
Abstract
Purpose
To compare the clinical and radiological results of two double-bundle (DB) anterior cruciate ligament reconstruction (ACLR) techniques. DB ACLR and anterolateral ligament reconstruction (ALLR) with internal brace (IB), and outside-in (OI) DB ACLR.
Hypothesis
We hypothesized that DB ACLR and ALLR with IB wound yield less femoral tunnel, especially femoral posterolateral bundle tunnel complications, than OI DB ACLR without ALLR because of better rotational control. Both techniques could provide good postoperative clinical outcomes.
Methods
Patients who received DB ACLR and ALLR (ALLR group) and who received outside-in DB ACLR (non-ALLR group) were enrolled. Age, BMI, follow-up duration, meniscus repair, laterality, and knee range of motion (ROM) were collected. Lysholm, Tegner scale, and radiological results were compared.
Results
Thirty-four and 33 patients were enrolled in the ALLR and non-ALLR groups. Patient demographics were similar between groups. Both groups showed postoperative improvements in Lysholm (ALLR group, 62.5 ± 6.8 preoperatively and 85.1 ± 5.7 postoperatively (p < 0.01); non-ALLR group, 63.5 ± 6.0 preoperatively and 82.9 ± 5.2 postoperatively (p < 0.01)) and Tegner Scale (ALLR group, 4.97 ± 0.52 preoperatively and 7.79 ± 0.41 postoperatively (p < 0.01); non-ALLR group, 4.91 ± 0.58 preoperatively and 7.7 ± 0.47 postoperatively (p < 0.01)) at final follow-up. There were no significant differences between groups preoperatively (Lysholm, p = 0.324, Tegner, p = 0.649) and postoperatively (Lysholm, p = 0.679, Tegner, p = 0.369). The ALLR group exhibited significantly lower percentages of femoral posterolateral bundle tunnel widening (p = 0.021) and a more femoral divergent angle (p < 0.001) than the non-ALLR group. Furthermore, no femoral tunnel coalescence was observed in the ALLR group, while 3% of the non-ALLR group showed coalescence.
Conclusions
DB ACLR with ALLR yielded less femoral posterolateral bundle tunnel widening, no femoral tunnel coalescence, and more femoral divergent angle than OI DB ACLR. Both techniques provided good postoperative outcomes. Incorporating ALLR and IB may benefit patients undergoing DB ACLR.
Level of evidence
Level III, Retrospective comparative therapeutic trial.
Clinical relevance
DB ACLR with ALLR and IB provides less femoral PL tunnel widening, no femoral tunnel coalescence, and more divergent angles between the two femoral tunnels compared with traditional OI DB ACLR. DB ACLR with ALLR and IB technique provides more flexibility during femoral tunnel preparation.
Introduction
Anatomic double-bundle (DB) anterior cruciate ligament reconstruction (ACLR) provides better biomechanical joint function and stability than single-bundle (SB) ACLR. 1 One possible reason is that the DB ACLR provides more footprint coverage and recreates the two functional anteromedial bundle (AMB) and posterolateral bundles (PLB).2,3 Anterolateral ligament (ALL) has a synergistic function with ACL toward knee rotational stability.4–6 Additional augmentation or reconstruction to ALL has shown a significant reduction of the level of persistent pivot shift without increasing the long-term risk of osteoarthritis.7,8 Besides DB ACLR, FiberTape augmentation as an internal brace (IB) has been proposed to be used along with ACLR.9,10 It protects the newly reconstructed ligament during rehabilitation. 11 ACLR with hamstring autograft and independent suture tape reinforcement provides low rates of complications, graft failure, and reoperations with similar function, and return-to-sport rates when compared with hamstring autograft ACLR without suture tape reinforcement. 12
Postoperative tunnel widening is a phenomenon widely reported with the use of soft-tissue grafts for ACLR. 13 Although the enlargement in the tunnel area, diameter, or shape does not influence the clinical results, 14 the widened tunnel filled with fibrous tissue can be difficult to treat in cases of revision surgery. 13 Large tunnels may compromise graft fixation during revision surgery and may lead to two-stage surgery. 15
This study aimed to compare the clinical and radiological results of two DB ACLR techniques. DB ACLR and ALLR with IB, and outside-in (OI) DB ACLR. We hypothesized that DB ACLR and ALLR with IB wound yield less femoral tunnel, especially femoral posterolateral bundle tunnel complications, than OI DB ACLR without ALLR because of better rotational control. Both techniques could provide good postoperative clinical outcomes.
