
Abstract
Introduction
Proximal tibia osteotomy has advanced with various techniques, such as dome and modified oblique osteotomies, to correct angular deformities and redistribute knee stress, thereby slowing arthritic progression. Despite advancements, a gap remains in understanding the biomechanical strengths of these techniques, especially concerning correction angles. The study aims to compare the stability of the construct for different degrees of osteotomy.
Materials and methods
Eighteen synthetic tibias were osteotomised based on the dome and modified oblique osteotomy technique. For dome osteotomy, the osteotomy site was fixed with two Kirschner wires 2.0 mm for different degrees of osteotomy, which were 10o, 20o, and 30o. Three samples from each construct were tested for rotational force. For modified osteotomy, two screws 3.5 mm were used to fix the osteotomy site and tested for rotational forces.
Results
The constructs were stiffest at ten degrees for rotational force, both in dome and modified oblique osteotomy (0.39 Nmm and 0.4 Nmm). The stiffness of dome osteotomy in correction angles of 10° and 20° is almost similar (p > 0.95), and it reduces significantly at 30°(p < 0.001). There were significant differences in stiffness of the oblique osteotomy construct when comparing 10° with 20° (p = 0.003), 10° with 30°(p < 0.001) and 20° with 30° (p < 0.001) correction angles. This is further proved by comparing the means of stiffness between the two methods, where dome osteotomy did better compared to modified oblique osteotomy at 20° and similar at 10°.
Conclusion
In performing proximal tibia osteotomy, we recommend limiting the acute angle of correction to 20°, and we suggest that for a larger correction angle, dome osteotomy exhibits better biomechanical stiffness. An angle exceeding 30o will predispose to higher rate of non-union or malunion as the stiffness of the surgical construct drops significantly, making it less resistant to rotational forces.
Introduction
In the field of orthopaedic surgery, the evolution of surgical techniques to correct deformities and alleviate associated pain has been marked by significant advancements. Among these, proximal tibia osteotomy has evolved over decades as an important procedure to correct angular deformity in multiple conditions such as rickets, poliomyelitis, medial knee arthrosis, blount disease and post-traumatic malalignment. 1 This surgical intervention, aimed at realigning the knee joint, seeks to redistribute mechanical stress away from the damaged compartment, thereby reducing the medial compartment knee pain, hence slowing down the arthritic progression. 2 Several surgical techniques, such as open or closed wedge, dome, “en chevron,” and modified oblique osteotomy, have been developed with the same goal: to diminish the load and contact area on the medial compartment by shifting the mechanical axis to the centre of or lateral to the joint. 3 Nonetheless, the biomechanical integrity of the osteotomy remains vital, as it determines the success of the corrective surgery, influencing both the immediate recovery process and the long-term outcomes of the patients.
Recent studies have particularly focused on the dome and modified oblique osteotomy techniques, each known for its unique advantages and applicability based on the specific clinical scenario and correction requirements. The biomechanical stability provided by these techniques is vital, as it directly impacts the patient’s post-operative recovery and the long-term durability of the correction. 4
Despite the wealth of knowledge accumulated over the years, there are remains a gap in the comprehensive understanding of the biomechanical strengths associated with each osteotomy technique, especially when considering varying degrees of correction angles. This gap presents an important problem, as the lack of definitive guidance on the optimal technique and correction angle may lead to suboptimal outcomes, including compromised biomechanical stability or increased risk of post-operative complications. 5
The biomechanical study is important in orthopaedic fields as it can suggest which construct is better in terms of stability. These biomechanical studies help surgeons understand the distribution of forces across the knee, which is essential for optimizing surgical outcomes and enhancing the longevity of the osteotomy. 6 Understanding the biomechanical implications allows surgeons to make precise adjustments in the surgical technique, such as the angle and location of the osteotomy, to achieve the desired correction and stability.
