
Abstract
Purpose
The primary objective of this study was to establish the anatomical landmarks intra-operatively to serve as safe zones at the wrist joint during percutaneous K-wire fixation of closed perilunate dislocation(PLD). The study then correlated the same landmarks in cadavers to look for potential neurotendinous injuries.
Methods
A cohort of 10 individuals with closed acute peri lunate dislocation underwent closed reduction and percutaneous K-wire pinning. We identified the precise locations for the K-wire entrance and the angle of trajectory for a diamond construct using prominent bone landmarks. We subsequently repeated the process on five cadaveric wrists to establish the accuracy of landmarks and safety of trajectory. We assessed the correctness of the K-wire trajectory using radiographic imaging. The five cadaveric wrists were later dissected to determine the precise trajectory of the K-wire and ascertain whether critical structures like the superficial radial nerve, the dorsal sensory ulnar nerve and the extensor tendons were compromised during the procedure. The clinical cohort was examined for any postoperative complications related to the K-wire placement postoperatively.
Results
With well-defined anatomical landmarks and a constant angular trajectory, we could achieve the diamond construct in all the cases of acute PLD. We avoided injury to the vital structures and confirmed the safety of these landmarks with the cadaveric correlation. None of the patients exhibited any sensory loss or pain and or any finger or wrist extension deficits postoperatively.
Conclusion
The anatomical described landmarks have produced a consistent fixation pattern and would help surgeons mark the entry points with great accuracy while performing closed reduction of acute PLD.
Introduction
The conventional treatment for acute perilunate injuries involves open reduction and ligamentous repair. 1 However, treatment with closed reduction and K-wire fixation without ligament repair or reconstruction has yielded favourable results, particularly in cases of acute presentation.2,3 Intraoperatively, it is extremely difficult without a mini open incision to determine whether the percutaneous K-wire path caused any damage to soft tissue structures, such as extensor tendons, sensory branches of the radial and ulnar nerves, and radial artery branches, as no safe zones have been described for this technique. There are established safe zones for K-wire insertion into the radius for distal radius fractures. These safe zones are based on anatomical landmarks and aim to minimize the risk of injury to extensor tendons and branches of the superficial radial nerve during the procedure. 4 In a cadaveric study to better define the clinical anatomy of the radial aspect of the wrist, Steinberg et al. identified a consistent safe zone in the anatomical snuff box for K-wire insertion into the carpal bones (scapholunate and scaphocapitate) and radius. 5 Similarly, Naik et al., in their cadaveric study, recommended safe techniques for pinning ulnar-sided wrist structures, particularly the lunotriquetral and fifth metacarpal bases, to avoid injury to the dorsal sensory branch of the ulnar nerve. 6 The concept of the diamond K wire construct for peri-lunate dislocation has gained popularity because of the work of Özyürekoğlu and Acar, 7 which is supported by a biomechanical rationale. However, no research has identified safe landmarks and trajectories for K-wire insertion in the percutaneous reduction of acute perilunate dislocation. Our study aimed to determine the anatomical landmarks for safe zones at the wrist that could be used to pass the K-wires. Our objective was to correlate the same with landmarks in cadaveric anatomy and to look for any complications.
Methodology
To establish secure fixation of the carpal bones in closed reduction and fixation of peri lunate dislocation, the senior author devised a surgical technique that utilizes a precise sequence, orientation, and arrangement of Kirschner wire placement. After approval from our institutional ethical committee, 10 consecutive patients with acute closed perilunate dislocation underwent closed reduction and percutaneous K wire pinning under an image intensifier. Patients with pure ligamentous injury were included in the study and ones with fracture of the scaphoid/ radial styloid were excluded. Patients had no other injuries apart from a closed perilunate dislocation. Accurate landmarks for K wire entry were marked with normal bony prominences as a guiding source. The borders of the distal radius with the radial styloid, surface marking of the first extensor compartment tendons : extensor pollicis brevis, abductor pollicis longus and the extensor pollicis longus tendon, radial and the ulnar borders of the distal ulna and the ulnar styloid, and the radial and the ulnar borders of the fifth metacarpal were marked around the wrist joint (Figure 1(a)–(d)). On the radial side, the X axis is the horizontal line across the dorsum of the wrist in line with the radial styloid tip till midline. The Y axis is along the dorsal edge of the radial styloid (Figure 1(e)). On the ulnar side, the X1 axis is the line across the dorsum of the wrist in line with the ulna styloid till midline. The Y1 axis is along the dorsal edge of the ulna styloid, which continues along the ulnar border of the fifth metacarpal (Figure 1(f)). We then proceeded to the diamond configuration with the following wire trajectories and order.(Table 1) Initially the Linscheid manoeuvre with a radio lunate wire was performed to facilitate reduction and to perform the subsequent K wire fixation. Important bony landmarks (a-d) and the axes on the radial and ulnar sides of the wrist defined (e and f). Summary of K-wire entry points and trajectories in the diamond Configuration.