Material and methods
Patients
This study was approved by the ethics committee of our institution, and informed consent was obtained. Patients who underwent primary DB ACLR between January 2011 and July 2019 were enrolled in this retrospective, single-center, comparative cohort study. All procedures were performed by the same surgeon. The indications for DB ACLR were patients who had a grade 2 pivot shift or greater, athletes participating in pivoting contact sports, and side-to-side difference >10 mm. Patients who underwent DB ACLR and ALLR with IB were assigned to the ALLR group. Patients who underwent OI-DB ACLR only were assigned to the non-ALLR group.
Surgical techniques
OI DB ACLR (non-ALLR group)
Autologous hamstring tendons were harvested and prepared as two double-strand grafts. The double-semitendinosus tendon functioned as an anteromedial (AM) bundle, whereas the double-gracilis tendon acted as a posterolateral (PL) bundle. After the center of the AM and PL femoral footprints were marked by a microfracture awl (Figure 1(a)), two femoral guide pins were introduced intra-articularly in an OI manner (Figure 1(b)). Two guide pins were subsequently inserted into the bases of the AM/PL tibial insertion sites (Figure 1(c)). Femoral and tibial AM and PL tunnels were created using OI drilling (Figure 1(d)). Totally, two femoral and two tibial tunnels were created for the double-semitendinosus tendon and double-gracilis tendon graft to pass through. Two Ethibond sutures were passed from the tibial AM/PL bundle to the femoral AM/PL bundles and were used for graft shuttling (Figure 1(e)). After the introduction of the double semitendinosus and gracilis grafts intra-articularly, two bioabsorbable interference screws (Biosure-HA screws; Smith & Nephew, Andover, MA, USA) were used for femoral fixation in an OI manner, and another two interference screws were used for tibial fixation. The final construct is shown in Figure 1(f). Surgical techniques of OI DB ACLR for the right knee. (a) Anterolateral portal view of the right knee. Center of AMB (arrow) and PLB (arrowhead) femoral footprint were marked by a microfracture awl. (b) Two femoral guide pins were introduced intra-articularly in an OI manner, aiming at the center of AMB (arrow) and PLB footprint (arrowhead). Dashed line, lateral intercondylar ridge; dotted line, lateral bifurcate ridge. (c) Two guide pins were inserted into the bases of AMB (arrow) and PLB (arrowhead) tibial insertion sites. (d) The femoral AMB (arrow) and PLB (arrowhead) tunnels were created by OI drilling. A bone bridge at least 2.0 mm in length between both tunnels was created to prevent tunnel coalescence. (e) Two Ethibond sutures were passed from the tibial AMB/PLB tunnels to femoral AMB (arrow)/PLB (arrowhead) tunnels and worked for graft shuttling. (f) The final construct of DB OI ACLR. ACLR, anterior cruciate ligament reconstruction; AMB, anteromedial bundle; DB, double-bundle; OI, outside-in; and PLB, posterolateral bundle.
DB ACLR and ALLR (ALLR group)
This technique was performed according to a previous study.