The evidence of osteotomy for Blount disease is relatively scarce and most of them are limited to case reports or retrospective studies,7,8 which is understandable given that the incidence of Blount disease is rare. However, understanding the biomechanical properties and management of these deformities remains crucial. Furthermore, exploring varying degrees of osteotomy is essential, as different correction angles can significantly impact construct stability. Failure to address these variations may result in potential complications, including diminished stability and higher risks of non-union or malunion, ultimately compromising surgical outcomes and patients’ quality of life. 5 Hence this study is conducted with the objective to assess the biomechanical strength, as indicated by stiffness, against rotational force across varying degrees of osteotomy for the two most common osteotomy techniques done which are the dome and modified oblique osteotomy of the proximal tibia.
By elucidating the relationship between the osteotomy technique, the degree of correction angles, and the resultant biomechanical strength, this research aims to inform clinical decision-making, ultimately enhancing surgical outcomes and patients’ quality of life.
Methodology
The study conducted was a biomechanical analysis to evaluate the fixation stiffness on artificial tibia bones, simulating the treatment of tibial deformity (genu varum) in paediatric patients with Blount’s disease.
The experiment was performed in: i. Orthopaedic Research Laboratory of the International Islamic University of Malaysia (IIUM), Jalan Hospital Campus, Kuantan, Malaysia (for bone cutting and fixation). ii. Sultan Ahmad Shah Medical Centre @ IIUM (SASMEC@IIUM), , Kuantan (for bone cutting and fixation). iii. Mechanical Engineering Laboratory of University Malaysia Pahang Al-Sultan Abdulah (UMPSA), Gambang (for torsional force testing).
Summary of synthetic bones label, configuration of fixations, and types of forces used in the biomechanical tests.

Proximal tibia osteotomy and fixation
