
Abstract
Artificial intelligence (AI) has become pervasive in biomedicine and is transforming orthopaedic research from bench to bedside. Beyond its established roles in robotic surgery and diagnostics, AI now supports advances in biomechanics, imaging, tissue engineering, drug discovery, genomics, and prosthetic control. In biomechanics, AI enables faster finite-element simulations, markerless gait analysis, and data augmentation using synthetic signals. Imaging applications include automated segmentation of the spine and hip, opportunistic screening for osteoporosis, bone metastasis detection, and three-dimensional analysis of knee osteoarthritis. In regenerative medicine, AI assists in scaffold optimization, bioprinting, and personalized cell therapies, while integration with genomic and proteomic data enhances precision orthopaedics. Machine learning–based control systems also improve the usability of prosthetics and exoskeletons, reducing cognitive burden for patients. Despite challenges such as data scarcity, validation, and ethical considerations, AI is emerging as a powerful complement to traditional research methods. By accelerating workflows, improving accuracy, and enabling individualized care, AI holds strong potential to bridge laboratory discoveries with clinical applications in orthopaedics. This review highlights the application of AI in orthopaedic research and assesses how it could integrate into clinical practice in the future.
Introduction
Artificial intelligence (AI) has emerged as a transformative force across multiple disciplines, and orthopaedic surgery is no exception. Beyond its established roles in robotic surgery, diagnostic support, and treatment optimization, AI is now reshaping the landscape of preclinical and translational orthopaedic research, and tools to enhance diagnostic accuracy have been employed in clinical orthopaedics.
Traditional preclinical methods in orthopaedics are often time-consuming, resource-intensive, and limited in predictive power. AI has begun to bridge the gap by enhancing animal model analysis, biomarker discovery, drug and device development, and biomechanical simulation. 1 In particular, machine learning (ML) and deep learning (DL) techniques have facilitated more accurate interpretation of laboratory data, enabling faster translation of experimental findings into clinical applications. 1
In biomechanics and computational modelling, AI has helped through detailed simulations of the mechanics of prostheses and implants. 2 In tissue engineering and regenerative medicine, AI supported the scaffold design through the biological and mechanical properties for bone and cartilage regeneration performance. 3 AI has also enhanced drug discovery and its delivery systems in orthopaedic research and care. 4 Integration with genomic datasets is further paving the way for personalized medicine, tailoring treatments based on individual biological profiles. 5
This review highlights the expanding role of AI in advancing preclinical and translational orthopaedic research, focusing on its applications in imaging, biomechanical analysis, tissue engineering, and drug/device development.
AI-assisted imaging and analysis in preclinical orthopaedic research
AI in biomechanical analysis
AI and finite element analysis (FEA)
AI in biomechanical analysis - AI in finite element analysis (FEA).

AI in gait and movement analysis
AI in biomechanical analysis – AI in gait and movement detection.

Systematic reviews confirm that AI models outperform conventional methods in analyzing high-dimensional gait datasets. 9 Both studies, Lim et al. and Molavian et al., confirmed the diagnostic utility of AI in distinguishing pathological gait, particularly in neurological conditions like Parkinson’s disease, with high accuracy (>90%).9,10 From the sports applications, Tedesco et al. demonstrated that IMU-based ML models detected long-term gait alterations with ACL injury, even years after the initial trauma. 11