16
The autologous semitendinosus was prepared in a triple-folded fashion as an AM bundle, as previously described. A single gracilis in full length along with FiberTape (from one Biocomposite Swivelock C anchor, Arthrex, Naples, FL) worked as the PL bundle intra-articularly and ALL extra-articularly. The femoral AM tunnel was prepared using a Clancy curved drill guide (Smith & Nephew, Andover, MA, USA) in an inside-out (IO) manner (Figure 2(a)), while the PL tunnel was drilled in an OI manner (Figure 2(b)). This technique ensured that the femoral AM and PL tunnels were positioned differently from each other (Figure 2(c)). One tibial ACL tunnel was subsequently created in the center of the ACL tibial insertion, and one tibial ALL tunnel was made posteriorly and proximally to Gerdy’s tubercle. The AM bundle graft (triple semitendinosus) was fixed using a suspensory fixation device (EndoButton; Smith & Nephew, Andover, MA, USA) on the femoral cortex (Figure 2(d)), and an interference screw at the tibial site was also fixed. The PL bundle graft (single gracilis and FiberTape) was fixed by an interference screw at the femoral side in an OI manner, and the same interference screw was fixed with the AM bundle in the same tibial tunnel. Finally, the single gracilis and FiberTape were shuttled from the lateral end of the femoral PL tunnel underneath the iliotibial band to the lateral end of the tibial ALL tunnel as the ALLR (Figure 2(e)). It was subsequently shuttled through the tibial ALL tunnel from the lateral to the medial side of the tibia, ensuring that both the gracilis and FiberTape were inside the ALL tibial tunnel. All sutures were thereafter tied and fixed intraosseously using a Swivelock C anchor. Totally, two femoral and one shared tibial tunnel were created. Triple semitendinosus and single gracilis with FiberTape were passed through the same shared tibial tunnel. Then, the triple semitendinosus was shuttled through the femoral AM tunnel, while the single gracilis with FiberTape was shuttled through the femoral PL tunnel. The final construct is shown in Figure 2(f). Surgical techniques of DB ACL and ALLR with IB for left knee. (a) Anterolateral portal view of the left knee. The femoral AMB tunnel (arrow) was prepared by a Clancy curved drill guide in an IO manner. (b) The PLB tunnel (arrowhead) was drilled in an OI manner. Dashed line, lateral intercondylar ridge; and dotted line, lateral bifurcate ridge. (c) The femoral AMB (arrow) and PLB (arrowhead) tunnels were divergent to each other. (d) The AMB graft (triple semitendinosus) was fixed by an EndoButton (arrow) at the femoral side. (e) The single gracilis (arrow) and FiberTape (arrowhead) were shuttled from the lateral end of the femoral PL tunnel, underneath the iliotibial band, to the lateral end of the tibial ALL tunnel as the ALLR. (f) The final construct of DB ACL and ALLR with IB for left knee. ACLR, anterior cruciate ligament reconstruction; ALLR: anterolateral ligament reconstruction; AMB: anteromedial bundle; DB: double-bundle; IB: internal brace; IO: inside-out; OI: outside-in; and PLB: posterolateral bundle.
