THA shows considerable potential in improving THA precision, enhancing surgical outcomes, and customizing patient care.
Keywords
Introduction
Total Hip Arthroplasty (THA) is one of the most common and successful orthopaedic surgeries performed worldwide. 1 This surgery is typically indicated for individuals suffering from severe pain and diminished mobility due to conditions like osteoarthritis, rheumatoid arthritis, osteonecrosis, or traumatic injury. As many as 500,000 THA’s are performed every year in the United States, and that number is projected to grow to between 575,000 and 635,000 procedures, by 2030.2,3 This surge reflects not only an aging population but also the expanding indications for THA in younger, more active patients. 4 Given these trends, ensuring a high success rate in THA is paramount.
The success of a THA is critically dependent on the precise positioning of the prosthetic components, a factor that significantly influences postoperative outcomes. 5 The positioning of the acetabular cup, in particular, is a key determinant of the surgery’s success, as it directly impacts the wear of the polyethylene liner, the range of motion achievable, and the stability of the prosthesis.5–7 The importance of accurate acetabular component alignment in THA cannot be overstated, as deviations can lead to major clinical complications, including increased dislocation rates, pelvic osteolysis and cup migration, ultimately shortening the lifespan of the prosthesis or requiring revision surgery.5–9 Recent advancements in surgical technology have increased the ability of surgeons to achieve accurate component alignment in THA.
The Direct Anterior Approach (DAA) for total hip arthroplasty has gained popularity supported by advancements in surgical instruments and specialized operating tables. Advocates of DAA highlight its benefits, such as less muscle damage and reduced pain,10,11 while the incorporation of fluoroscopy has improved the accuracy of component placement.12,13 However, the use of fluoroscopy increases radiation exposure to both patients and surgeons14,15 and presents a lengthy learning curve for practitioners.3,12,14 There is also a potential increased risk of contamination associated with the use of the fluoroscopic arm. 16
In contrast, Robotic-assisted Total Hip Arthroplasty (RA THA) uses pre-operative CT scans to create precise 3-D models for aligning bone cuts, eliminating the need for intra-operative fluoroscopy. RA THA has shown greater accuracy in component positioning compared to a manual posterior approach.17–19 yet, it is limited by its high costs, restricting its use to primarily high-volume centers. Drawbacks also include the necessity for pre-operative CT scans, limited implant choice, increased operating times, and limited implant options. 20
A promising alternative is Computer-Navigated Total Hip Arthroplasty (CN THA). CN THA offers real-time feedback and guidance, potentially enhancing the accuracy of bone cuts and component placement. Research indicates that CN THA achieves more accurate cup positioning, is cost-effective, adds minimal operative time, and requires only slight modifications to surgical techniques.21–25 One example of CN THA technology is HipAlign® (OrthAlign Inc., Aliso Viejo, CA), an accelerometer-based, open implant device combining a reference sensor with a disposable computer display.
This study aimed to achieve two primary objectives. Firstly, it sought to evaluate the precision of CN THA in correcting leg length discrepancies and in accurately positioning the acetabular cup, as determined by inclination and anteversion angles. Secondly, the study aimed to assess the accuracy of CN THA in providing intra-operative measurements of leg length, inclination, and anteversion that correspond with those acquired from post-operative radiographs.
Methods
Subjects
Summary of cohort demographics.

Operative methods and materials
The surgeon utilized an anterior approach for each patient. Pre-operative templating was completed for all patients, including pre-operative leg length discrepancy measurements. The reference frame target inclination and anteversion angles were 40° and 15° respectively. All patients received the same Smith and Nephew (Memphis, Tennessee) acetabular and femoral components. The Hana® table (Mizuho Inc., Chiyoda City, Tokyo, Japan) was used during all DAA procedures. Fluoroscopy was used only to assess the fit of the femoral stem and overall offset.
For this procedure, HipAlign was utilized as per its standard operating guidelines.
26
The setup process entailed attaching the computer to the ipsilateral iliac wing using a base and two pins, positioned 2 cm and 4 cm behind the anterior superior iliac spine (ASIS) respectively. The system was then calibrated using key anatomical points: The Coronal Plane (CP) and the Anterior Pelvic Plane (APP). This calibration allowed the accelerometer-based navigation system to accurately determine the orientation of the pelvis and leg length (Figure 1). Intra-operative pictures highlighting registration of the APP (bilateral ASIS [A, B] and pubic symphysis [C] and acetabular component insertion [D]).
HipAlign is integrated with sensors that provide continuous updates on the positioning and alignment of the hip joint components during the operation. As the surgeon places the hip cup, real-time feedback is offered on both the inclination (the angle of the cup in relation to the body’s coronal plane) and the anteversion (the angle of the cup’s opening in relation to the axial plane). Figure 2 displays a typical HipAlign reading during surgery, along with a 3D representation of the Coronal and Anterior Pelvic Plane (APP) reference planes. The measurements of inclination, anteversion, and leg length obtained by HipAlign during the surgery were documented for each patient. These measurements represent the intra-operative data for each parameter in this study. HipAlign intraoperative display. Used with permission from HipAlign operating Manual.
26