Aside from the diagnostic approach, Ben Chaabane et al. showed that advanced AI architectures (LSTM, CNN, ResNet, Vision Transformers) can forecast gait progression, supporting individualized treatment planning. 12 One of the main challenges in applying AI to gait research is the scarcity of data. To overcome this, Sharifi Renani and colleagues 13 developed synthetic IMU signals for model training, which significantly improved prediction accuracy, reducing errors by more than half at the hip and nearly as much at the knee. While these advances are promising, limitations remain. Much of the work so far has been carried out in controlled laboratory settings, making real-world validation necessary before clinical use. In addition, approaches such as unsupervised and transfer learning are still underutilized, even though they could enhance robustness in natural environments. Better integration of multimodal inputs—such as video, IMU, and EMG—would also provide a more comprehensive view of movement. Finally, ethical and privacy issues surrounding gait data must be carefully addressed before these technologies can be adopted more broadly.8,11
AI-assisted pre-clinical imaging
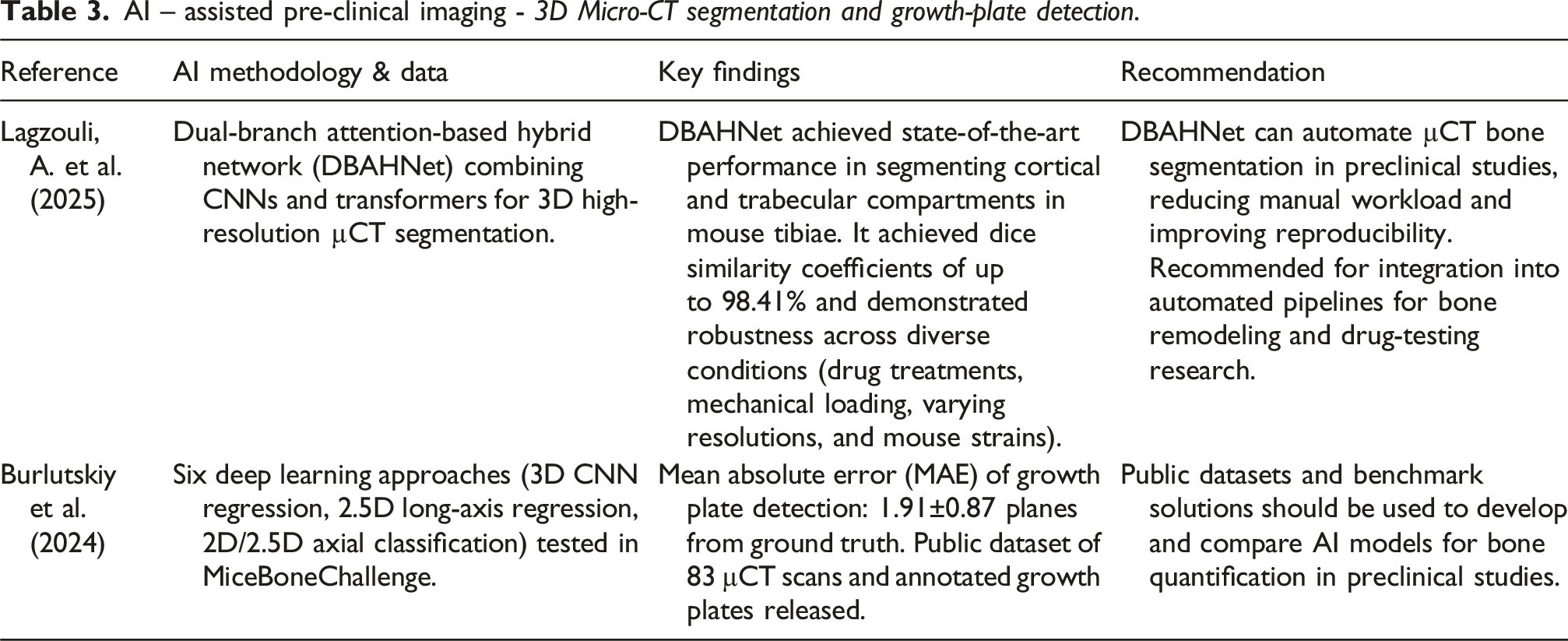
3D Micro-CT segmentation and growth-plate detection
AI – assisted pre-clinical imaging - 3D Micro-CT segmentation and growth-plate detection.
AI – Preclinical screening and disease modelling, assisted sports injury prediction
Machine learning based osteoporosis model
Machine learning based on an osteoporosis model.

Sport injury prediction
AI in sports injury prediction.

Besides ACL injury risk, muscle injury in soccer can be predicted by identifying hamstring strength and stiffness. In muscle-injury prediction, XGBoost classifiers applied to professional soccer players identified maximal hamstring force and tissue stiffness as top features, achieving ∼78% accuracy. 20 Importantly, this approach provided interpretable outputs, underscoring the need for explainability in clinical translation. However, a study by Amendolara et al. found that the current lack of open-source datasets and reliance on dated regression models produce inconclusive results regarding the efficacy of machine learning in predicting sports injuries. 22
AI can classify athletes into higher- and lower-injury-risk strata based on movement stability and load-absorption metrics. In youth basketball players, inertial-sensor features such as ellipse area and RMS acceleration during landing correlated with LESS scores, producing high accuracy (96%) with a linear SVM. 18
Tissue engineering and regenerative medicine
AI is slowly becoming an indispensable tool in orthopaedic research, where it can extract meaningful patterns and insights from large, heterogeneous datasets, thereby improving prediction and guiding experimental design. Applications include bone imaging analysis, surgical planning, and regenerative orthopaedics. For example, Fredrik Liu et al. developed a neural network model that integrated preclinical and clinical data to predict cartilage repair outcomes, achieving a cross-validated R2 = 0.637 ± 0.005 (p < 0.005). 23 The model identified that the defect depth, area, and implantation dose were essential predictors, with optimal MSC doses ranging between ∼17 and 25 million cells. Importantly, it also quantified uncertainty, providing confidence-based guidance for clinical translation.
Tissue engineering and regenerative medicine in orthopaedic research.
