
Abstract
Introduction
First metatarsophalangeal (MTP) joint arthrodesis is the gold-standard treatment for end-stage arthritis and hallux deformities. Successful fusion is improved by achieving adequate compression across the joint. Traditional plating systems provide single-point compression, whereas the Arthrex MTP valgus plate is designed for double compression, potentially improving stability and union rates. This study aimed to confirm double compression and compare two anchoring methods: K-wire and olive tip guide wire (BB-tack).
Methods
Twelve cadaveric feet were randomised to plate fixation using either K-wire or BB-tack anchoring. Compression was measured with Tekscan sensors during three stages: after seating the first compression screw, after seating the second screw, and after reseating the second screw without the stabilising K-wire. Peak force and contact pressure were analysed using ANOVA and t-tests (α = 0.05).
Results
Both techniques achieved measurable compression after the first screw, which increased significantly with the second screw (mean pressure: 0.55–0.62 MPa; peak force: 18.3–22.2 N). Removing the stabilising K-wire before reseating reduced peak force but maintained comparable pressure. No significant differences were found between anchoring methods (p > 0.05).
Conclusion
The Arthrex MTP valgus plate achieves double compression, enhancing construct rigidity compared to single-compression systems. Further clinical studies are warranted to validate these biomechanical advantages.
Introduction
Arthrodesis of the first metatarsophalangeal (MTP) joint is widely regarded as the gold-standard surgical intervention for managing a range of forefoot pathologies, including end-stage arthritis, hallux valgus and hallux rigidus. 1 The procedure aims to eliminate pain and obtain a stable, automatically aligned hallux. Several different techniques and devices are used to achieve MTP joint fusion, including staples, Kirschner-wire (K-wire), crossed screws and various plate designs.2–4 While there is no consensus on a single superior method, plating techniques consistently demonstrate fewer complications, greater stability and more favourable biomechanical outcomes than other methods.1,5 A critical factor influencing the success of MTP joint fusion is the degree of compression across the fusion site, with increased compression improving joint stability and osseous union. Most plating systems provide single-point compression over the joint during the procedure, whereas more recent designs, such as the MTP valgus plate, are engineered to achieve double compression, applying compression force on both sides of the joint.6,7 This dual compression valgus plate approach may offer biomechanical advantages that further support successful fusion and improved patient outcomes.
The MTP valgus plate is designed to achieve an additional stage of compression during arthrodesis, potentially enhancing fusion outcomes. In theory, this is accomplished through a sequential fixation technique. Initially, the plate is anchored longitudinally to the metatarsal using either a K-wire or olive tip guide wire (BB-tack) through a purpose designed hole in the plate. The first compression screw is then inserted in the phalanx, drawing the two bones together, using the K-wire or BB-tack as a post to compress against. Just before seating the head of the second compression screw in the metatarsal, the K-wire or BB-tack is removed. The shaft of the second screw holds the initial compression, and the seating of the head results in a second compression force, thus “double compression”.
The aim of this study was twofold: first, to confirm that double compression is achieved using this novel plate design; and second, to compare the effectiveness of the anchoring methods (K-wires and BB-tack) in generating the highest level of final compression across the fusion site.
Methods
The study assessed the contact pressure and peak force of the MTP valgus plate (Therapeutic Goods [Medical Devices] Certificate No: MDSAP 619148) produced by Arthrex (Naples, Florida), following two different compression posts, K-wires (Figure 1(b)) and BB-tack (Figure 1(c)). Six pairs of cadaveric feet (12 feet) from the Surgical Skills Training Unit of Macquarie University were randomised to the two techniques. The Tekscan system was used to measure the contact forces and surface area across the joint.
8
Valgus metatarsophalangeal (MTP) plate configurations and fixation techniques.
Procedure
The standard MTP joint fusion procedure was followed, with some minor modifications to accommodate the Tekscan sensor.