Radiographic evaluation
Bone tunnel width and enlargement
Bone tunnels of the knee were measured using plain radiographs in the anteroposterior (AP) and lateral view at 0-month and 2-year postoperatively by the first author, who interviewed the patients before surgery and at the final follow-up. We only measured the femoral tunnel in the AP view because of difficulties in identifying both tunnels in the lateral view. We utilized Baumfeld’s method to measure the width of the femoral tunnel,
2
which calculated the width at 1 cm from the aperture of the femoral tunnels in the joint, and the measurements were made perpendicular to the long axis of the tunnels (Figure 3). Femoral bone tunnel width measurement by plain radiographs. Baumfeld’s method was used to measure the width of the femoral tunnel, calculated as the width at 1 cm from the aperture of the femoral tunnels in the joint. Measurements were made perpendicular to the long axis of the tunnels.
17
Anteroposterior view of the left knee. AM: anteromedial; PL: posterolateral.
Tunnel coalescence
Femoral tunnel coalescence was defined as the absence of a bony bridge between the AM and PL tunnels 1 cm from the aperture of the femoral tunnels in AP view (Figure 4). Tunnel coalescence of the left knee. Femoral tunnel coalescence was defined as the absence of a bony bridge between the AM and PL tunnels at 1 cm (arrowhead) from the aperture of femoral tunnels in AP view. AM: anteromedial; PL: posterolateral.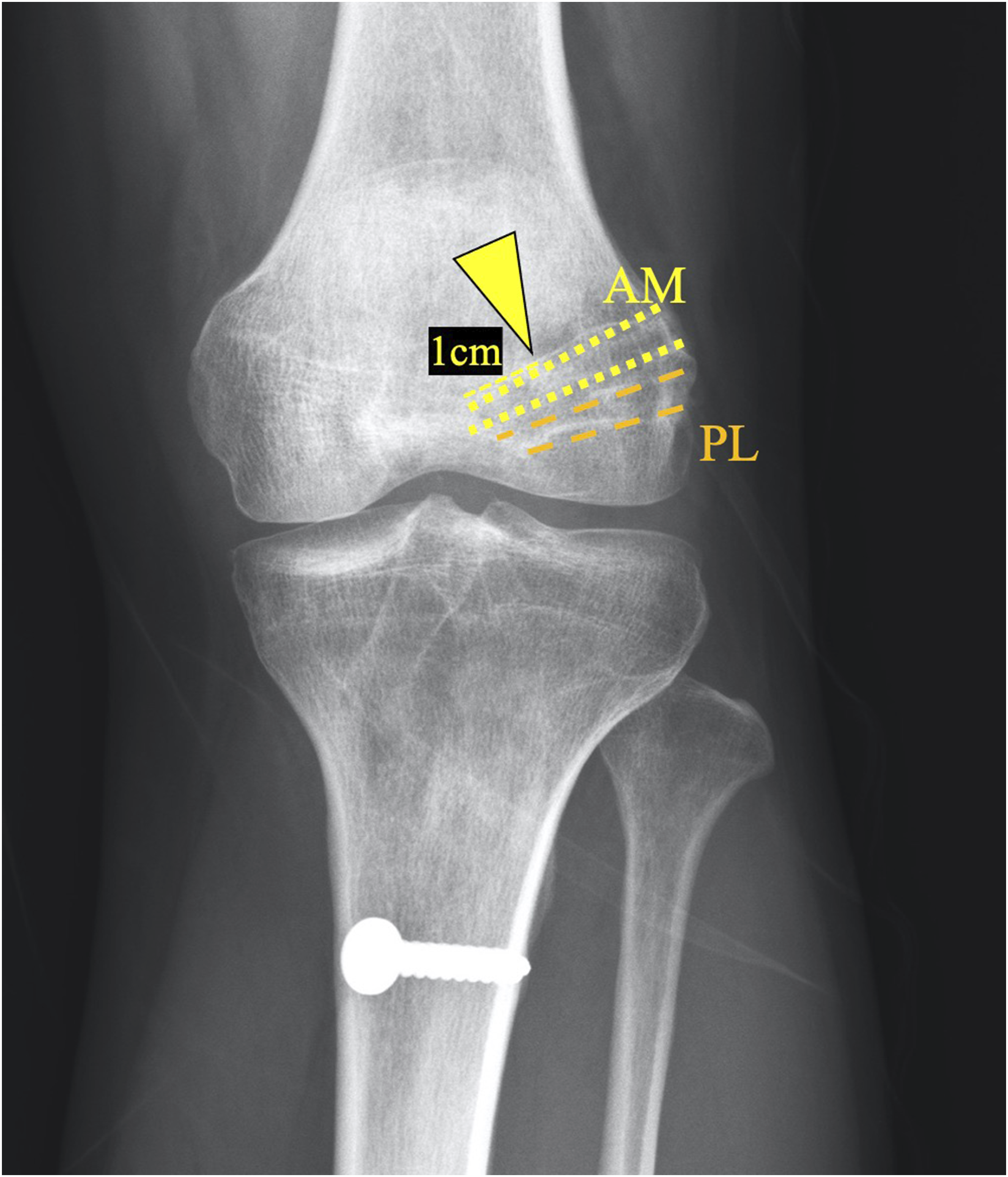
Femoral divergent angle
The divergent angle was defined as the included angle between the two lines formed by the axis of the femoral AM and PL tunnels in AP view (Figure 5). Femoral divergent angle of the right knee. (a) ALLR group. (b) Non-ALLR group. AM: anteromedial; DA: divergent angle; PL: posterolateral.
Rehabilitation
Patients in both groups received a brace-free mobilization, and tolerated full weight-bearing, and progressive ROM exercise immediately after the surgery. A gradual return to sports activities was allowed starting at 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8–9 months for pivoting contact sports, 18 regardless of the meniscal treatment intraoperatively.
Clinical evaluation
Clinical evaluations were performed preoperatively and at 2 years postoperatively using Lysholm, 19 and Tegner Activity Scale. 20 Knee ROM data were collected preoperatively, and 2 years postoperatively by an independent orthopedic doctor blinded to the type of surgery and rehabilitation. Radiographs were obtained at 0-month (postoperatively) and 2-year postoperatively to quantify the bone tunnel diameter and evaluated by a radiologist with >10 years of experience.
PICO of this study
P – patient, population, or problem
• Patients who underwent primary DB ACLR • Problem: patients with a grade 2 pivot shift or greater, participation in pivoting contact sports, and side-to-side difference >10 mm.