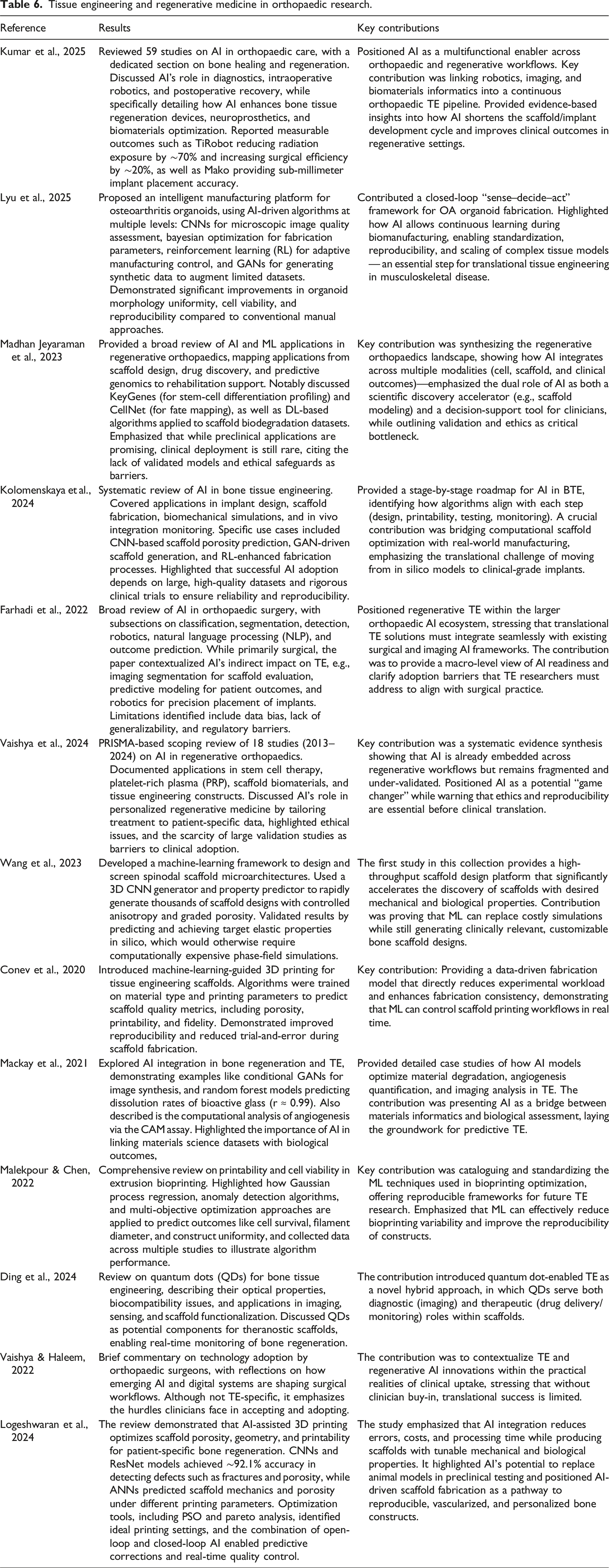
Other research described how AI can be integrated into scaffold design, CAD modelling, process monitoring, and biological evaluation.22,25,28 AI can also accelerate both the design and evaluation phases. A study by Fredrik Liu et al. quantified MSC dosage and its effects in depth, offering predictive insights for cell-based therapies. 29
AI also extends into intelligent manufacturing systems. Lyu et al. proposed AI-assisted production of osteoarthritis organoids, combining automation, predictive modelling, and quality control. 30 This framework aims to stabilize OA microenvironments in vitro, producing reproducible organoids that support drug testing and disease modeling 30
More recently, Logeshwaran et al. reviewed artificial intelligence-based 3D printing strategies for bone scaffold fabrication, demonstrating how AI can enhance scaffold porosity, topology, geometry, and printability to produce patient-specific constructs. 31 The study highlighted the use of convolutional neural networks (CNNs) and ResNet models for quality control, with the capability of detecting fractures, gas porosity, and lack of fusion with ∼92.1% accuracy. In contrast, artificial neural networks (ANNs) were employed to predict scaffold mechanical properties and porosity under varying printing parameters. Optimization methods, such as particle swarm optimization (PSO) and Pareto front analysis, were employed to identify ideal printing conditions. The combination of open-loop and closed-loop AI approaches enabled both pre-printing geometry programming and real-time corrective feedback. Importantly, the review emphasized the potential of AI-assisted 3D scaffolds to serve as alternatives to animal models in preclinical studies, thereby reducing ethical concerns while supporting translational applications. 31
Personalization of cell-based therapies
AI-driven network analysis has become a powerful tool for narrowing down candidate genes and pathways from high-throughput datasets. For example, Shi et al. integrated transcriptomic profiling with protein-protein interaction (PPI) networks in rheumatoid arthritis and identified hub genes such as LILRB1 and ATXN1, which subsequently guided structure-based drug screening. 32 In a similar approach, Huo et al. combined ferroptosis-related networks with differentially expressed genes (DEGs) in osteoporosis, uncovering 10 hub genes central to bone metabolism and iron handling. 33 These computational pipelines effectively condense thousands of genes into a focused set of candidates that can be directly leveraged for drug discovery and docking workflows.
Personalization has also emerged as a unifying theme across recent studies. Liu et al. demonstrated that AI can optimize mesenchymal stem cell (MSC) dosing, identifying optimal dose ranges, critical defect size thresholds, and case-specific confidence measures. 29 Such predictive models reduce empirical trial-and-error and enable patient-tailored regenerative medicine. More broadly, reviews emphasize the importance of embedding personalization into imaging, risk stratification, and therapy planning in orthopaedics. Underscoring AI’s role in advancing precision medicine21,23,24
Drug discovery and delivery
Drug discovery and delivery in orthopaedic research.