The procedure was as follows: 1. A dorsal incision was made, followed by an orthogonal incision around the lateral aspect of the MTP joint to facilitate the Tekscan sensor insertion. 2. Preparation of the proximal side of the joint. A K-wire was inserted coaxially into the metatarsal (Figure 2(a)). A 22 mm concave reamer was used to expose the subchondral surface (Figure 2(b)), and the wire was removed. The 22 mm reamer was used on all specimens to minimise sensor creasing. 3. A K-wire was inserted coaxially into the proximal phalanx. A 22 mm convex reamer was then used to create the mating surface (Figure 2(c)), after which the K-wire was removed. 4. A stabilising K-wire was passed from distal to proximal through the medial aspect of the proximal phalanx to the metatarsal to maintain the joint position for plate fixation (Figure 2(d)). In the standard procedure, this wire passes through the joint centre; however, to allow for the Tekscan placement sensor, it was positioned at the lateral periphery. 5. A BB--tack was used to anchor the MTP valgus plate longitudinally to the metatarsal (Figure 3(a)). 6. A hole was drilled eccentrically in the phalanx adjacent to the distal bevelled edge of one plate hole for the first compression screw (Figure 3(b)). 7. The first compression screw is inserted (Figure 3(c)). Seating the screw head into the bevelled hole produced compression against the K-wire or BB-tack anchoring the plate (Figure 3(d)). Pressure values recorded prior to seating (baseline) were subtracted from those after seating (first compression). 8. With the K-wire//BB-tack still in place (Figure 4(a)), a hole was drilled eccentrically in the metatarsal adjacent to the proximal edge of the appropriate plate hole. The second compression screw is inserted (Figure 4(b)), and the K-wire/BB-tack was removed just before seating the screw head, enabling double compression. Baseline values were subtracted from post-seating values (second compression). 9. The second compression screw was backed out until its head cleared the plate, and the stabilising K-wire was removed (Figure 4(c)). 10. The second compression screw was then reseated (Figure 4(d)). Baseline values prior to reseating were subtracted from post-reseating values. Sequential preparation of the metatarsophalangeal (MTP) joint surfaces for arthrodesis. Application of the first compression screw and assessment of joint compression during metatarsophalangeal (MTP) fixation. Application of the second compression screw and assessment of joint compression during metatarsophalangeal (MTP) fixation.



Tekscan measurements
Six pressure measurements were recorded for each procedure to assess peak force and contact pressure: 1. Baseline before seating the first compression screw (Figure 3(c)). 2. After seating the first compression screw (Figure 3(d)). 3. Baseline before seating the second compression screw (Figure 4(a)). 4. After seating the second compression screw (Figure 4(b)). 5. Baseline after backing out the second compression screw and removing the stabilising K-wire (Figure 4(c)). This should be comparable to reading three. 6. After reseating the second compression screw without the stabilising K-wire (Figure 4(d)).
Pressure readings were captured as follows: 1. The first using High2 sensitivity (the highest level) for direct comparison of contact area and pressure. 2. In cases where sensor saturation had occurred, a second reading at a lower sensitivity level was captured and was used for peak load determination.