The dome osteotomy and subsequent fixation were done. Initially, a dome-shaped cut was outlined on the anterior surface of the proximal tibia, with the apex located 1 cm below the tibial tuberosity. The apex of the osteotomy site, located 1 cm below the tibial tuberosity, was marked with a drill hole with a diameter of 3.5 mm. Additional drill holes were placed medially and laterally in a semi-circular pattern, ensuring that the concavity of the dome faced the adjacent joint (Figure 1(a)). Using a small osteotome, these drill holes were then connected to complete the dome osteotomy. Subsequently, the metaphyseal-diaphyseal angle was adjusted to 10°, 20°, and 30° measured using goniometer in each sample in this arm (Figure 1(c)). Then the osteotomy site was fixed with two 2.0 mm cross K-wires (Figure 1(b)) Stepwise demonstration of dome osteotomy using a synthetic tibia bone model, (a) marking of a dome-shaped osteotomy on the anterior surface of the proximal tibia, (b) fixation of the osteotomy using two 2.0 mm cross K-wires following alignment and (c) final fixation position at 10° metaphyseal-diaphyseal angulation to simulate deformity correction.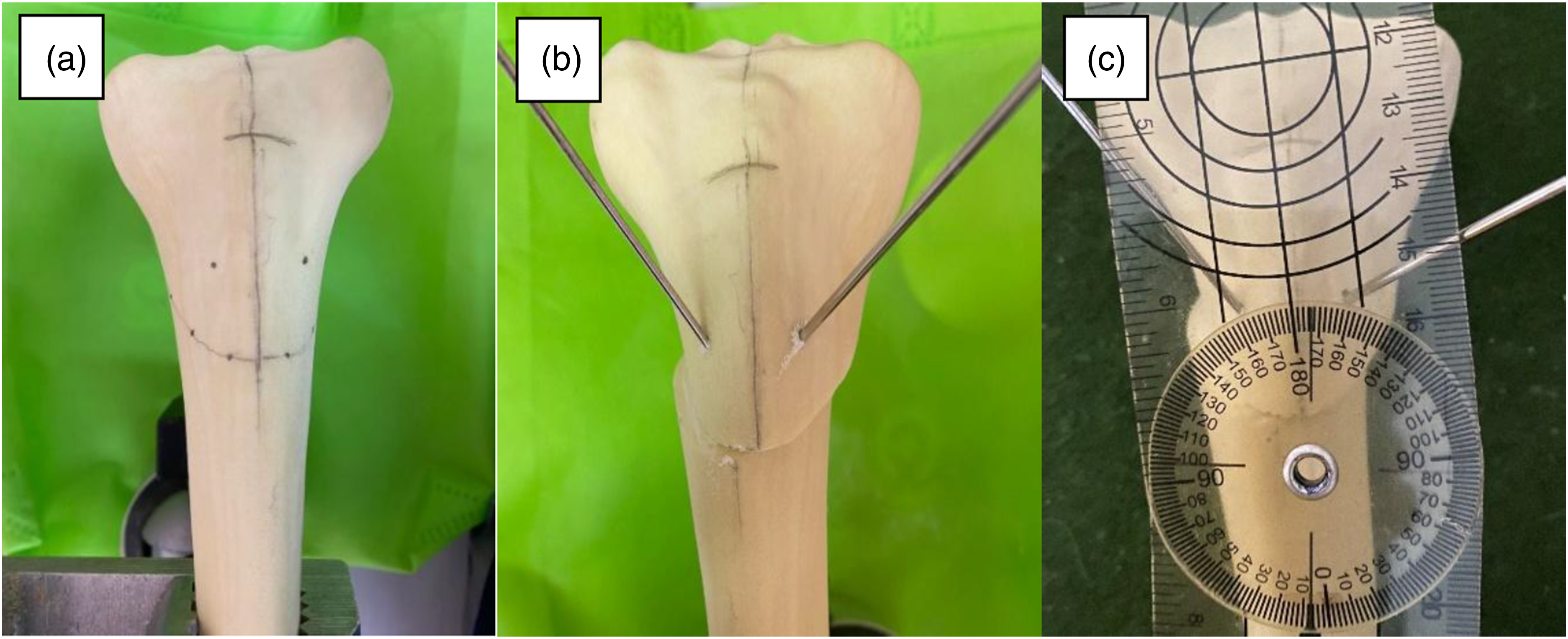
The modified oblique osteotomy and fixation were then performed. Initially, a guide pin (K-wire) was inserted 1 cm distal to the tibial tubercle and directed toward the posterior cortex at a 45° angle. A power saw was used to osteotomize the tibia distal to the pin. The saw was penetrated deep into the bone, with an angle of about 45° upward direction (Figure 2(a)) until the osteotomy was completed. Subsequently, the metaphyseal diaphyseal angle will be adjusted to 10° (Figure 2(b)), 20°, and 30° in each specimen in this arm. Two cortical screws inserted from the anterior-posterior direction were used to fix the osteotomy site (Figure 2(c)). Stepwise demonstration of modified oblique osteotomy using a synthetic tibia bone model, (a) osteotomy done at 45° obliquely, (b) modified oblique osteotomy at 10° and (c) anterior-posterior screw direction for oblique osteotomy.