Post-operative measurements
Post-operative pelvic radiographs, consisting of calibrated anterior-posterior images, were taken for each patient 6 weeks following surgery. Acetabular cup position and leg length were measured using TraumaCad® (BrainLab Inc., Westchester, Illinois), which is a validated technology that can measure cup position, using angular measurement tools on anteroposterior radiography. 27 The cup position (acetabular cup inclination angle and anteversion angle), and leg length discrepancy, were evaluated by two independent observers, both of whom were blinded to each other’s results.
For each image and software program, manual calibration was performed using a standard 25 mm scaling ball. Acetabular component position and leg length were measured using the inter-teardrop line to lesser trochanter method. Leg length measurements were defined as the perpendicular distance between the inter-teardrop line and the most prominent medial point of the lesser trochanter. Acetabular inclination was defined as the angle between the horizontal reference line and a line bisecting the center of the acetabular cup face through the medial and lateral apexes (i.e., along the major axis) of an oval overlaying the cup face. Acetabular anteversion was determined by measuring the angle between the minor axis of an ellipse around the acetabular component and the inter-teardrop line.
Comparisons
The accuracy of CN THA at obtaining leg length restoration was assessed using post-operative leg length measurements. These measurements were then compared to intra-operative measurements obtained using CN THA. The accuracy of CN THA at obtaining proper acetabular component positioning was evaluated against the target alignment goals of 40° and 15°. Lastly, post-operative acetabular component position measurements (inclination and anteversion angles) from TraumaCad were also compared with the intraoperative CN THA measurements. Measurement error was determined by calculating the discrepancy between TraumaCad and CN THA measurements across both parameters. Measurement error thresholds were selected in accordance with those outlined by Koldychuk et al. 28 Measurement errors within 5° or 5 mm were deemed non-outliers, errors exceeding 5° or 5 mm but less than 10° or 10 mm were classified as mild outliers, and errors surpassing 10° or 10 mm were categorized as significant outliers. These thresholds were based on their established use in prior clinical research28–30 and the clinically accepted tolerances for leg length discrepancies.31,32
Data analyses
Categorical variables were characterized using frequencies and percentages, and continuous variables were characterized using means and standard deviations. The accuracy of acetabular component positioning was evaluated using one-sample t-tests to compare the post-operative inclination and anteversion angles with target goals of 40° and 15°, respectively. Linear regression models were used to assess the association between intra-operative and post-operative anteversion and inclination. Because we anticipated that multiple patients would likely have the same intra-operative and post-operative angles, we used a jitter to add small amounts of random noise to each plot and avoid overplotting. Pearson correlation coefficients were used to compare the CN THA measurements to TraumaCad technology. Analyses were performed using R version 4.0.3.
Results
Summary of descriptive analysis examining leg length discrepancy, inclination, and anteversion, emphasizing precision in placement and measurement consistency. The table also includes Pearson Correlation Coefficients comparing intra-operative measurements of leg length, inclination, and anteversion with their corresponding post-operative radiographic values.
Evaluation of leg length discrepancy measurements, intra-operative, post-operative, and measurement error.

Evaluation of acetabular cup anteversion angle measurements, intra-operative, post-operative, and measurement error.

Evaluation of acetabular cup inclination angle measurements intra-operative, post-operative, and measurement error.