The Tekscan 6900 sensor was selected for its suitable footprint. The 6900 sensors have four individual sensors; only one of these was used at any time during testing. Baseline subtraction was performed to minimise background noise from inactive sensors. An example reading after seating the second compression screw is shown in Figure 5. Tekscan system output and sensor schematic used for joint compression analysis.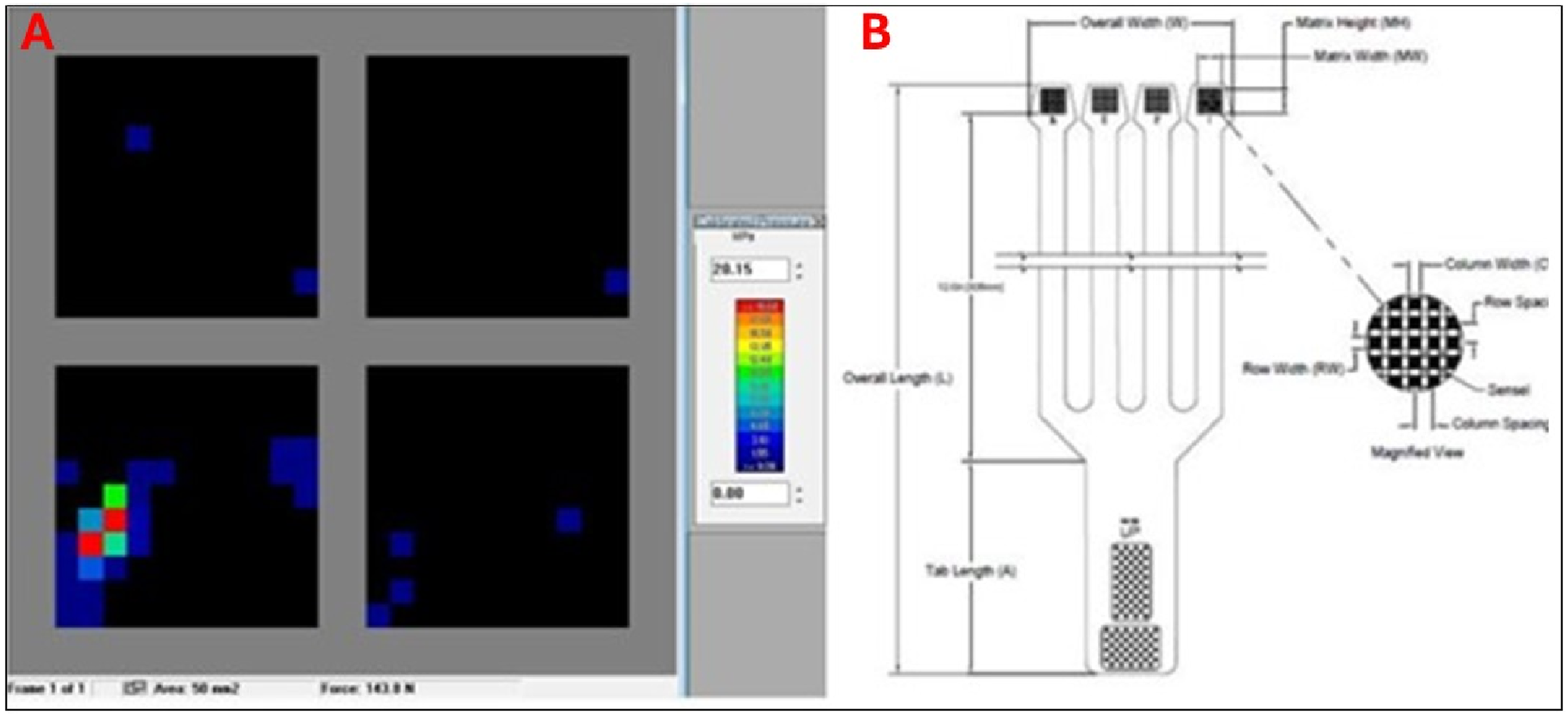
Calibration
Calibration was performed post-testing for each individual sensor used during testing. Each sensor was calibrated at all sensitivity levels used during testing. An Instron (E1000 ElectroPuls) machine was used to accurately capture three points for each calibration procedure as follows: 1. Initial detection of compression. 2. Moderate compression distributed across the sensor. 3. Onset of saturation.
These points were used to generate a calibration curve applied to the respective data.
Statistics
Data were analysed using SPSS (version 29). Normality was assessed using the Shapiro-Wilk test, and homogeneity of variations was verified with Levene’s test.
A one-way ANOVA was performed to compare contact pressure and peak force across three stages: (i) seating of the first compression screw; (ii) seating of the second compression screw; and (iii) seating of the second compression screw without the stabilising K-wire. Analyses were conducted separately for the BB-tack and K-wire groups. Where ANOVA indicated significance, post hoc Tukey tests were applied. Additionally, independent-samples t-tests compared BB-tack and K-wire groups at each stage. Statistical significance was set at α = 0.05.
Results
Summary of contact pressure and peak force across stages for BB-tack and K-wire groups.

Values are Mean ± SD.