Biomechanical testing
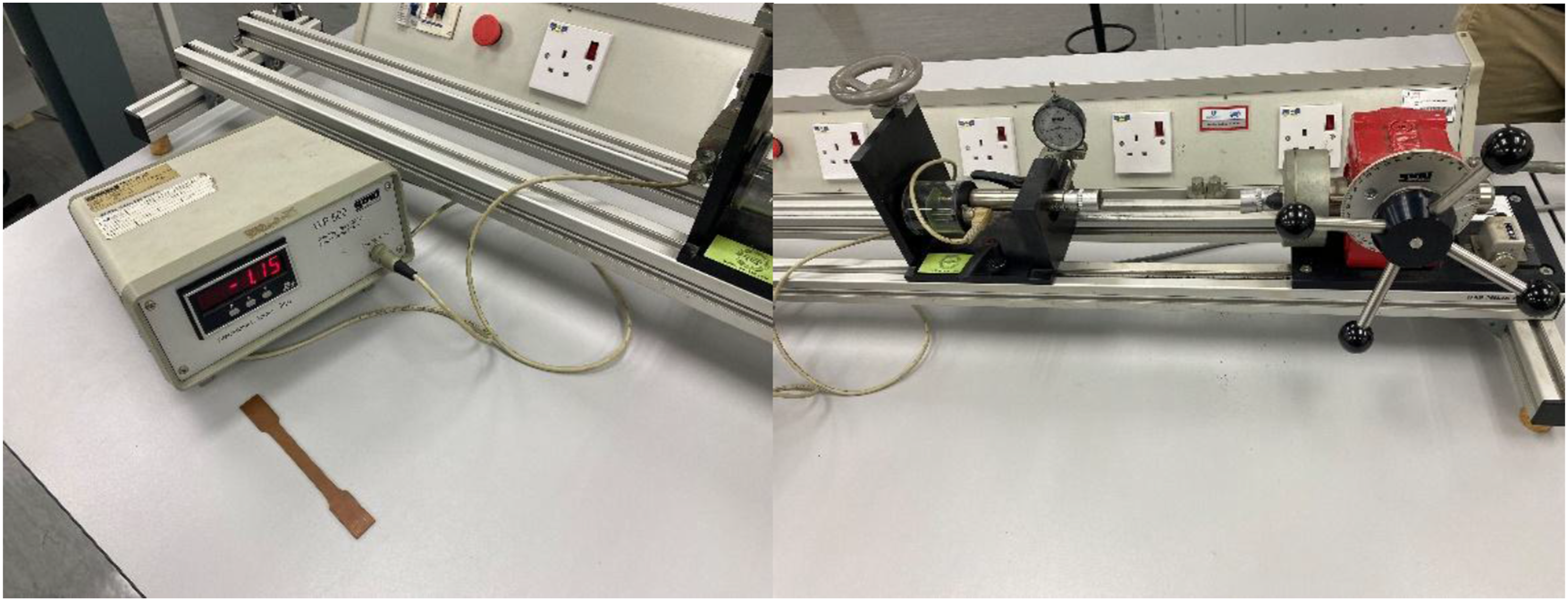
To ensure uniform force transmission through the bone samples and to prevent displacement during testing, the samples were securely clamped at the proximal and distal ends using a tibia clamp (Figure 3). The prepared bone samples were mounted horizontally into a WP500 Torsion Testing Apparatus (GUNT Hamburg Geratebau GmbH, Barsbuttel) machine designed to impose torsional forces. This position of the construct in the testing system was to simulate the natural loading conditions accurately. A reference point was marked on the tibia across the osteotomy site to facilitate precise measurement of displacement during the testing (Figure 4). The torsional force was applied to each sample using the machine (Figure 5). This force induced a rotational motion, creating a twisting deformation in the synthetic bone. The setup ensured that the applied torsional force and the resulting shear stress were uniformly distributed across the osteotomy site. The tibia clamp used to secure the synthetic tibia bone model. Reference point marking for displacement measurement across the osteotomy site. The machine used to exert torsional force in the study.

In the initial step, a preload of 50 N was applied. The distance between two reference points was measured before commencing the test. The load was then applied incrementally from 100 N to 1000 N, increasing by 100 N each time. After each increment, the distance across the osteotomy site at the reference points was measured using a digital microcaliper. The test was concluded either when the load reached 1000 N or when the point of failure was observed. The point of failure was defined by a 2.00 mm gap between the reference point, implant pull out, or implant break.
Data management and analysis
All data were entered and managed using IBM SPSS Statistics version 27.0 Descriptive statistics were presented in means and standard deviations, and frequency distributions where appropriate. Inferential analysis was performed using one-way Analysis of Variance (ANOVA) to determine the presence of statistically significant differences in the mean point of failure across varying degrees of angulation (10°, 20°, and 30°) and between different types of osteotomy techniques. A p-value of less than 0.05 was considered statistically significant (Supplemental Material).