(a-c): Schematic illustration and the c-arm trajectory of the scapholunate wire (Wire 1).
(a-c): Schematic illustration and the c-arm trajectory of the lunotriquetral wire (Wire 2).
(a-c): Schematic illustration and the c-arm trajectory of the triquetrocapitate wire (Wire 3).
(a-c): Schematic illustration and the c-arm trajectory of the scaphocapitate wire (Wire 4).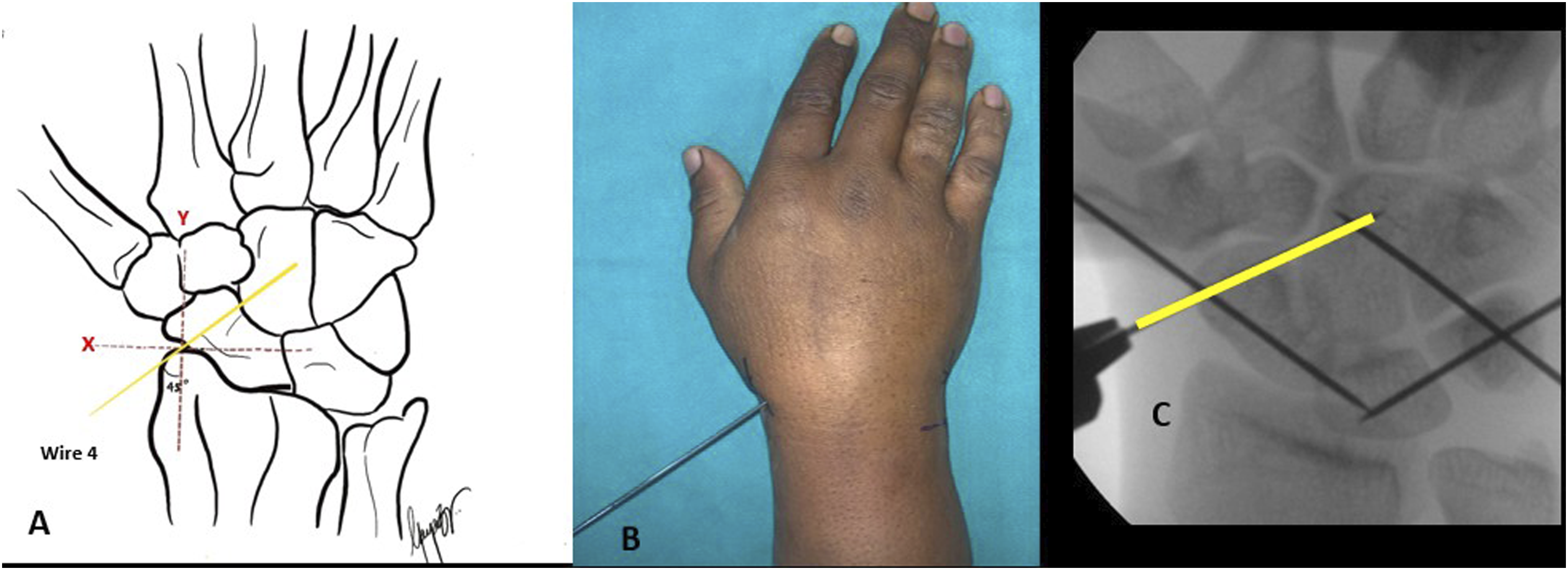
Accurate joint purchase was confirmed by visualizing the trajectory of each wire across the intended carpal joint space without extraosseous protrusion. The trajectory angle and diamond configuration was evaluated on the C arm in real time for wire orientation symmetry and convergence at the mid-carpal and radiocarpal levels (Figure 6). Particular attention was paid to the restoration of carpal alignment and the correction of any dorsal intercalated segment instability (DISI), a common sequela of perilunate injuries. (a-c): Schematic illustration and the c-arm trajectory of the diamond construct for perilunate dislocation.