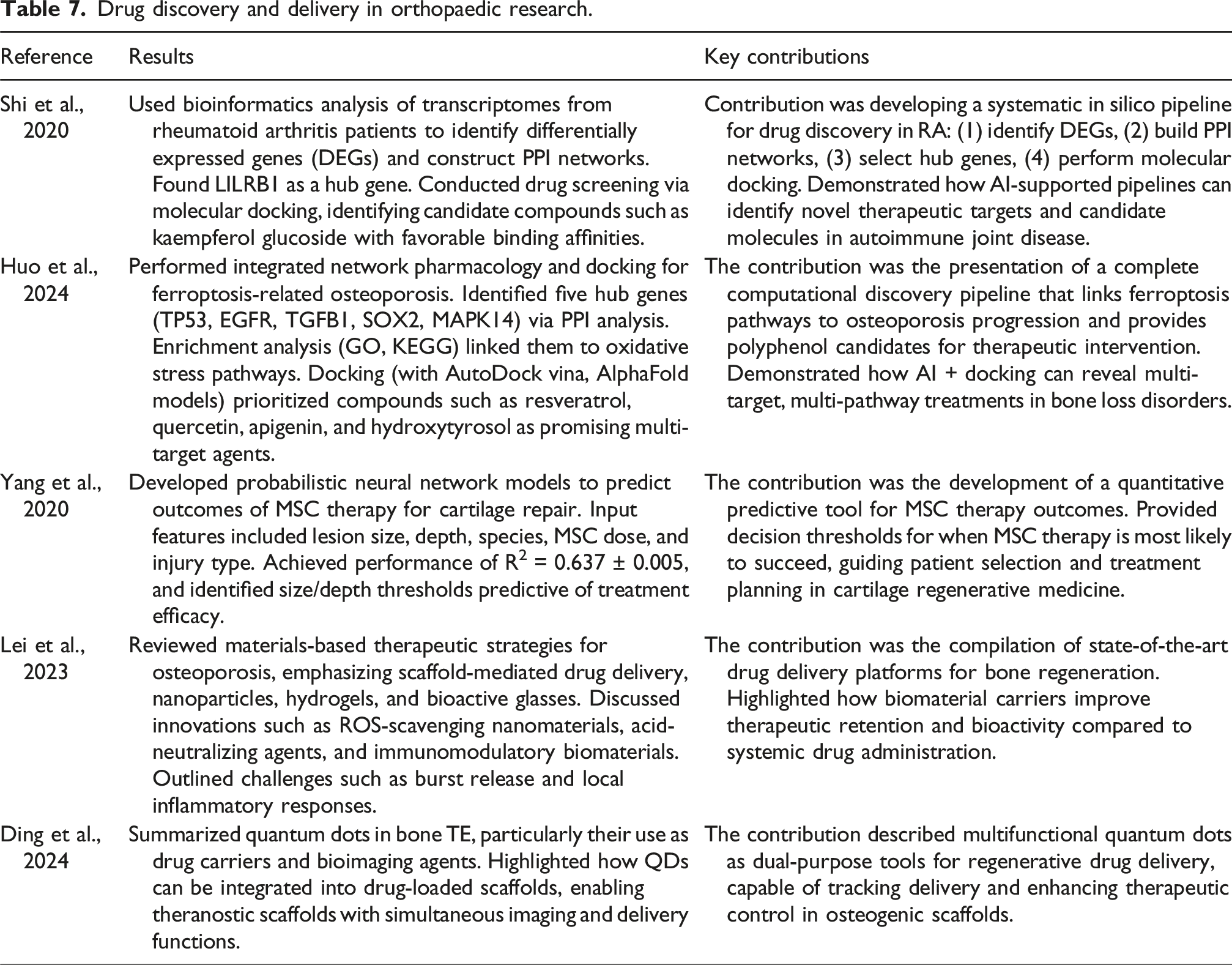
Complementary to molecular docking, materials-based platforms extend drug discovery into the realm of delivery. Based on the research of Lei et al., reviewed biomaterials, such as hydrogels, nanocarriers, and scaffolds, that help in more targeted and sustained delivery of osteoanabolic and osteoimmunomodulatory agents. 34 Whereas research done by Ding et al. described Quantum Dots (QDs) as a theragnostic tool, that enables or allows the combination of drug delivery with imaging and osteogenesis-enhancing functions. Although it was mentioned that biocompatibility and toxicity remain critical challenges that need further research and testing, 35 This continuum highlights how AI connects drug discovery with translational strategies in orthopaedics.
Genomics and precision orthopaedics
Genomics and precision orthopaedics.

Aside from genomics, proteomics offers real-time insights into disease by revealing the dynamic functional states of tissues. By using new biomarker panels and identifying disrupted pathways across various biological samples, proteomics complements structural data derived from both genetic and imaging analyses. It enhances understanding of disease mechanisms, stratifies patient risk, monitors recovery, and predicts treatment response. 37 The omics can be discovered from single-cell RNA sequencing (scRNA-seq), a powerful tool for investigating cellular diversity and mechanisms underlying orthopaedic diseases. This advancement could lead to the development of novel therapeutic targets, supporting precision orthopaedic practices. 38
The PRECISE STUDY by McKinley et al., 39 is a leading example of comprehensive data integration. Their “precision injury signature” concept, developed innovatively, created a multidimensional profile for patients with multiple injuries by analysing data on mechanical damage, blood flow dynamics, immunological responses, and demographics. Furthermore, understanding molecular interactions at the genomic level facilitates the design of effective bioactive scaffolds, particularly in the construction of implants and joint reconstruction. 40
Artificial intelligence enables more effective analysis of GWAS data, offering new avenues for uncovering genetic insights. These insights enhanced the identification of genetic risks and facilitated the prediction of susceptible diseases based on phenotypic expression. 41 Additionally, these genetic insights are also helping the development of targeted therapies. For instance, gene-editing techniques enable direct modification of genetic sequences associated with OA pathology.42,43 Metagenomic sequencing can also analyse the pathogens of bone and joint infections. A study by Maimati et al. 40 demonstrated 16S rRNA sequencing has a high concordance rate (87.5%) with bacterial cultures in detecting pathogens. This approach also recognised overlapping genetic pathways, for example, sarcopenia and osteoporosis both contribute to an increased risk of disability. 44
AI and prosthetic limb control
Lower limb prosthetics and exoskeletons have evolved from passive mechanical devices to powered, microprocessor-controlled systems. 45 Despite technological advances, intuitive and reliable user-device interaction remains a significant challenge, particularly in replicating natural volitional control.46,47 AI plays a vital role in replicating natural volitional control in prostheses and exoskeletons (Table 8).