I - intervention
• Procedure: Anatomic DB ACLR and ALLR with an IB. • This involved using autologous semitendinosus as an anteromedial bundle and single gracilis with FiberTape as the posterolateral bundle and ALL extra-articularly. • The femoral anteromedial tunnel was prepared inside-out, and the posterolateral tunnel was drilled outside-in.
C - comparison
• Procedure: OI DB ACLR only. • This involved using autologous hamstring tendons (double-semitendinosus as the anteromedial bundle and double-gracilis as the posterolateral bundle) with both femoral and tibial tunnels created using OI drilling.
O - outcome
• Clinical Outcomes: Postoperative Lysholm and Tegner Activity Scale scores at 2 years, and knee ROM. • Radiological Outcomes: Femoral bone tunnel width and enlargement (specifically anteromedial and posterolateral bundle tunnels) at 0 and 2 years postoperatively, femoral tunnel coalescence, and femoral divergent angle.
Statistical analysis
The percentage of tunnel enlargement, average divergent angle, knee ROM, Lysholm, and Tegner Activity Scale were compared between groups using Student’s T-test. The paired T-test was used to compare the preoperative and postoperative Lysholm and Tegner Activity Scale in each group. The percentage of tunnel coalescence was compared using Pearson’s chi-square test. A p-value <0.05 was considered statistically significant. We evaluated the effect sizes of the Lysholm score, Tegner Activity Scale, tibial and femoral tunnel enlargement, as well as the divergent angle, in the context of the ALLR group compared to the non-ALLR group. To quantify the effect sizes, we utilized Cohen’s d calculations, wherein an effect size of 0.2 was defined as indicating a small effect, 0.5 as indicating a medium effect, and 0.8 as indicating a large effect.
Results
Patient demographics
Eighty patients were initially enrolled, while 67 patients (ALLR group, n = 34; and non-ALLR group, n = 33) (Figure 6) were finally included. Patients in the ALLR group who received anatomic DB ACLR and ALLR with IB were recruited after 2019 because the surgical technique
16
was developed after that. Demographic data are illustrated in Table 1. Only the sex ratio and initial tunnel drilling size of the femoral AM and PL bundles were significantly different between groups (Table 1). Study flowchart. ACL: anterior cruciate ligament; ALLR: anterolateral ligament reconstruction. Patient demographics.
a
ALLR: anterolateral ligament reconstruction; MM: medial meniscus; LM: lateral meniscus. aValues are presented as n, (%), or mean ± SD.

Clinical outcomes
Intra-group and inter-group comparison of pre- and postoperative Lysholm and Tegner activity scale between the ALLR and non-ALLR groups.

ALLR: anterolateral ligament reconstruction; Pre-OP: preoperative; and Post-OP: postoperative.
*p < 0.05.
*Paired T-test.
**Student T-test.
Radiographic results
Comparison of the percentage of tunnel enlargement in the femur between the ALLR and non-ALLR groups at 2-year follow-up.

ALLR: anterolateral ligament reconstruction; AM: anteromedial; PL: posterolateral.
Comparison of the average of the divergent angle and percentage of tunnel coalescence between the ALLR and non-ALLR groups at 0-month and 2-year follow-up.

ALLR: anterolateral ligament reconstruction.
Discussion
In this study, our hypothesis was approved that DB ACLR and ALLR with IB yielded less femoral posterolateral bundle tunnel widening than OI DB ACLR without ALLR. Both techniques provided good postoperative clinical outcomes. DB ACLR with ALLR and IB also provided a more femoral divergent angle when compared to the non-ALLR group. Incorporating ALLR and IB may benefit patients undergoing DB ACLR.
Many surgical techniques with different fixation devices have been proposed to achieve DB ACLR.21,22 In our study, the difference between groups was that the ALLR group had a higher divergent angle between the femoral AM and PL tunnels because of different drilling techniques. The advantage of this divergence could prevent the potential risk of intraoperative femoral AM and PL tunnel connection and the postoperative tunnel coalescence caused by tunnel enlargement. 23 According to our demographic data, 93.9% of patients in the non-ALLR group were male because the relatively smaller femoral ACL footprint in women discouraged the surgeon from choosing DB ACLR for female patients in the past. With the newly developed DB ACLR and ALLR technique, 16 52.9% of male patients and 41.7% of female patients had successfully tunnel drilling without coalescence during the surgery because of more divergent angle between AM and PL femoral tunnels, precluding femoral tunnel coalescence.