We then performed the same procedure using five cadaveric wrists for correlation in accordance to the above-mentioned landmarks and trajectories. The scapholunate joint, lunotriquetral joint, scaphocapitate, and triquetrocapitate joints were percutaneously pinned using smooth 1.5 mm Kirschner wires applied with a wire driver (Figure 7(a)). The five cadaveric wrists were then radiographed to assess the accuracy of the K-wire trajectory and the purchase of the joints leading to the diamond configuration with respect to the anatomical landmarks (Figure 7(g) and (h)).We meticulously dissected the five wrists to identify the actual trajectory of the K wire and whether any structures, such as the superficial radial nerve, dorsal sensory branch of the ulnar nerve and extensor tendons, were violated during this process. The underlying anatomic structures were meticulously preserved while the skin and subcutaneous tissues were dissected (Figure 7(b)). The superficial radial sensory nerve (Figure 7(c)) and the dorsal sensory ulnar nerve (Figure 7(d)) were identified. The extensor tendons were visualized once the extensor retinaculum had been raised (Figure 7(e)). To confirm the presence of bone in the K wire trajectory, the superficial layer of the carpal bones was scraped (Figure 7(f)). The average distance from the K wires to the soft tissue structures were also measured during each of the above-mentioned steps. The clinical cohort was clinically evaluated for any neuro tendinous involvement postoperatively. (a-h): Layerwise cadaveric dissection with the identification of vital structures (a-f) and confirmation of the trajectory on imaging of the dissected wrist.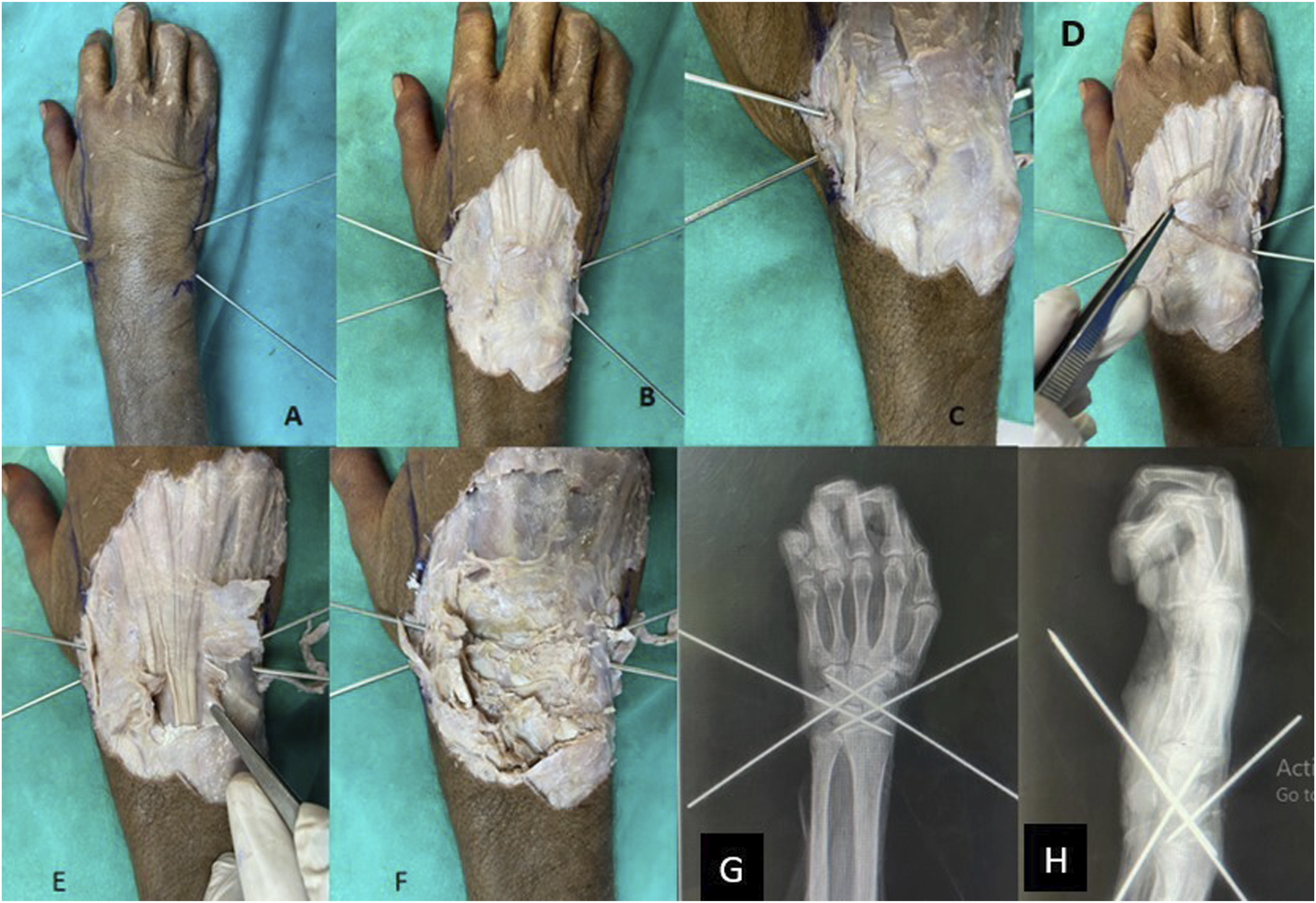
Results