Results
This study involved 18 synthetic tibia bones, with 9 each tested for modified oblique osteotomy and dome osteotomy. Each osteotomy group included 3 bones for each correction angle of 10 o, 20 o, and 30o.
Descriptive analysis
Descriptive analysis of stiffness measurements for modified oblique and dome osteotomies at varying degrees of angulation.

For the dome osteotomies corrected to 10°, the mean stiffness was 0.400 (±0.010) Nmm. At a correction angle of 20°, the mean stiffness slightly increased to 0.403 (±0.006) Nmm. However, when the correction angle was increased to 30°, the mean stiffness significantly decreased to 0.243 (±0.012) Nmm. These results indicate that the biomechanical stability of the dome osteotomy construct is maintained up to 20° of correction, but it markedly decreases at 30° of correction.
Inferential analysis
Comparison of stiffness differences between degrees of correction in modified oblique osteotomy.

Statistical analysis: One-way ANOVA followed by pairwise comparison with 95% confidence interval adjustment by Bonferroni correction. Assumptions of normality and homogeneity of variances were checked and fulfilled. *Statistically significant at α = 0.05.
Comparison of stiffness differences between degrees of correction in dome osteotomy.
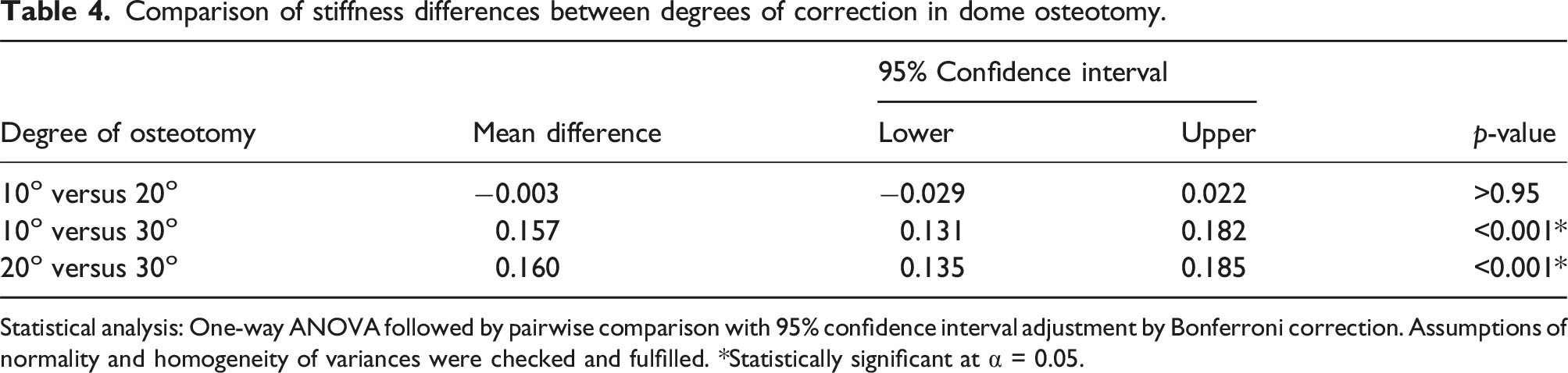
Statistical analysis: One-way ANOVA followed by pairwise comparison with 95% confidence interval adjustment by Bonferroni correction. Assumptions of normality and homogeneity of variances were checked and fulfilled. *Statistically significant at α = 0.05.
For dome osteotomy, the comparison between 10° and 20° corrections shows no significant difference in stiffness between these two correction angles. In contrast, the comparison between 10° and 30° corrections reveals a significant mean difference in stiffness of 0.157 (95% CI: 0.131 to 0.182, p < 0.001), suggesting a substantial reduction in stiffness when moving from a 10° to a 30° correction. Similarly, the comparison between 20° and 30° corrections shows a significant mean difference of 0.160 (95% CI: 0.135 to 0.185, p < 0.001), indicating a marked decrease in stiffness between the 20° and 30° corrections. Overall, the data demonstrate that while there is no significant stiffness difference between 10° and 20°, there is a significant reduction in stiffness at the 30° correction angle compared to both 10° and 20°.