As for femoral tunnel widening, the percentage of tunnel enlargement of the AM and PL tunnels in the literature was 7.1%–54% and 0.4%–42%, respectively.24,25 They were only 6.7% and 0.7% in the ALLR group and 11% and 9.65% in the non-ALLR group in our study. The significant difference (p = 0.021) in femoral PL tunnel widening between groups might be attributed to increased rotational stability and load sharing of the combination of DB ACR and ALLR. 26 This result echoed the concept that the isolated ACLR does not restore normal kinematics and biomechanics of the knee, especially for rotational stability 18
Bone tunnel coalescence is a multifactorial issue and is considered a potential risk that compromises ACLR laxity. 27 Kawaguchi et al. 28 had no femoral tunnel communication, but 12.8% of tibial tunnel communication. Kiekara et al. 29 presented femoral and tibial tunnel communication rates of 10% and 27%, respectively. Lehmann et al. 30 reported that 67% of bone bridges broke. Intraoperative communication of the tunnel was caused mainly by drilling, 27 the engagement of interference screw, 30 and the insufficient distance of the bone bridge and divergent angle. 31 Postoperative tunnel coalescence was caused by tunnel widening. For intraoperative tunnel coalescence, the volume of the interference screw dilates the diameter of the tunnel surrounded by cancellous bone, resulting in 67% of bridges breaking in the femoral tunnel. 30 Therefore, we used a cortical suspensory system for femoral AM tunnel fixation to lower the risk of tunnel coalescence in the ALLR group. Furthermore, the thickness of the sparing bone bridge of at least 2 mm was considered to prevent tunnel coalescence. However, in patients with a small ACL footprint, the 2-mm-apart rule will make DB ACLR difficult and might compromise the thickness of the bone bridge in between. We noticed that the creation of divergent AM and PL tunnels did not alter clinical outcomes, even when the intra-articular aperture was overlapped because the two tunnels were in different trajectories. 32 In our study, the divergent angle was 30.8 ± 12.8 in the ALLR group, which was significantly larger than that in the non-ALLR group (p < 0.01). This suggests that a high divergent angle might bypass the problems of a small ACL footprint and reduce the risk of tunnel communication owing to the different tunnel trajectories. The 2-mm-apart rule might be unnecessary when using this technique in the ALLR group. This provided more flexibility during femoral tunnel preparation.
This study has some limitations. First, we lacked a 2-year CT/MRI follow-up to evaluate the healing condition of the reconstructed ACL, ALL, and tunnel widening. Most of our patients returned to full sports activity at the final follow-up, and it is not rational to arrange further imaging studies only for research in the authors’ insurance system, even though they are recognized as the gold standard for the evaluation of tunnel position and widening. Second, no biomechanical study has yet compared DB ACLR and ALLR with IB, and OI DB ACLR, 33 especially when two femoral and two tibial tunnels were created in the non-ALLR group, while two femoral and one shared tibial tunnel in the non-ALLR group.
Conclusion
DB ACLR with ALLR and IB yielded less femoral posterolateral bundle tunnel widening, no femoral tunnel coalescence, and more femoral divergent angle than OI DB ACLR. Both techniques provided good postoperative outcomes. Incorporating ALLR and IB may benefit patients undergoing DB ACLR.
Footnotes
Author contributions
CW wrote the manuscript and performed the clinical and radiological assessment of the patients. LH helped with the clinical assessment of the patients. PC performed the statistics. CY and HS provided professional opinions regarding ACL reconstruction. JC provided all study cases and reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully thank Department of Orthopedic Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan, CMRPG5K0092, CMRPG3M2032, CLRPG3D0045, CMRPG5K021, SMRPG3N0011, SMRPG3P0011; Minister of Science and Technology, Taiwan, MOST 111-2628-B-182A-016, NSTC112-2628-B-182A-002-.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Chang Gung Medical Foundation Institutional Review Board, IRB 202100829B0, approved on 15 June 2021. (Chairman of the ethics committee, Tsang-Tang Hsieh, MD). All methods were performed in accordance with the relevant guidelines and regulations.
Data Availability Statement
The details of the data can be found in the Chang Gung Memorial Hospital Database. The point of contact is the corresponding author (Joe Chih-Hao Chiu MD, PhD).