Advanced machine learning techniques can analyze electromyography (EMG) signals and intuitively control the prosthetic device, thereby reducing the user’s cognitive burden. In a case series by Edwards et al., the application of General Value Functions (GVF) can predict a user’s intended next move in myoelectric upper-limb prostheses. The study demonstrated that predicting the user’s intended next move reduces the time and cognitive load required for amputees to operate their prosthetic device. 45 For lower limb prosthesis or exoskeleton, Cimolato et al. and Belal et al. conduct a systematic review evaluating machine learning processing to enhance the lower limb exoskeleton and prosthesis control.46,47 Cimolato et al. found that pattern recognition is the most prevalent approach for microprocessor-controlled lower limb prostheses (MLLPs). 46 The key findings from a study by Belal et al. on deep learning algorithms for lower limb exoskeletons included gait phase recognition, locomotion mode prediction, and torque/angle estimation. 47 CNNs, LSTM models, and reinforcement learning were most widely applied, demonstrating superior accuracy compared to traditional rule-based approaches. 47
From this literature, EMG remains essential for capturing user intent. However, hybrid systems integrating predictive algorithms and multimodal sensors hold tremendous promise for reliable, intuitive, and adaptive control.45–47
Synthetic data and virtual trials
AI and prosthetic limb control.

Gao et al. introduced SyntheX, a framework for generating realistic simulated images from human models. 49 This system enables the development of generalizable AI algorithms for X-ray image analysis. Their study compared models trained on realistically simulated data (Sim2Real) with those trained on SyntheX-generated synthetic data and found comparable performance. These results suggest that synthetic data from SyntheX can serve as a viable alternative—or complement—to real data acquisition. 49
Motion analysis and biomechanics are essential for comparing healthy and pathological individuals and assessing disease progression. However, human motion capture research is challenging because it requires considerable time commitments and significant financial resources. Thus, with the development of deep learning, generative AI can be employed to augment datasets by generating various synthetic biomechanical data. Perrone et al. (2025) applied a variational autoencoder with temporal modelling to generate synthetic kinematic and kinetic variables for motion analysis. 48 Both real data alone and a combination of real and synthetic data were used to train LSTM models. The performance of LSTM models trained on real data alone and on a combination of real and synthetic data is comparable, with normalised root mean square errors (nRMSE) on all four biomechanical outputs. 48
Sharifi Renani et al. (2021) further advanced this field by generating synthetic inertial measurement units (IMUs) to train recurrent neural networks for predicting 3D joint angles during gait. 13 Using a musculoskeletal modeling workflow in OpenSim, they augmented real IMU data with synthetic signals. Their results showed substantial improvements: prediction accuracy increased by 38% at the hip and 11% at the knee, while RMSE was reduced by 54% and 45% at the hip and knee, respectively. These findings highlight the potential of synthetic data to enhance predictive modeling where real data are limited. 13
Taken together, these studies demonstrate that synthetic data generation offers a powerful strategy to address data scarcity in orthopaedic research. Whether in imaging, motion analysis, or biomechanics, synthetic datasets can improve model robustness, reduce reliance on costly real-world data collection, and accelerate the development of AI-driven medical technologies. However, in data-scarce settings, synthetic data generation may lack the complexity of real-world variability and omit necessary factors.
Translational AI for orthopaedic diagnostics
Machine learning and deep learning
Machine Learning and Deep Learning are computer techniques that learn patterns from orthopaedic data like X-rays, CT/MRI scans, or clinical records to help clinicians spot problems sooner, measure them more consistently, and predict risks that matter for treatment and recovery. 53
Machine Learning uses algorithms that look at input features (for example, age, bone measurements, or image-based markers) to classify or predict outcomes.54,55 Deep Learning is a specialized type of Machine Learning that uses multi-layer neural networks to automatically learn patterns directly from raw images or signals, which is especially helpful for tasks such as detecting fractures, grading osteoarthritis, segmenting bones and joints, and recognizing implants or soft-tissue injury in complex 2D–3D imaging.53,56 In everyday practice, ML/DL can speed up image reading by auto-segmenting the spine or hip, flag likely bone metastases on CT, or screen for low bone density supporting faster decisions and more personalized care alongside clinician judgment. 57 Modern reporting checklist such as Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD + AI) for prediction models and Checklist for Artificial Intelligence in Medical Imaging (CLAIM) for medical-imaging AI explain what authors must disclose about data, model training, testing, and limitations so clinicians can trust what they read and reproduce it. Beyond headline accuracy, models should also report calibration because these determine safe decision thresholds and triage rules in clinical workflows.37,57
Synthetic data and Virtual trials in orthopaedic research.

Lumbar spine MRI
Hess et al. successfully applied machine learning to perform fully automated quantitative imaging from lumbar spine MRI data. In their study, convolutional neural networks (V-Net–style) were trained to segment vertebral bodies, intervertebral discs, and paraspinal muscles on routine sagittal and axial T1-weighted MRI scans. The AI-generated masks showed high agreement with human annotations, achieving segmentation Dice coefficients ≥0.77, and strong correlations for derived morphometric and biomechanical parameters (≥0.69 when significant). These findings suggest that AI-based segmentation could serve as a reliable substitute for manual annotations of major lumbar spine structures, with potential for integration into future clinical workflows 50
CT-scan for femoral neck anteversion (FNA)
Until recently, the assessment of femoral neck anteversion (FNA) has been limited by substantial intra- and inter-observer variability. Xiao et al. addressed this challenge by developing a fully automated FNA workflow based on deep learning. 51 Their model integrates femur segmentation, landmark identification, and anteversion calculation. Two-axis definitions were employed: Auto_GT, using the greater trochanter relative to the intercondylar notch center, and Auto_P, using the piriformis fossa relative to the intercondylar notch center. The deep learning approach achieved high measurement consistency, with intraobserver intraclass correlation coefficients (ICCs) ranging from 0.864 to 0.961. These results demonstrate that an automated, 3D CT–based method can provide reliable and highly reproducible FNA measurements, offering a robust alternative to conventional manual techniques.