Contact pressures
Figure 6(a) illustrates scaled contact pressures following seating of the first compression screw, the second compression screw, and reseating of the second compression screw after removal of the stabilising K-wire. Each measurement was referenced to its own respective baseline. Comparative analysis of joint compression metrics during metatarsophalangeal (MTP) fusion.
These results demonstrate that the insertion of the first screw produces measurable compression, which increases further with the insertion of the second compression screw. Comparable pressure was achieved when the stabilising K-wire was removed prior to seating the second compression screw.
Peak forces
Figure 6(b) shows peak forces recorded at the contact surface. These results indicate that the peak force rises with the first and second compression screws but declines when the stabilising K-wire is removed before seating the second screw.
Figure 6(c) highlights variability among specimens for both anchoring methods across all stages.
Discussion
This study demonstrated that the Arthrex MTP valgus plate achieves double compression across the MTP joint, which theoretically increases construct rigidity and may reduce non-union rates, leading to improved surgical outcomes. By anchoring the plate to the metatarsal during the placement of the first compression screw in the phalanx, greater total compression can be achieved across the joint. This dual compression mechanism represents an innovation in plate design, potentially offering superior compression compared to existing constructs.
Previous techniques for MTP joint fusion have included transarticular screws, non-locking plates and single-compression locking plates. However, to our knowledge, no prior study has described a plate system capable of two distinct compression events.6,7 This feature may address a well-recognised challenge in MTP joint arthrodesis, namely maintaining compression during fixation. 6 Alternative approaches, such as continuous compression devices, have recently been explored to improve fusion rates, 9 but these differ fundamentally from the dual compression concept evaluated here.
Our results also highlighted variability in compression and peak force values, as reflected by large standard deviations and inconsistent individual outcomes (Figure 6). This variability suggests that construct stability remains a concern, particularly when the stabilising K-wire is removed prior to seating the second screw; maintaining compression across the joint during fixation is a known issue during MTPJ fusion. Although the average compression was similar whether the K-wire was retained or removed, the inconsistency indicates that leaving the K-wire in situ may provide additional stability. The choice between BB-tack and K-wire anchoring remains at the surgeon’s discretion, with the K-wire potentially offering bicortical purchase, while the BB-tack may enhance plate-to-bone contact.
The strengths of this study include confirmation that the valgus plate design can deliver two distinct compression events across the first MTP joint, which has not previously been reported. Our results also provide clear biomechanical evidence that this approach offers greater rigidity than traditional single-compression plates.
Limitations
The first potential limitation of the study was that the placement of the Tekscan sensor required modifications to the standard surgical technique, including peripheral positioning of the stabilising wire and extensive soft tissue dissection. These changes might have reduced joint stability and altered load distribution, concentrating forces beneath the plate rather than across the entire fusion surface. 10 The second potential limitation was that Tekscan sensors have known limitations in accuracy and reliability, particularly under high loads and complex geometries.11,12 Future studies should consider custom sensors designed for joint contours and improved calibration protocols.
Despite these potential limitations, the current findings provide valuable comparative data and confirm that double compression occurs with this plate design. Future research should include biomechanical testing under cyclic loading, evaluation of fatigue resistance, and clinical studies assessing union rates and functional outcomes. Additionally, exploring hybrid fixation strategies and dynamic compression systems may further optimise stability and reduce non-union risk. 13
Conclusion
The Arthrex MTP valgus plate achieves double compression across the first MTP joint, offering greater compression than traditional plating methods. This design innovation may enhance construct rigidity and improve fusion outcomes. Further clinical studies are warranted to validate these biomechanical advantages and assess their impact on non-union rates and patient-reported outcomes.
Clinical relevance
Double compression achieved by the Arthrex MTP valgus plate represents a significant advancement in first MTPJ arthrodesis. Increased compression across the fusion site may enhance construct rigidity, reduce micromotion, and lower non-union rates, which are critical factors for improving patient outcomes. Surgeons should consider this technique when addressing cases with high risk of non-union or poor bone quality. Further clinical trials are needed to validate these biomechanical advantages and determine their impact on postoperative function and patient satisfaction.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Pepper has a consultancy agreement with Arthrex.