Comparison of stiffness between modified oblique and dome osteotomies at specified angulation degrees.

Statistical analysis: One-way ANOVA followed by pairwise comparison with 95% confidence interval adjustment by Bonferroni correction. Assumptions of normality and homogeneity of variances were checked and fulfilled. *Statistically significant at α = 0.05.
In the oblique osteotomy group, there were significant statistical differences in terms of stiffness between all angles of correction. In the dome osteotomy group, there is no statistical difference in terms of stiffness in the angle of correction of 10° when compare to 20° correction; however, there was a significant statistical difference in mean when compared to stiffness in 20° and 30° angle of correction. When comparing two methods, at a 10° angle, there was no significant difference in stiffness in both groups. While at 20° and 30° angles, there were significant differences in stiffness between both two groups.
Discussion
Proximal tibia osteotomy is a surgical procedure used in orthopaedics to realign tibia bones that have undergone malformation or deformity due to various conditions such as developmental disorders, metabolic bone diseases, trauma, or acquired deformities. In Blount’s disease, proximal tibia osteotomy was one of the mainstay treatments, especially in adolescent Blount’s disease. 3 Fixation stability plays a critical role in the success of corrective osteotomies, ensuring proper alignment and promoting optimal healing. Stable fixation not only supports early mobilisation but also reduces the risk of complications such as non-union or malunion, which can compromise the functional outcome of the procedure. 10 Thus, achieving fixation stability through appropriate surgical techniques is paramount in ensuring the success of corrective osteotomies in orthopaedic surgery.
This study described the biomechanical strength of dome osteotomy and modified oblique osteotomy techniques of the proximal tibia across varying degrees of osteotomy against applied rotational force. The strongest biomechanical strength was determined by identifying the highest torsional force that each fixation technique could withstand before failure.
The modified oblique osteotomy’s results indicate that the greatest biomechanical strength occurs at a 10° corrective osteotomy angle, demonstrating a mean stiffness of 0.393 Nmm. As the corrective angle increases, stiffness decreases. This trend is supported by the result which showed statistically significant mean differences in stiffness reduction across varying degrees of corrective osteotomy. These findings align with previous studies that demonstrate a similar relationship between osteotomy angle and biomechanical outcomes in orthopaedic surgery, suggesting that the proximal tibia osteotomy angle should be less than 15°. Larger correction angles result in increased gaps at the osteotomy site, potentially compromising stability. 11 This evidence supports that the larger the degree of corrective osteotomy (in this study, more than 10°), the more it may affect the stability of the construct evidenced by a significant decrease in stiffness. Thus, for modified oblique osteotomy, we suggest that if the degree of osteotomy required for correction is more than 10°, extra precaution may be needed to immobilise the osteotomy site. The application of a cast post-osteotomy will help to provide external stability at the osteotomy site. 12
With regards to dome osteotomy, our results showed that dome osteotomy corrected to 10° exhibited a mean stiffness of 0.400 ± 0.010 Nmm, with a non-significant difference increase to 0.403 ± 0.006 Nmm at 20° correction (p > 0.95). However, a significant decrease in mean stiffness to 0.243 ± 0.012 Nmm was observed at a 30° correction angle. These findings suggest that while corrections up to 20° maintain comparable stiffness, whereas a 30° correction angle markedly compromises the biomechanical stability. These statistically significant findings suggested that the critical threshold of more than 20° may affect the biomechanical stability of the fixation. However, these results were slightly different from the literature, which indicates that smaller correction angles of 10° or less are more favourable for maintaining structural integrity in dome osteotomy. 13 This difference may be attributed to the variation in implants used for dome and oblique osteotomies. In the dome osteotomy, K-wires were utilised, while screw fixation was employed for the oblique osteotomy. This factor, which was not accounted for in the study, may have contributed to the discrepancy in results.