Radiographs of the cadaveric wrist revealed that all five wrists had accurate K-wire trajectories leading to the diamond configuration, aligning perfectly with the anatomical landmarks in both the PA and lateral views. On cadaveric dissection, the K wires were found to spare the ulnar sensory nerve, radial sensory nerve and extensor tendons in all five wrists, where the landmarks and trajectories were followed. (Figure 7)
On the radial side, the mean distance from scapholunate wire (wire 1) to the extensor pollicis longus tendon was 0.48 ± 0.09 cm and scaphocapitate wire (wire 4) to the 1st extensor compartment muscles was 0.58 ± 0.05 cm (Figure 8(a)), and that from scaphocapitate wire( wire 4) to the main sensory branch of the radial nerve was 0.5 ± 0.08 cm (Figure 8(c)). On the ulnar side, the mean distance from triqitrocapitate wire (wire 3) to the dorsal sensory branch of the ulnar nerve was 0.45 ± 0.05 cm (Figure 8(c)), and that from lunotriquetral wire (wire 2) to the extensor digiti minimi tendon was 0.53 ± 0.09 cm (Figure 8(b)). A total of 10 patients who underwent percutaneous K wire fixation were clinically evaluated postoperatively to determine the presence of a sensory deficit in the dorsum of the hand within the sensory nerve territories of the radial and ulnar nerves as well any complications related to extensor tendon. None of the patients exhibited any sensory loss or any finger extension lag, suggesting the safety of the trajectories and the wire placements. All patients demonstrated restoration of normal carpal angles without residual DISI deformity, further supporting the radiological accuracy of this technique (a) extensor tendons on the radial side. (b) extensor tendons on the ulnar side. (c) the sensory nerves . W- K wires in the order of one to four.