Discussion
This study set out to assess the ability of CN THA to perform two main aspects of THA, the restoration of leg length and proper acetabular component positioning. We looked at the accuracy of CN THA in accurately performing those tasks and assessed how accurately intra-operative CN THA measurements aligned with those taken from post-operative radiographs.
CN THA demonstrated a high degree of accuracy in correcting leg length discrepancies, with over 85% of cases less than 5 mm. The performance of CN-THA in this study was found to be superior to other studies investigating leg length restoration using DAA-F THA. A study by Austin et al. reported that only 59.6% of patients achieved a leg length offset of less than 5 mm. 33 These results are consistent with other research highlighting the advantages of computer-navigated leg length restoration compared to fluoroscopy.28,34 This suggests that CN THA may offer more precise leg length restoration and potentially outperform traditional THA methods in this regard.
Furthermore, when comparing the accuracy of intra-operative measurements taken with CN THA to post-operative leg length differences, CN THA proved to be highly precise, with 98.4% of CN THA measurements falling within 5 mm of their respective post-operative radiographic measurements. A study by Caus et al. explored the accuracy of intra-operative leg length measurements using fluoroscopy versus post-operative radiographs, revealing a mean difference of 2.17 mm. 35 In contrast, our study demonstrated that CN performed substantially better, showing a mean difference of only 1.03 mm in leg length measurements when compared to post-operative radiographs. The Pearson Correlation Coefficient of 0.80 indicates a very strong correlation between CN THA intra-operative measurements and post-operative radiographs. This high degree of association reinforces the notion that CN THA provides surgeons with a dependable indication of the actual leg length restoration achieved.
CN THA was shown to be highly precise in achieving target alignment: no inclination measurements were significant outliers (error ≥10°) from the 40° target, with only 9.0% as mild outliers (5° ≤ error <10°). For anteversion, there were 23.8% mild outliers and just 1.6% significant outliers. The two patients who were significant outliers had anatomic deficiencies in the acetabular wall. The surgeon did not want the acetabular component to be too prominent for fear of impingement on the surrounding soft tissue. A similarly conducted study using a handheld accelerometer-based CN THA found similar results, with 74% of anteversion and 90% of inclination angle measurements deemed non-outliers. 28 These results indicate that the use of CN THA for THA results in accurate and precise acetabular component positioning.
This study also assessed the ability of CN THA to consistently obtain intra-operative anteversion and inclination angle measurements that align with those taken post-operatively. We found a moderately strong correlation between intra-operative device measurements compared to post-operative radiographic measurements; Pearson correlation coefficient was 0.50 between intra-operative and post-operative anteversion measurements and 0.66 for inclination measurements. Descriptive analysis showed that 97.5% of intraoperative anteversion and inclination measurements using CN THA fell within 10° of the postoperative radiograph measurements, demonstrating extremely high accuracy in positional assessment of the acetabular component. These findings resemble those of Kolodychuk et al., where 95% of anteversion measurements and 100% of inclination measurements were within 10° of post-operative radiographic measurements. 28
Proper acetabular component alignment is essential for successful total hip arthroplasty and has been shown to prevent complications like joint dislocation, impingement, and accelerated wear.36–38 The target inclination and anteversion of 40° ± 10° and 15° ± 10° that were chosen for this study were consistent with prior literature.28,39,40 Lewinnek noted a significantly higher dislocation rate for implants outside the “safe-zone” of 40° ± 10° for inclination and 15° ± 10° for anteversion. 41 However, safe zone definitions vary, with alternatives like the Widmer, Callanan, and Dorr safe zones offering different alignment recommendations.42–44 Safe zones continue to evolve, with recent studies suggesting more nuanced ranges based on individual patient anatomy such as spino-pelvic relationships, femoral neck-shaft angle, and femoral anteversion.44–46
It is important to recognize that commonly accepted target zones for component positioning do not eliminate the risk of dislocation or impingement, particularly in patients with spino-pelvic imbalance. Abdel et al. reported that among 206 total hip arthroplasties that subsequently dislocated, 58% had acetabular components positioned within the traditional “safe zone” of 40° ± 10° of inclination and 15° ± 10° of anteversion. 48 These findings highlight that, although target alignments remain clinically useful, optimal component positioning must also account for patient-specific anatomic factors, including femoral anteversion, neck–shaft angle, and the spinopelvic relationship.44–46
Robotic-assisted total hip arthroplasty (RA-THA) addresses this limitation by enabling real-time incorporation of individualized anatomic variables into component positioning, albeit at increased cost and with reliance on preoperative CT imaging. More recently, computer-navigation technologies such as Lantern® Hip (OrthAlign Inc., Aliso Viejo, CA) have sought to bridge this gap by allowing intraoperative navigation to a functional pelvic plane, thereby facilitating patient-specific acetabular placement without the added cost or need for preoperative CT imaging. Further investigation is needed to determine the clinical effectiveness of these emerging technologies.
The limitations of this study must be acknowledged. The research was conducted with a specific cohort under the care of a single, fellowship-trained orthopedic surgeon, which may limit the generalizability of the findings. Furthermore, the absence of a control group and a comparison against other THA techniques or navigation systems limit the scope of our conclusions. Another limitation is the use of post-operative radiographs instead of computed tomography, which has been shown to be superior for measuring acetabular cup orientation, specifically anteversion. 47 Additionally, the study was constrained to the Direct Anterior Approach (DAA) and did not encompass long-term post-operative outcomes. The comparative effectiveness of CN THA against other hip alignment technologies remains an area for future exploration.
Conclusion
CN THA shows considerable potential in improving surgical precision with THA, particularly in correcting leg length discrepancy and achieving accurate positioning of the acetabular component. Additionally, this study provides strong evidence that the measurements obtained from CN THA are reliable and align with gold standard measurements, offering surgeons confidence that their intra-operative measurements are highly accurate – what you see is what you get. As the field of orthopaedics advances, the adoption of such sophisticated systems will be crucial in enhancing surgical results and customizing patient care.
Footnotes
Ethical considerations
The authors accessed only de-identified data, except for the senior author who provided surgical care and follow-up but did not participate in the data collection and analysis. Consequently, the project was determined not to require IRB oversight.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael Decker, M.D. receives research support from Arthrex and is a paid speaker for Aerobiotix. William Lutes, D.O. recieves royalties from OrthoAlign, is a paid speaker for OrthoAlign and Smith and Nephew, is a paid consultant for OrthoAlign and Smith and Nephew, and holds stock in OrthoAlign.
Declaration of generative AI and AI-assisted technologies in the writing process
Statement: During this work’s preparation, the authors used Chat-GPT to correct grammar and help make the manuscript more concise. After using Chat-GPT, the authors reviewed and edited the content as needed and took responsibility for the publication’s content.