Knee OA detection from MRI
Knee osteoarthritis (OA) is inherently a three-dimensional disease process, requiring volumetric imaging for early and accurate detection. Yeoh et al. addressed this challenge by adapting 2D convolutional neural network (CNN) weights to 3D, creating transfer-learning–assisted 3D CNN architectures (ResNet, DenseNet, VGG, AlexNet) trained on MRI data from the Osteoarthritis Initiative. 52 Across 13 tested architectures, transfer learning markedly enhanced performance, particularly in ResNet and DenseNet models. Among these, ResNet34 achieved the highest accuracy (0.875) and F1 score (0.871), while shallower networks such as ResNet18 and DenseNet121 reached AUCs of 0.945 and 0.914, respectively. These findings highlight the ability of 3D CNNs to capture the complex anatomical and structural features of the knee joint, supporting their potential use as computer-aided diagnostic tools for OA when volumetric MRI data are available. 52
Automatic detection and classification of bone metastases
Bone metastasis (BM) detection on CT scans is a time-consuming process, traditionally focused primarily on the spine. To address this limitation, a multi-institutional study developed an automated Bone Lesion Detection System (BLDS) trained on 2,518 CT scans encompassing 9,177 BMs from five hospitals. 53 The BLDS achieved 89.1% lesion-wise sensitivity at 1.40 false positives per case and delivered 92.3%/91.1% accuracy for BM versus non-BM classification in internal and external test sets, respectively. Integration with radiologist workflows improved lesion-wise sensitivity by 22.2% and reduced reading time by 26.4%. Real-world validation in 54,610 patients further confirmed strong performance, with 90.2% patient-level sensitivity and a 98.2% negative predictive value, underscoring its readiness for clinical deployment. 53
Opportunistic osteoporosis detection using LDCT
A 2025 study developed an opportunistic screening model for osteoporosis using low-dose abdominal CT. 54 he approach combined deep learning–based automatic segmentation of the proximal femur (VB-Net) with radiomics-based classification. Segmentation performance was excellent, with Dice similarity coefficients of 0.975 ± 0.012 (validation) and 0.955 ± 0.137 (test). For bone status classification, a random forest radiomics model achieved strong discrimination: AUCs of 0.924 for normal bone mass, 0.960 for osteoporosis, and 0.828 for osteopenia. Corresponding sensitivity and specificity values were high, with osteoporosis detection reaching 0.947 and 0.963, respectively. This framework demonstrates the potential of leveraging routine CT scans for radiation-free, cost-neutral, and opportunistic AI-based osteoporosis screening. 54
Hip fracture risk prediction with uncertain quantification
Shaik et al. developed a predictive model for hip fracture risk by integrating clinical variables with imaging features derived from hip dual-energy X-ray absorptiometry (DXA). CNN-extracted features included shape and texture measurements, which were incorporated into two ensemble models: Ensemble 1 (clinical variables only) and Ensemble 2 (clinical plus imaging features). Ensemble 2 demonstrated superior performance, achieving an AUC of 0.95, accuracy of 0.92, sensitivity of 0.81, and specificity of 0.94. Furthermore, a staged workflow with uncertainty quantification enabled approximately 54% of patients to be ruled out from requiring DXA scans, while maintaining high diagnostic accuracy. This approach highlights a cost-effective and patient-specific strategy for fracture risk prediction and screening optimization. 55
Common challenges, emerging trends, and consensus across studies
Across the studies included in this review, several recurring challenges and limitations emerge in the current application of AI in orthopaedic research. These include a limited dataset, a lack of standardized protocol, insufficient external validation, and substantial heterogeneity in evaluation metrics. Data scarcity and limited data variables affect research areas such as gait analysis, micro-CT imaging, regenerative modelling, and prosthetic limb control.12–15 Due to scarcity and limited data variables, many machine learning or deep learning models are trained on single-center or simulation-based datasets, leading to limited generalizability and increased risk of overfitting.12–14 Several studies also highlight the lack of a standardized protocol for AI development and evaluation in orthopaedic research. For instance, multiple gait analysis studies highlight a systemic lack of harmonized protocols for hardware configuration, sensor placement, gait task instructors, video acquisition settings, annotation methods, and preprocessing pipelines.7,10,11,13 Another major concern is the insufficient level of external validation in most imaging and biomechanical studies. Some AI models included in this review have not been deployed in the real world. Hence, limiting their translational ability. Moreover, reporting performance metrics such as AUC, RMSE, or Dice coefficient remains inconsistent across studies. Thus, underlining the importance of unified reporting frameworks such as TRIPOD-AI and CLAIM.56,57 Finally, interpretability represents a persistent challenge in deep learning models. The use of various algorithms with limited transparency may hamper clinical trust and regulatory approval; this issue is highlighted by the studies of Kolomenskaya et al. and Farhadi et al.22,23
Despite the challenges identified in AI orthopaedic research, several notable trends have emerged, including the use of synthetic data and generative modelling, a shift toward multimodal and integrative approaches, advancements in regenerative orthopaedics, and the development of real-time intelligent systems. Synthetic data and generative modelling have shown promising results, as demonstrated by synthetic IMU generation and syntheX.13,49 Both studies demonstrated that simulated data can meaningfully improve and reduce the prediction error of an AI model. By combining video, IMU, EMG results, radiomics, genomics, and proteomics, diagnostic precision and decision support in orthopaedics can be enhanced.8,11,36,37 In the field of regenerative orthopaedics, AI can aid in optimizing scaffold design, generate predictive models for mesenchymal stem cell therapy, and automate organoid fabrication. 24 Through predictive modelling, AI can also reinforce prosthetic and exoskeleton control. Machine learning, such as LSTM and reinforcement learning, helps translate user intent into more intuitive device behaviour.45,46 Collectively, AI in orthopaedic research does not replace conventional orthopaedic methods. Rather, it functions as a powerful tool that enhances accuracy, accelerates workflows, and promotes more integrated and individualized care. However, broader multicentre studies, consensus on regulatory framework, and integration strategies for safe and effective deployment must be implemented before clinical translation can be fully realized.