Discussion
The primary treatment objective in acute perilunate dislocation is to reestablish carpal alignment, allowing the intercarpal ligaments to heal and regain stability. 8 A contentious debate exists regarding the most appropriate approach to achieve reduction and the optimal method for preserving carpal alignment in terms of closed reduction and pinning versus open reduction and ligament repair. 9 A study conducted by Inoue and Kuwahata (1997) 10 involving 14 patients evaluated the efficacy of closed reduction versus open reduction and ligamentous repair. This investigation revealed no statistically significant difference in outcomes between the two groups. 10 Percutaneous K-wire fixation following closed reduction is a highly effective approach for treating acute closed perilunate dislocation, as long as precise anatomical carpal realignment is achieved.2,3 The studies conducted by Hildebrand et al. (2000) 11 and Sotereanos et al. (1997) 12 involved the execution of perilunate dislocation treatment with a fixation technique that employed two K-wires for the fixation of both the scapholunate (SL) and lunotriquetral (LT) ligaments exclusively involving the proximal row. Most patients experienced satisfactory pain alleviation, improved functional motion, and increased grip strength following this surgery. A further investigation by Herzberg (2008) 13 and Malovic et al. (2011) 14 revealed favourable outcomes by the use of a K-wire for fixation at the proximal row and midcarpal joints. The utilization of a diamond-shaped arrangement consisting of four K-wires for the treatment of Peri lunate dislocation was initially reported in a study conducted by Bhatia D. N. (2016)15 and subsequently gained popularity through the work of Özyürekoğlu & Acar. (2021). 7 This configuration indicates the most effective stabilisation can be accomplished by using non-parallel K-wires through each bone segment, reducing dislocation and unloading adjacent rows. The design offers strength by stabilising dislocated joints in the proximal row and stabilising the proximal row against the distal carpal row. In a cadaveric study by Steinberg et al. (1995) 5 to denote safe zone on the radial side of the wrist, three percutaneous Kirschner wires were inserted into the upper extremities through the anatomic snuff box with fluoroscpic guidance. One Kirschner wire was inserted into the radial styloid, one across the scapholunate joint, and one across the scaphocapitate joint. They revealed a persistent safe zone for the insertion of K wires from the radial aspect of the wrist, with a mean area of 0.682 cm around the anatomical snuff box, bordered by branches from the superficial radial nerve, tendons forming the first dorsal compartment, the radial artery and its branches, and the radial styloid. Specific neurovascular and musculotendinous structures, including the ulnar nerve, ulnar artery, extensor digiti minimi, extensor carpi ulnaris, and flexor carpi ulnaris, are at risk for iatrogenic damage during the percutaneous pinning of ulnar-sided structures (Mok D et al., 2006). 16 A study by Naik et al. (2016) 6 demonstrated that two of the 11 ulnar styloid pins directly penetrate the distal superficial branch of the ulnar nerve (DSBUN) and that one of the 11 lunotriquetral pins directly penetrates the DSBUN. These findings highlight the potential risk of nerve injury associated with the placement of the ulnar styloid and lunotriquetral pins. However, the precise landmarks and trajectories for K wire insertion were not specified in the clinical and cadaveric studies previously discussed. While wire placement accuracy was confirmed intraoperatively and through cadaveric dissection, this study quantified safety rather than finding a “ideal” intraosseous position. Our study’s chosen landmarks and trajectories effectively avoided damage to essential structures during K-wire insertion. These findings indicate that the technique used in this study can be considered safe and reliable for future clinical applications. This may reduce the use of image intensifiers and decrease the amount of radiation exposure associated with their use.
The study’s primary shortcomings include its small sample size, its lack of a correlation between genders, and its exclusion of contributing anthropometric variables like hand size. However, the cadaveric correlation in our study offers insightful information on anatomical features, enabling a more thorough comprehension of the results. During cadaveric validation, we observed a distinct learning curve, evidenced by enhanced wire placement accuracy following the initial two specimens. As familiarity increased, the duration for wire placement decreased, and trajectory errors lessened, indicating that the method is readily teachable and reproducible with limited fluoroscopic support. Additionally, the inclusion of clinical evaluation of the patients postoperatively ensures that the study’s conclusions are supported by real-world observations and not limited to theoretical implications.More inclusive research with a larger sample size is needed to make it applicable to diverse demographic groups and a more diverse patient population. In addition, considering a potential variability in anatomical landmarks would also provide a balanced perspective. This study is the first of its kind in terms of safe anatomical landmarks for K-wire fixation of perilunate dislocation. A comparative analysis would place our findings in context and highlight the advancements our study offers over current practices. In clinical practice, reliable radiographic accuracy and the lack of iatrogenic damage further validate that the procedure may be safely implemented following initial supervised training.
Footnotes
Acknowledgement
We acknowledge Dr Anne D. Souza, Associate Professor (Anatomy), and Dr Joseph Abraham, Research Scholar (Anatomy), Kasturba Medical College, Manipal, India for facilitating the cadaveric dissection. Dr Gayathri jyotish, junior resident, Department of Hand surgery, Kasturba Medical College, Manipal for the schematic illustrations.
Author contributions
Dr Anil K Bhat: Concept, technique development, intellectual inputs, manuscript editing. Dr Mithun Pai G: Cadaver dissection, Data collection and manuscript draft. Dr Saktthi S S: Cadaver dissection and manuscript editing.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent
Written informed consent was obtained from the parents / legally authorized representatives before the study.