These findings are further supported by the comparison of mean stiffness values between the two osteotomy techniques. The dome osteotomy demonstrated superior stiffness compared to the modified oblique osteotomy at both 10° and 20°. At 30°, the modified oblique osteotomy showed significantly greater stiffness than the dome osteotomy. Although the modified oblique osteotomy showed significantly better stiffness than the dome osteotomy at 30°, both techniques experienced a marked reduction in stiffness as the osteotomy angle increased. This suggests that increasing the angle of correction, regardless of technique, weakens the construct. A previous study has similarly reported that larger osteotomy angles are associated with compromised biomechanical stability. It has been recommended that proximal tibial osteotomy angles should ideally remain below 15°, as larger corrections can lead to wider gaps at the osteotomy site, increasing the risk of instability. 11
Our findings reinforce this principle. Both osteotomy methods showed significant reductions in stiffness at larger correction angles, indicating compromised construct stability. This supports that excessive angular correction may increase the risk of non-union or malunion due to insufficient mechanical support. Therefore, acute correction is not recommended when the deformity exceeds 20°.
In comparison between dome osteotomy and modified oblique osteotomy, based on our results, dome osteotomy provides better stability in a higher degree of osteotomy than modified oblique osteotomy. One of the key advantages of dome proximal tibial osteotomy for larger corrections is its uniform load distribution. The dome shape allows for a more even distribution of mechanical loads across the osteotomy site, reducing the risk of localised stress concentrations that could lead to complications such as fractures or hardware failure. 14 Additionally, the circular or dome shape of the cut provides inherent stability post-operatively, which is particularly beneficial when larger corrections are required. 15 Another advantage of dome osteotomy is its ability to achieve multiplanar corrections, such as addressing internal rotation, which is more challenging with modified oblique osteotomy. Dome osteotomy is particularly effective for correcting complex multiplanar deformities, making it a preferred option for cases involving complex deformities. 16
However, performing a dome osteotomy of the proximal tibia is a technically demanding procedure that requires meticulous pre-operative planning, precise surgical technique, and careful post-operative management. The complexity of creating a curved osteotomy, ensuring proper fixation, and managing soft tissues all contribute to the difficulty of the procedure. 17 But, when executed correctly, this technique offers significant advantages in terms of load distribution, stability, and preservation of bone stock, making it a valuable option for correcting significant angular deformities of the proximal tibia.
The strengths of this study include its detailed analysis of different osteotomy angles, providing valuable insights into the relationship between correction degree and biomechanical stability. Additionally, the use of robust statistical methods to compare stiffness across varying correction angles enhances the reliability of the findings. The study also fills a critical gap in the existing literature by specifically addressing the biomechanical implications of different correction angles, offering practical guidance for clinical decision-making in orthopaedic surgery.
In addition to the observed biomechanical changes in stiffness related to varying degrees of dome osteotomy correction angles, it is crucial to consider the comprehensive impact of other biomechanical forces on surgical outcomes. While stiffness provides valuable insights into immediate structural stability, future research should explore into how other dynamic forces, such as bending, linear, and compressive forces, interact with different correction angles. Exploring these additional biomechanical factors can provide a more holistic understanding of how varying degrees of correction influence the overall biomechanics. This comprehensive approach is essential for guiding clinical decisions regarding optimal correction angles in modified oblique and dome osteotomy procedures, aiming to balance effective correction with long-term fixation stability and functional outcomes. Additionally, future studies may further explore the relationship between correction angles and long-term clinical outcomes to refine surgical techniques and improve patient care in orthopaedic practice in real-life situations.