Research gaps and future research directions in AI-driven orthopaedics researches
Despite rapid advances, significant research gaps persist that limit the scalability and translational readiness of AI applications in orthopaedics research. Most notably, the lack of large, diverse, and multi-institutional datasets poses a major obstacle across imaging, gait biomechanics, prosthetic control, and tissue engineering.12–15 Many existing models are developed using controlled laboratory or simulation environments, resulting in limited external validity and uncertain real-world performance. The majority of studies also lack rigorous external validation, with only a small proportion evaluating models across independent populations or clinical settings, as highlighted by research on bone metastasis detection and opportunistic osteoporosis screening.53,54 In regenerative orthopaedics, translational pipelines are still fragmented, with limited continuity between in silico scaffold design, in vitro organoid modelling, in vivo validation, and clinical readiness. 24
For further advancement of AI in orthopaedic research, future studies should develop an organized multicenter data networks that facilitate collaborations while increasing the diversity and representativeness of training datasets. Harmonizing evaluation frameworks through systematic adoption of TRIPOD-AI, CLAIM, and ISO/IEC 23894 will be essential to ensure transparent reporting, robust calibration, and reliable external testing.56,57 Future research should also invest in trustworthy and interpretable AI, enabling clinicians to understand the AI model’s behaviour across imaging, biomechanics, and regenerative medicine, thereby supporting clinical acceptance and regulatory approval. Integrating multimodal data, including genomics and proteomics with gait, imaging, and biomechanics evaluation, may further enhance precision in orthopaedic research.8,11,36,37 Combining finite element modelling, multimodal sensor data, and patient profiles could enable more personalized implants and more accurate fracture-healing prediction.6,9,10 In regenerative medicine, progress will benefit from AI-driven scaffold design, automated organoid fabrication, and standardized preclinical validation frameworks.21–24,29 Finally, regulatory-ready AI will require ongoing research into fairness auditing, robustness testing under domain shift, lifecycle monitoring, and real-world post-deployment evaluation. Together, these directions outline a roadmap toward more reliable, explainable, and clinically impactful AI systems in orthopaedics.
Comparison of artificial intelligence models in orthopaedic research
Machine Learning (ML) and Deep Learning (DL) can serve as complementary or assist in orthopaedic research. Current ML algorithms, such as Decision Trees, Random Forests, Support Vector Machines, and Gradient Boosting, are considered important for certain research where datasets are structured or limited. These algorithms or methods are prized for transparency, lower computational demands, and robustness in situations with limited data.58,59
They require relatively low computational resources and provide transparent decision-making, which is valuable for applications such as biofabrication parameter optimization and clinical risk modelling. Conev et al. used Random Forest classifiers to predict print quality in 3D-printed scaffolds, enabling precise differentiation of optimal printing parameters and minimizing potential redundancies in experimentation. 26 Similarly, Malekpour and Chen combined experimental and ML algorithms to help in the assessment of printability and cell viability in extrusion-based bioprinting, which demonstrates the effectiveness of ML-assisted control in tissue engineering. 27 These studies highlight ML’s strengths in interpretable, parameter-driven, and data-limited applications.
Deep Learning (DL), which includes Convolutional Neural Networks (CNNs), Recurrent Neural Networks (RNNs), and transformer-based models, can automatically extract hierarchical features from unstructured data, enabling end-to-end learning from complex imaging or histological data without manual feature engineering. These DL approaches have achieved diagnostic accuracies ranging from 85% to 99% in orthopaedic applications, including fracture detection, implant recognition, and osteoarthritis grading. 60 Gao et al. developed the SyntheX framework, which trained DL models on synthetic X-ray datasets and reported equivalent or superior performance when compared to models trained on real clinical data for hip imaging and surgical tool detection. 49 Likewise, Paek et al. integrated DL-assisted image analysis into a bone-on-a-chip platform to evaluate the efficacy of an anti-SOST antibody. They reported achieving over 95% accuracy in β-catenin translocation patterns. 17 However, these performance advantages are not without disadvantages. It is reported that there are challenges when using said algorithms, which have higher computational requirements and limited interpretability, as DL models often function as “black boxes,” complicating their clinical translation and regulatory validation.17,60
Supervised learning, which relies on labeled datasets, remains the dominant paradigm in both ML and DL applications, consistently achieving high predictive accuracy in classification and regression tasks.17,49,59,61 It has been especially successful in orthopaedic applications involving image segmentation, motion tracking, and cellular-level imaging. By contrast, unsupervised learning discovers hidden structures and correlations in unlabeled data via clustering or dimensionality reduction (e.g., K-Means, PCA). Less utilized in orthopaedics due to a lack of standardized evaluation metrics, related domain studies suggest that unsupervised or self-supervised pretraining can achieve 15-30% performance improvements in data-limited conditions. 61 This suggests applicability for orthopaedic datasets where annotations may be rare or inconsistent.