This study has several limitations. Firstly, the use of synthetic tibia bones may not fully replicate the biomechanical properties of natural or cadaveric bone. While cadaveric specimens would provide greater anatomical and biological fidelity, obtaining a sufficient number for standardized testing is often impractical. In contrast, synthetic tibiae are cost-effective, readily available, and exhibit reduced inter-specimen variability, making them suitable for controlled biomechanical assessments. Additionally, synthetic models are composed of composite materials designed to mimic the mechanical characteristics of natural bone, though they lack the biological complexity of living tissue.
Another limitation is the inability of synthetic bones to simulate pathological conditions such as Blount disease, which involves altered bone morphology and abnormal loading patterns. As such, the biomechanical load created in this study may not fully represent diseased bone. In this study, deformities were artificially induced at fixed angles on normal synthetic bones, unlike in clinical cases where deformities occur naturally and osteotomies aim to restore anatomical alignment. Despite these limitations, the findings provide valuable insights into the comparative biomechanical property of different osteotomy techniques for future in vivo or clinical studies.
Additionally, this study may disregard other factors that may affect fixation stability or stiffness, such as the contributions of muscles, ligaments, tendons, periosteum, and other surrounding soft tissues. These elements play an important role in real-life biomechanical scenarios by providing dynamic support and stabilisation to both fixation and knee joints. 18 By not incorporating these factors, the study may not fully represent the true biomechanical condition of the proximal tibia, thereby limiting the applicability of the results to clinical practice.
Apart from that, this study also did not specifically account for implant-related factors that may influence construct stiffness. Screw fixation generally provides greater biomechanical stability and stiffness than K-wire fixation. 19 In this study, fixation methods were applied according to common clinical practice which are K-wires for dome osteotomy, and screws for modified oblique osteotomy. As the primary objective was not to compare implant types, we recommend that future studies explore the biomechanical differences by applying both screw and K-wire fixation across different osteotomy techniques. This approach would help to better understand the influence of implant choice on construct stability.
Lastly, the manual cutting process of the bone could result in a lack of uniformity, introducing variability that might affect the consistency of results, hence influencing the outcomes of the biomechanical testing. To overcome this issue, a single operator performed all the cutting procedures. This measure aimed to enhance consistency and uniformity across all bone samples, thereby improving the reliability of the study’s findings.
Conclusions
In conclusion, this study highlights the critical importance of osteotomy angle in maintaining biomechanical stability in the correction of tibia vara. The stiffness of the modified oblique osteotomy reduced significantly when comparing the correction angles of 10°, 20°, and 30°. While the stiffness of dome osteotomy in correction angles of 10° and 20° is almost similar, it reduces significantly at 30°. This is further proved by comparing the means of stiffness between the two methods, where dome osteotomy did better compared to modified oblique osteotomy at 20° and similar at 10°. Hence, we suggest that for a larger correction angle, dome osteotomy exhibits better biomechanical stiffness. Acute correction is not recommended when the deformity exceeds 20°.
Supplemental Material
Supplemental material - Proximal tibia osteotomy: Biomechanics study of two techniques
Supplemental material for Proximal tibia osteotomy: Biomechanics study of two techniques by Nik Ahmad Fauzan Nik Wan, Nik Alyani Nik Abdul Adel, Ardilla Hanim Abdul Razak, Mohd Shukrimi Awang and Ahmad Syahrizan Sulaiman in Dementia
Footnotes
Acknowledgments
We would like to extend our sincere gratitude to the staff at the Orthopaedic Research Laboratory, IIUM and Sultan Ahmad Shah Medical Centre @ IIUM (SASMEC@IIUM) for their invaluable assistance and support throughout this research project. Furthermore, we appreciate the support and technical assistance provided by the staff at the Mechanical Engineering Laboratory of Universiti Malaysia Pahang Al-Sultan Abdullah (UMPSA), Gambang, which significantly contributed to the successful completion of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Research Management Grant, International Islamic University Malaysia (Grant no. RMCG20-025-0025).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.