While small datasets are a potential limitation to any machine learning technique, TL can practically adapt pre-trained models or synthetic data to orthopaedic imaging tasks.49,60 Medical imaging using TL has demonstrated near-perfect accuracy while reducing the need for data and computation. 60 Gao et al. have shown that TL in a synthetic data generation framework, called SyntheX, enables deep networks to generalize well from simulated to real radiographic data with accuracy comparable to that of models trained solely on real data. 49 By contrast, training from scratch offers a lot of flexibility in architecture but remains impractical in orthopaedics because of limited data availability and high computational costs.17,49,60
In summary, ML models are superior in terms of interpretability and efficiency with smaller, structured datasets, while DL models thrive with large, complex datasets. Supervised algorithms are known to achieve high accuracy in well-annotated or labelled data, whereas unsupervised or hybrid supervised-unsupervised algorithms offer flexibility for unlabelled data. TL algorithm model strikes a practical balance by improving accuracy and generalization in low-data contexts. These models (ML, DL, and TL) each have their own advantage and disadvantages, so future researcher must have have a clear idea of what type of data that is being used or interpreted and use the appropriate algorithm that suits the research that is being conducted and can not be blindly used to enhance accuracy, consistency, and translational results in orthopaedic studies.
Ethical, privacy, and regulatory considerations in translational orthopaedic AI
Despite rapid progress, translating AI into orthopaedic research and clinical workflows requires careful attention to data governance, patient privacy, algorithmic transparency, and regulatory compliance. Preclinical and clinical datasets often contain identifiable imaging, gait signatures, and genomic patterns, making privacy-preserving data handling essential. Regulatory frameworks such as HIPAA (U.S.) and GDPR (European Union) require secure processing, de-identification, and controlled sharing of patient data, while emerging global frameworks increasingly emphasize data minimization and traceability of model decision-making.
For medical AI software, multiple governing standards outline validation, risk management, and reporting expectations. In particular, the FDA’s Software as a Medical Device (SaMD) framework and the EU Artificial Intelligence Act (2024) classify clinical decision-support models as high-risk systems requiring external validation, post-deployment monitoring, and bias auditing.62,63 Professional organizations have published complementary methodological standards, including TRIPOD + AI for transparent reporting of prediction models and CLAIM for AI in medical imaging, both of which promote reproducibility, calibration reporting, and external testing.56,57 Additionally, ISO/IEC 23894:2023 and IEEE 7001/7003 provide governance principles for algorithmic fairness and human oversight. 64 Hence, multicentric studies and real-world data validation are needed to ensure the AI systems can be reliably translated into clinical settings.
Translational imaging.

Conclusion
Artificial intelligence is reshaping preclinical and translational orthopaedic research, with applications spanning biomechanics, imaging, tissue engineering, drug discovery, genomics, and prosthetic control. AI enhances efficiency, accuracy, and personalization—examples include automated imaging analysis, synthetic data generation, scaffold optimization, and fracture risk prediction. However, the methodological quality of the studies is limited, as many studies faced data scarcity, validation issues, and ethical concerns, thereby undermining the generalizability of the findings. The lack of standardized performance metrics highlights a gap in reproducibility and external validation in AI applications. While other challenges remain, the integration of multimodal data and advanced learning methods offers a path forward. Rather than replacing traditional methods, AI serves as a powerful complement, accelerating translation from laboratory research to patient-specific clinical care. AI is transforming orthopaedics by enhancing imaging, drug discovery, implant planning, and regenerative therapies in both preclinical and translational domains. The field is advancing rapidly, but clinical translation requires better validation, regulation, reproducibility, and explainability.
Footnotes
Authors Note
The following information is required for submission. Please note that failure to respond to these questions/statements will mean your submission will be returned. If you have nothing to declare in any of these categories then this should be stated.
ORCID iDs
Consent to participate
Studies on patients or volunteers require ethics committee approval and fully informed written consent which should be documented in the paper.
Authors must obtain written and signed consent to publish the case report from the patient (or, where applicable, the patient’s guardian or next of kin) prior to submission. We ask Authors to confirm as part of the submission process that such consent has been obtained, and the manuscript must include a statement to this effect in a consent section at the end of the manuscript, as follows:
“Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request”.
Patients have a right to privacy. Patients’ and volunteers’ names, initials, or hospital numbers should not be used. Images of patients or volunteers should not be used unless the information is essential for scientific purposes and explicit permission has been given as part of the consent. If such consent is made subject to any conditions, the Editor in Chief must be made aware of all such conditions.
Even where consent has been given, identifying details should be omitted if they are not essential. If identifying characteristics are altered to protect anonymity, such as in genetic pedigrees, authors should provide assurance that alterations do not distort scientific meaning and editors should so note.
Author contributions
Please specify the contribution of each author to the paper, e.g. study design, data collections, data analysis, writing, others, who have contributed in other ways should be listed as contributors.
• Study design: LAPP, IHD
• Data collections: SG, JAH, AAH
• Data analysis: SG, JAH, AAH
• Writing: JF, EK, SG, JAH, AAH
• Supervisor: LAPP, IHD, JF, EK
Funding
The authors declare no involvement of study sponsors regarding this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.